Case Presentation Dr Mahmoud Abu Esleih L J

Case Presentation Dr Mahmoud Abu Esleih

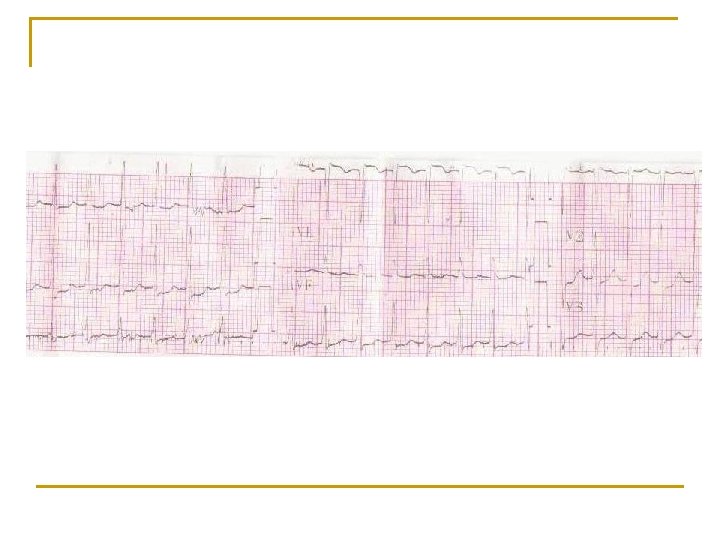
L. J. a 38 year old female patient was admitted to Thabet Hospital of Tulkarem on 19. 5 2009 with Palpitation and Tremor. The patient is pregnant (32 wks) LMP 1. 10. 2008. The patient is known to have attacks of palpitation since 2003, which were more frequent during her pregnancies. Since then she was diagnosed to have thyrotoxicosis.

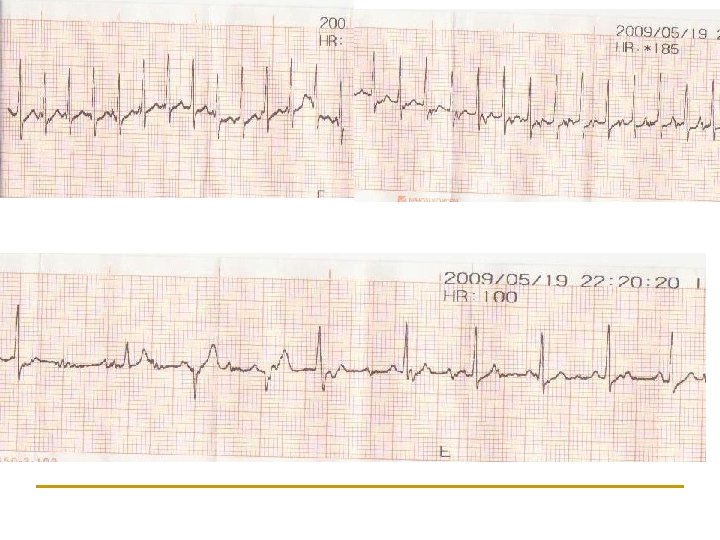
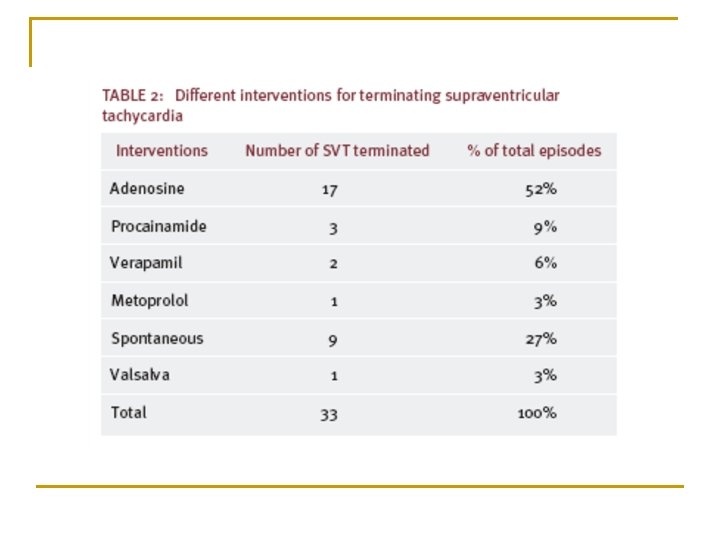
Propranolol and PTU were prescribed. She was maintained on them since 2003. In the ER she was tachycardic >180 bpm. Monitor showed narrow complex tachycardia 190 bpm. Carotid Massage was tried three times by a colleague but there was no response. She was given Verapamil 2 doses IV but there was no response.

