Ultrasound and Doppler in Obstetrics Dr Anupriya Maharshi

Ultrasound and Doppler in Obstetrics Dr Anupriya Maharshi DEPARTMENT OF OBGY MGM Medical College

Routes • Trans-abdominal – 5 MHz • Trans-vaginal – 7. 5 MHz

Timings for USG • First trimester • Anomaly scan • Third trimester scan • Specialised scans – NT scan – Targeted Fetal Echo

• First Trimester Scan

Purpose of First Trimester Scan Intra/Extra –uterine Viability Dating Number of G sacs/ embryos (singleton/multifetal gestation) • Corpus luteum • Diagnosing abnormalities • •

What features do we look for in the first trimester scan • Gestational Sac – Mean Sac Diameter or MSD (MSD in mm + 30 = gest age in days) • Yolk sac- diameter • Fetal pole –Crown Rump Length or CRL (CRL in mm + 42 +/- 3 days = gest age in days) • Cardiac activity • Corpus luteum


Gestational Sac

Yolk Sac

Fetal Pole


Location of Pregnancy

When do we call it a confirmed intrauterine pregnancy? • Gestational sac containing a yolk sac within the uterine cavity • PUL- Pregnancy of Unspecified Location

Viability

Discriminatory Levels • MSD 10 mm= 6 wks → Yolk sac should be seen • MSD 18 mm or CRL 7 mm = 7 weeks → Fetal pole and cardiac activity should be seen

Diagnostic Findings of an Early Pregnancy Loss 1. CRL > or = 7 mm and no heartbeat 2. Mean Sac Diameter (MSD) > or = 25 mm and no embryo 3. Absence of cardiac activity in an embryo 2 weeks or more after a scan that showed a gestational sac without a yolk sac 4. Absence of cardiac activity in an embryo 11 days or more after a scan that showed a gestational sac with yolk sac society of radiologist in ultrasound multispeciality panel on early first trimester diagnosis of miscarriage and exclusion of a viable intrauterine pregnancy
 • Discrepancy between")
Dating • CRL scan is most accurate (after cardiac activity appears) • Discrepancy between Menstrual dating and Sonographic dating – Till 10 weeks: discrepancy > 5 days→ reassign acc to USG – Between 10 -20 weeks: discrepancy > 10 days →reassign acc to USG

For example • By dates- → 40 weeks by USG of 8 wks- → 39. 1 wks By dates → 40. 3 wks by USG of 9 wks → 39. 6 wks by dates → 40 weeks by USG of 18 weeks → 38. 2 wks

Beyond 21 weeks , USG dating has discrepancies of > 14 -21 days

Diagnosing abnormalities • Fetal – Big G. sac, big Yolk sac, blighted Ovum , Missed abortion, sub-chorionic hemorrhage • Maternal – Adnexal masses – Ovarian cyst – Fibroid

• Second and Third Trimester Scans

Anomaly Scan- Timing • 18 -20 weeks

Anomaly Scan • • TIIFA- Targeted Imaging For Fetal Anomalies Fetal Biometry Amniotic Fluid Placentation Cervical Length Fetal presentation Cardiac activity

Anomalies to look for. . • Cranial stuctures – Lateral vetricles, choroid plexus, midline falx, cavum septum pellucidi, cerebellum, cisterna magna • Cardiac anomalies – Four chamber view, Left & Right outflow tract • • • Spinal anatomy Stomach bubble Kidneys Urinary bladder Extremities Upper lip

Second /Third Trimester USG Fetal Biometry • • Bi-parietal Diameter BPD Head Circumference HC Abdominal Circumference AC Femur Length FL
 • AFI by Four Quadrant Method Probe")
Amniotic Fluid • Single Deepest Pocket (SDP) • AFI by Four Quadrant Method Probe needs to be perpendicular to abdominal surface, cord-free & fetal part-free

Placentation • Location – Upper segment – Lower segment – distance away from os • Maturity – Grades I, III • Number of vessels and insertion site of Umbilical cord • Abnormalities