The patient was hemodynamically stable. BP 110/60, there was no dizziness, no sweating. She was given Adenosine 6 mg but there was no response. Another carotid massage was done with relief of SVT. The patient has 2 sons and daughters. One son died with Marfan syndrome because of Aortic Arch Dissection which was operated twice.
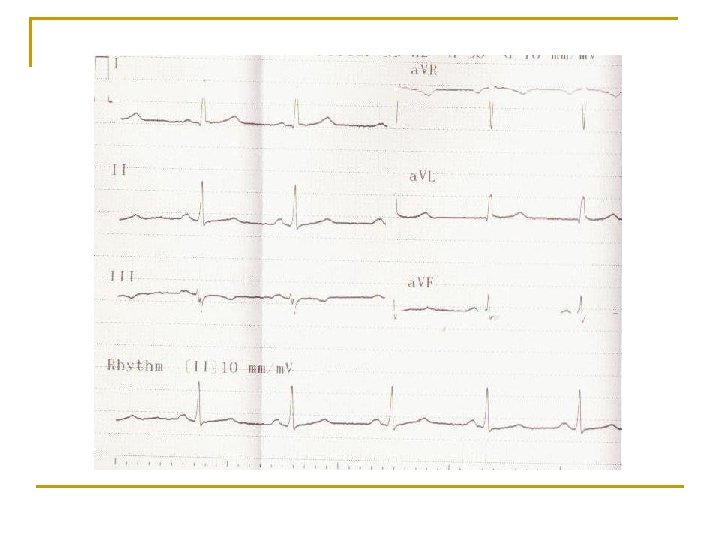

PMH was negative except for a previous CS and abortion and curettage. Hb 11. 9 g, WBC 10800, PLT 284000, BUN 15, creatinine 0. 6, RBS 103, Na 140, K 4. 7, TSH 0. 54, FT 3 2. 25, FT 4 0. 95. The second day the patient was stable and was discharged in good general condition on Propranolol and PTU.

After 1 mo she attended the Outpatient Clinic with good general condition and no palpitation with normal thyroid function. On 8. 7. 2009 the patient was admitted to the hospital with Labour Pain. Abd US showed single viable fetus. She underwent CS with good outcome. The second day after CS the patient developed an attack of SVT for which she was given Amiodarone 300 mg. TSH for the baby was 2. 73 and was repeated after 1 mo and was 2. 4

What to discuss? Physiologic Changes in pregnancy? How frequent is SVT in pregnancy? Effect of pregnancy on SVT and vice versa. Management of SVT in Pregnancy How safe are non pharmacological therapeutic procedures on the fetus? How safe are antiarrhythmics on the fetus?

How common is thyrotoxicosis in pregnancy? Diagnosis of thyrotoxicosis in pregnancy? Management of thyrotoxicosis in Pregnancy. Safety of ATD in Pregnancy. Effect of thyrotoxicosis on the fetus Effect of therapy on the fetus

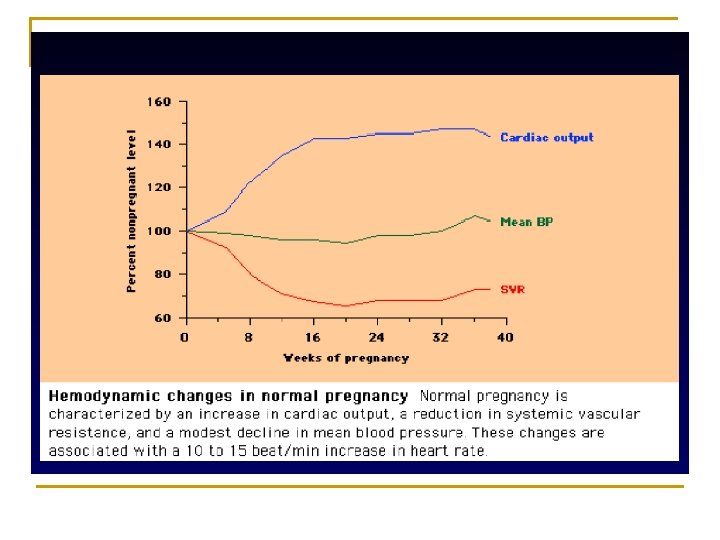
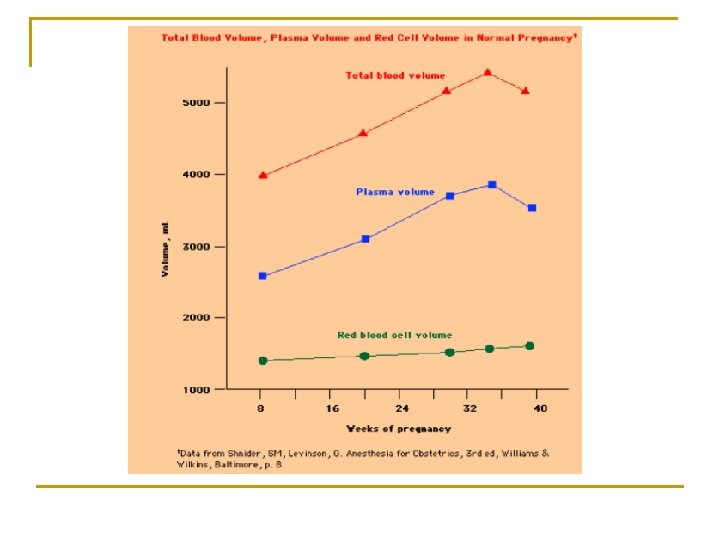
BP decreases The resting HR also increases about 10 beats per minute
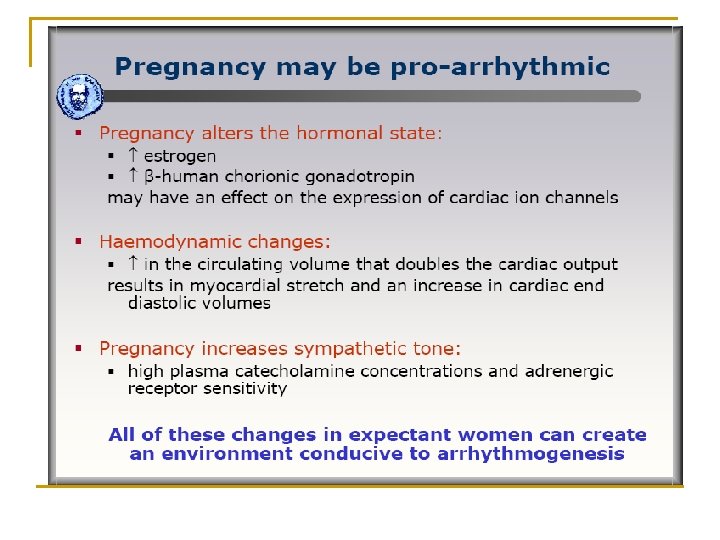

Cardiac Arrhythmias in Pregnancy Cardiac diseases complicate 1% to 4% of pregnancies in women without preexisting cardiac abnormalities. Serious cardiac arrhythmias are uncommon in pregnancy.
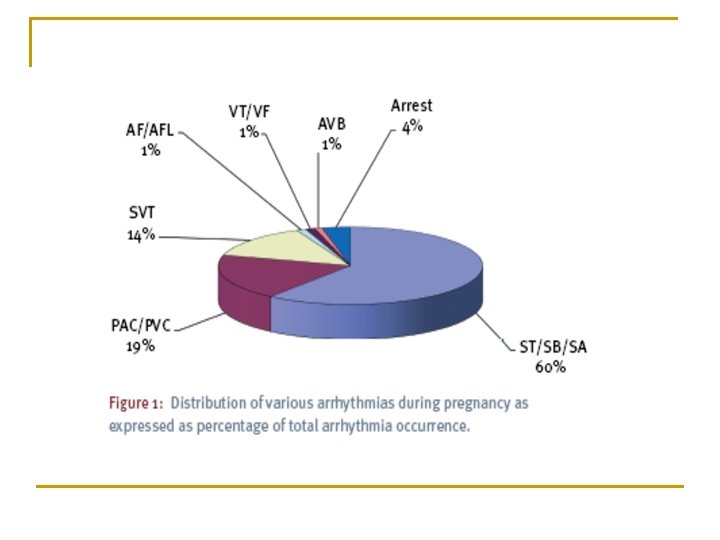