Fetal Growth Restriction • Symmetric • Asymmetric– Brain-sparing: HC , not BPD – AC affected the most. < 10 th centile – HC: AC ratio (preterm fetus ratio is >1, as pregnancy progresses , ratio approaches 1. if ratio is >1, asymmetric FGR) – EFW <10 th centile

Cervical Length • Predictor of Preterm Labor • Cut-off cervical length- 27 mm
- FGR, oligohydramnios • Rh")
Obstetric Doppler • To study fetal and placental circulations (insufficiency)- FGR, oligohydramnios • Rh isoimmunization • Cardiac evaluation • Twin pregnancy • Fetal abnormalities

Doppler Waveform Meaurements
 Ratio • Pulsatility Index- PI – Peak systolic")
Obstetric Doppler Indices • S/D (systolic/diastolic) Ratio • Pulsatility Index- PI – Peak systolic velocity – End diastolic velocity Mean velocity • Resistance Index RI
")
Uterine Artery Doppler • Non- pregnant Diastolic notch normally present (closure of aortic valve) • Disappears as pregnancy advances • Abnormal if diastolic notch persists beyond 20 weeks

Uterine Artery Doppler

Umbilical Artery Doppler • In normal fetus, Um. A a Low resistance circulation • In reduced placental perfusion & uteroplacental insufficiency → Umbilical artery impedance increases → decreased end diastolic flow → increased S/D • A rising S/D in umbilical artery is abnormal • Absent or reverse end diastolic flow is ominous

Umbilical Artery Doppler

Umbilical A Doppler- Normal Values • Normal S/D - < 2. 7 to 3 Abnormal S/D - > 3 • Normal PI - <1 Abnormal PI - >1

Middle Cerebral Artery MCA Doppler Normally , a high resistance circulation More blood flow in systolic, less in diastlolic S/D will be high ‘Brain-sparing ‘ effect → converts to a low resistance circulation→ diastolic blood flow will relatively increase→ S/D will decrease • A decreasing S/D in MCA is abnormal • •
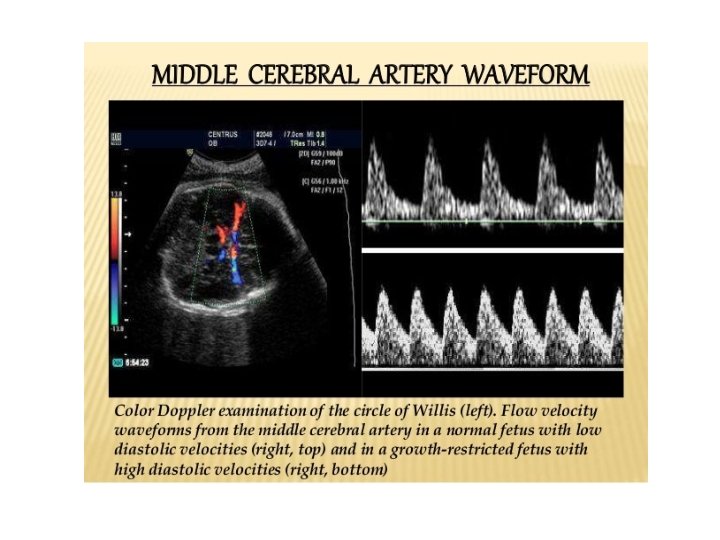

MCA Doppler – Normal Values • Normal S/D ratio 6 to 3. 5/4 Abnormal S/D ratio <3. 5 • Normal PI (Pulsatility Index) >1 to 1. 2 Abnormal PI <1

Cerebro-Placental Ratio • MCA : Um. A pulsatility index ratio • Better predictor of fetal compromise • MCA: Um. A PI ratio >1 ---- normal <1 ----abnormal

Ductus Venosus Doppler Waveform • Absence or reversal of flow during atrial contraction (a wave) (deep a wave in DV) indicates failure of fetal circulatory compensatory mechanism to supply well oxygenated blood to vital organs

Normal DV Waveform
- Slides: 43