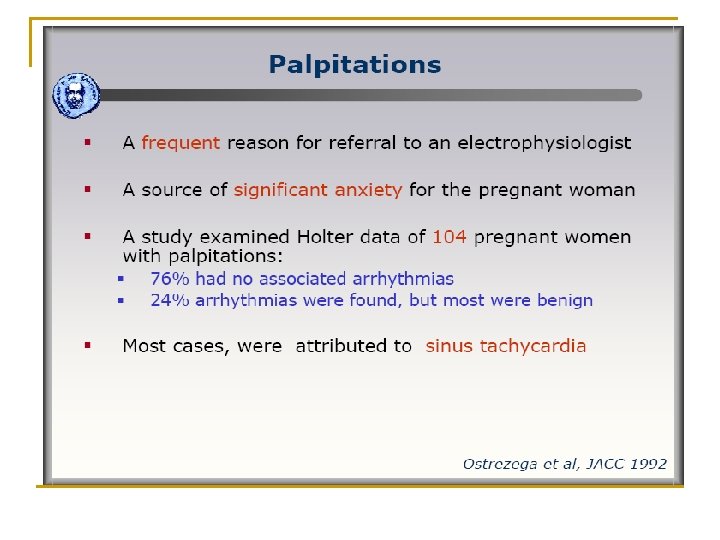
Effect of Pregnancy on SVT Pregnancy may predispose to and exacerbate symptoms of PSVT. Several case reports and a retrospective study of 60 patients with documented SVT showed pregnancy to be associated with both an increased risk, and an exacerbation of symptoms.

Clearly, both mother and fetus are at risk when SVT occurs during pregnancy. There are no maternal deaths as a result of arrhythmia reported. There is minimal information on morbidity associated with SVT in pregnancy.

However, emergency CS is often a consequence, increasing maternal risk and if pre-term, increasing fetal risk. A cardiac lesion may predispose to SVT. Congenital heart disease such as Ebstein’s anomaly.

Treatment of SVT in pregnancy may also affect the fetus Carotid massage Facial ice immersion

Direct current electrical shock has been used at all stages in pregnancy without significant complication

The amount of current reaching the fetus is thought to be negligible. However, transient fetal dysrhythmia has been described. Sanchez–Diaz et al. reported 20 cases in which electrical cardioversion was used on an emergency basis during pregnancy. All of the patients were successfully cardioverted, and no immediate adverse effects were reported.

Ueland et al. reviewed 15 cases of electrical cardioversion use in pregnancy. The cardioversion was successful in 13 of the 15 cases, using energy levels of 50 to 300 joules. One fetus developed a nonreactive heart rate tracing after cardioversion and emergency CS was subsequently performed for suspected fetal distress, which in fact was not present.

If an ICD is deemed necessary for the mother’s survival, the procedure can be considered.

Radiofrequency ablation generally requires the use of large amounts of fluoroscopy, far more than would be required for implantation of an ICD, for instance. Therefore, this procedure should virtually never be performed during pregnancy with the exception of a life-threatening arrhythmia. A case report showed no adverse effects in the fetus following an ICD discharge.

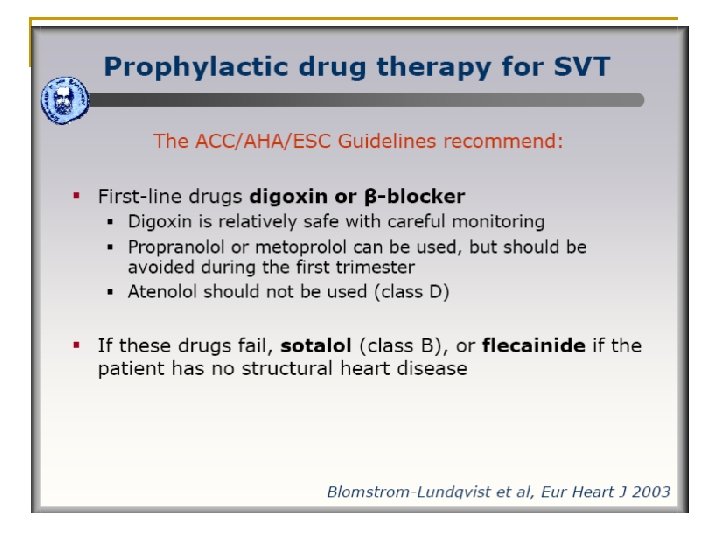
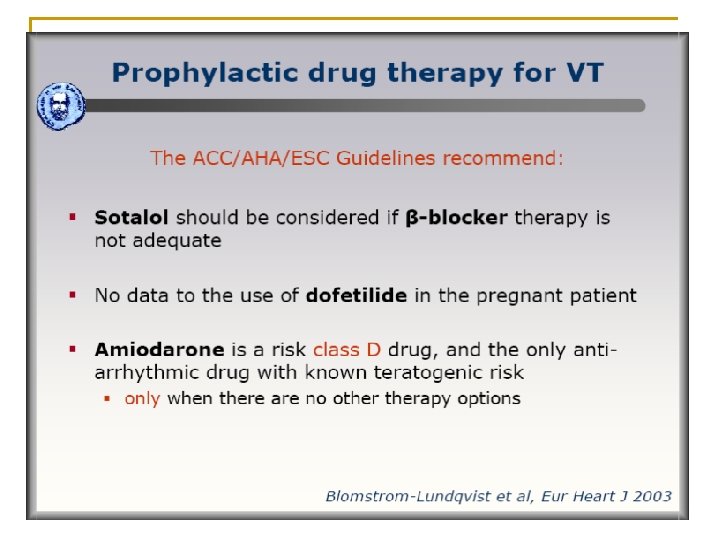
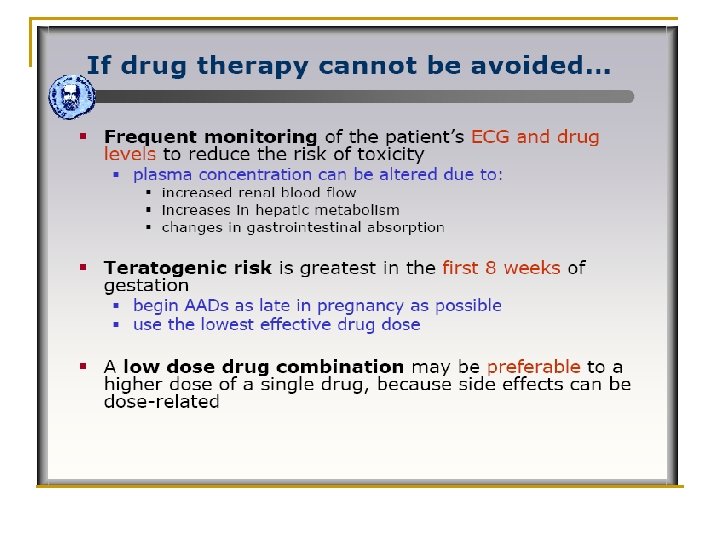
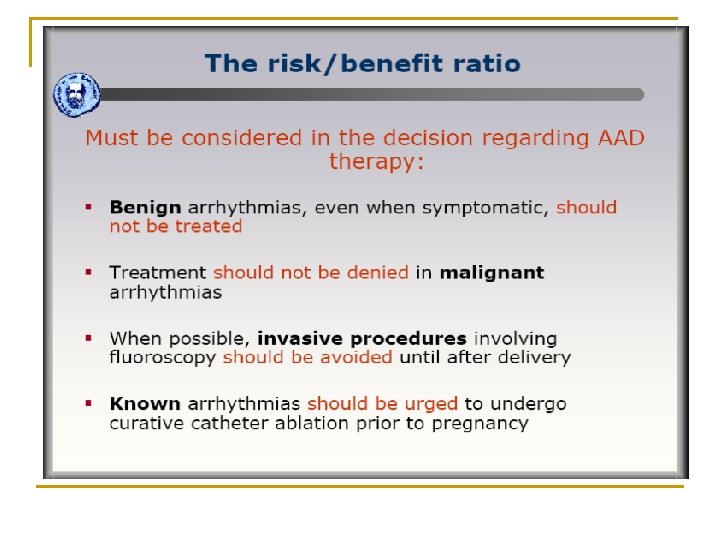
The major concern during treatment of SVT during pregnancy is the potential for adverse effects on the fetus, as all commonly used antiarrhythmic drugs cross the placental barrier to some extent.

All antiarrhythmic drugs should be regarded as potentially toxic to the fetus and should be avoided if possible, especially during the first trimester

Thyrotoxicosis in pregnancy Thyroid abnormalities affect 5 -15% of pregnant women & 4 -8% of post partum women. Hyperthyroidism occurs in 0. 2% of pregnancies Thyroid disease has adverse effects on maternal health, the course of pregnancy, and development of the fetus

Up to 60% of women with hyperemesis gravidarum have a subnormal TSH and nearly 50% have an elevated free T 4 concentration

Causes of Hyperthyroidism Grave’s disease HCG related thyrotoxicosis Toxic adenoma Toxic multinodular goitre Thyroiditis

In some women, the THX precedes the pregnancy. In others, THX begins during pregnancy, usually in the first trimester or early in the second. Relapses of THX also occur during pregnancy in women who were in remission before becoming pregnant.

Figure 2 Most frequent symptoms and signs of hyperthyroidism Because nonspecific symptoms of hyperthyroidism such as tachycardia, warm moist Vita R et skin, al. (2008) A patient with stress-related onset and exacerbations of Graves disease tremor, and systolic murmur may be mimicked by normal Nat Clin Endocrinol Metab doi: 10. 1038/ncpendmet 1006 pregnancy, the presence of. Pract classic thyroid ophthalmopathy, a significant goiter, or pretibial myxedema may point to a diagnosis of true GD. A careful PE should be performed in all patients

Diagnosis of hyperthyroidism Patients suspected of having hyperthyroidism require measurement of serum TSH, T 4, T 3 levels, and thyroid receptor antibodies. However, interpretation of TFTs must be made in relation to the h. CG-mediated decrease in serum TSH levels and the increase in TBG concentrations that occur during pregnancy.

Pregnant woman with GD Thyroid stimulating antibodies are present and cross freely the placenta.

50 percent higher than normal If the diagnosis is not established by these tests, the wisest course is continued observation.

Adverse effects of maternal hyperthyroidism: pregnancy outcome The risk of complications for both mother and fetus is related to the duration and control of maternal hyperthyroidism. Fetal and neonatal risks of maternal hyperthyroid disease are related to the disease itself and/or to the medical treatment of the disease.

Maternal complications: - Miscarriage - Infection - Preeclampsia - Preterm delivery - Congestive heart failure - Thyroid storm - Placental abruption Fetal and neonatal complications: - Prematurity - Small size for gestational age - Intrauterine fetal death - Toxemia - Fetal or neonatal THX, including accelerated bone maturation, goiter, and hydrops

THERAPEUTIC OPTIONS In managing hyperthyroidism during pregnancy, it should be remembered that two patients are being treated: the mother and the fetus. A balance must be made in optimizing treatment for one without impinging on the other.

If a subnormal serum TSH concentration is detected during gestation, hyperthyroidism must be distinguished from both normal physiology during pregnancy and HG because of the adverse effects of overt hyperthyroidism on the mother and fetus. Differentiation of GD from gestational THX is supported by evidence of autoimmunity, a goiter, and presence of TSH receptor antibodies (TRAb).

For overt hyperthyroidism due to GD or hyper-functioning thyroid nodules, ATD therapy should be either initiated (for those with new diagnoses) or adjusted (for those with a prior history) to maintain the maternal thyroid hormone levels for free T 4 in the upper nonpregnant reference range.
 drugs are considered first-line therapy. Several studies have shown no")
Antithyroid drugs Thionamide (PTU) drugs are considered first-line therapy. Several studies have shown no significant correlation between daily maternal ATD dose and fetal thyroid status. Elevation in serum TSH concentration can still be found in newborns of 23% of mothers taking low-dose PTU (100 mg daily or less) and 15% of those taking low-dose MMI (10 mg daily or less).

Until recently, it was recommended that ATD doses be individualized such that maternal serum FT 4 levels were in the upper third of or just above the normal nonpregnant reference range.

Teratogenicity No prospective studies to establish causality. Multiple case reports have associated MMI with two types of congenital anomalies: choanal or esophageal atresia, and aplasia cutis (Incidence 0. 03%). These malformations can occur as part of an ‘embryopathy’ that also includes developmental delay, hearing loss, and dysmorphic facial features. No case reports of aplasia cutis and only rare anecdotal reports of embryopathies associated with PTU ingestion.

Propranolol A useful treatment for hyperthyroid symptoms and preparation for thyroidectomy is BB, specifically with propranolol; however, continued propranolol use in pregnancy has been associated with fetal growth retardation.

Iodide has not been recommended in the treatment of hyperthyroidism during pregnancy because of its association with neonatal goiter and hypothyroidism when given in conjunction with thionamides.

Previously treated Grave’s disease May escape detection but the fetus is at risk because thyroid stimulating antibodies cross the placenta and cause fetal THX. Fetal THX may present with fetal tachycardia, IUGR, goitre, cardiomegaly, premature fusion of the cranial sutures Measure antibodies early in pregnancy & at 30 weeks. Treat fetus by giving PTU

Complications of treatment PTU & CMZ are both safe for use in pregnancy & both cross the placenta PTU & CMZ in high doses used in conjunction with T 4 can cause fetal hypothyroidism Rare but potentially lethal agranulocytosis caused by PTU

Surgery Owing to obstetric and fetal risks, surgery is not regarded as first-line therapy, but might be considered if necessary for the mother’s health. First trimester spontaneous abortions Second trimester Preoperative preparation includes ATD therapy (if not contraindicated), short-term use of iodides, and BB. THX should be controlled as best as possible to lower the risk of thyroid storm.

Surgery is reserved for patients who meet 1 of the following criteria: - High doses of ATDs (PTU > 300 mg, MMI > 20 mg) are required. - Clinical hyperthyroidism cannot be controlled. - Fetal hypothyroidism occurs at the dosage needed for maternal control. - The patient cannot tolerate ATDs (severe adverse reaction). - The patient is noncompliant. - Malignancy is suspected.

Radioactive iodine Administration of radioactive iodine for diagnostic or therapeutic purposes is contraindicated in pregnancy and lactation. After 10– 12 weeks of gestation, once the fetal thyroid has the ability to concentrate iodine, congenital hypothyroidism can occur.
 have")
Gestational Thyrotoxicosis A small percentage of pregnant women (2 percent in one survey) have transient THX during the latter part of the first trimester of pregnancy. As a group, they have few symptoms and signs of THX and no thyroid enlargement, but some have nausea, vomiting, and weight loss. The THX usually subsides in 4 to 8 weeks as CG secretion declines from its peak at 10 to 12 weeks of pregnancy.

Postpartum Thyroiditis PPT occurs in 1 to 6 percent of postpartum women of whom about half have THX. Thyrotoxicosis may occur in the first several months after delivery. Three forms of PPT are recognized: - New development of Graves' hyperthyroidism. - Recurrence of Graves' hyperthyroidism. - THX occurs as part of the syndrome of PPT. - PPT is a clinically heterogeneous disorder; some - women have only transient THX, others have transient THX followed by transient hypothyroidism, and still others have only transient hypothyroidism.
 thyroiditis, and postpartum thyroiditis.")
Schematic diagram of the course of subacute thyroiditis, painless (silent) thyroiditis, and postpartum thyroiditis. An annual TSH level should be performed in these women.

Fetal thyroid dysfunction If the mother is not treated, there is an increase in congenital anomalies and increased fetal loss resulting from spontaneous abortion and premature delivery. These are probably direct effects of maternal THX, as they do not occur in mothers who receive ATD.
 - Intrauterine growth restriction")
Suggestive findings: - Fetal tachycardia (fetal heart rate >160 bpm) - Intrauterine growth restriction - Fetal goiter - Hydrops - Advanced Bone age - Craniosynostosis - CHF

Diagnosis and screening Fetal diagnosis requires umbilical cord sampling to differentiate hyperthyroidism from hypothyroidism. In women with a past or current history of autoimmune thyroid disease, thyroid antibody values should be checked at the end of the first pregnancy. For those with positive results for TR–stimulating antibodies or those taking ATDs, fetal US should be performed at least monthly after 20 weeks of gestation. Diagnosis of FTD is challenging

Causes of FTD Treatment of FTD The risk of fetal or neonatal thyrotoxicosis is related to the mother's level of TR– stimulating antibodies. Fetal or neonatal hypothyroidism may also be due to maternal use of ATDs. FTD is treated with adjustment of maternal ATD therapy. Fetal hypothyroidism may require intraamniotic administration of T 4.

Neonatal thyroid dysfunction Neonatal THX due to persistence of maternal TRAbs occurs in about 1% of babies born to mothers with either active or previously treated GD and lasts for up to 3 months. Multiple studies have attempted to predict neonatal thyroid status using maternal antibody levels.

Baby of mother with Grave’s disease in pregnancy All newborns of mothers with GD should be evaluated for thyroid dysfunction and treated if necessary.

Cord blood should be reserved at delivery for measurement of neonatal serum TSH and either total T 4 or FT 4 levels. It has also been suggested that a hyperthyroid fetal environment might cause central congenital hypothyroidism. The incidence of central congenital hypothyroidism in these cases has been found to be about 0. 9%.

Screening Although the benefits of universal screening for hypothyroidism may not be justified by current evidence, we recommend case finding among the following groups of women at high risk for thyroid dysfunction:

1. Women with a history of hyperthyroid or hypothyroid disease, PPT, or thyroid lobectomy 2. Women with a FH of thyroid disease 3. Women with a goiter 4. Women with thyroid antibodies 5. Women with symptoms or clinical signs suggestive of thyroid Dysfunction, including anemia, elevated cholesterol, and hyponatremia

6. Women with type I DM 7. Women with other autoimmune disorders 8. Women with infertility should have screening with TSH as part of their infertility work-up. 9. Women with prior therapeutic head or neck irradiation. 10. Women with a prior history of miscarriage or preterm delivery

Targeting ATD treatment to maintain maternal serum free T 4 levels at the upper limit of the nonpregnant T 4 range usually protects the fetus from hypothyroidism. Close following of maternal T 4 and TSH levels, assay of TRAb, and fetal US including the thyroid are recommended for guiding therapy and fetal blood sampling is rarely needed.

Fetal hyperthyroidism does not occur during pregnancies in which TRAb levels are normal and ATD is not administered. Surgery may be required in some instances. PTU, propranolol, and iodides may be used for preoperative preparation.
 freely cross the placenta and can")
Fetal TRAb (either TSH receptor-stimulating or -binding antibodies) freely cross the placenta and can stimulate the fetal thyroid. These antibodies should be measured before pregnancy or by the end of the second trimester in mothers with current Graves’ disease, with a history of GD and treatment with 131 I or thyroidectomy, or with a previous neonate with GD. Women who have a negative TRAb and do not require ATD have a very low risk of fetal or neonatal thyroid dysfunction.

In women with elevated TRAb or in women treated with ATD, fetal US should be performed to look for evidence of fetal thyroid dysfunction that could include IUGR, hydrops, presence of goiter, or cardiac failure.

Umbilical blood sampling should be considered only if the diagnosis of fetal thyroid disease is not reasonably certain from the clinical data and if the information gained would change the treatment. The fetal thyroid begins concentrating iodine at 10– 12 wk gestation and is under control of fetal pituitary TSH by approximately 20 wk gestation. Fetal serum levels of TSH, TBG, free T 4, and free T 3 increase throughout gestation, reaching mean adult levels at approximately 36 wk. TSH does not cross the placenta
- Slides: 79