Topic outlines Preterm birth definition incidence and etiologies

Topic outlines • Preterm birth: definition, incidence and etiologies • Prevention of preterm birth • Progesterone ▫ Mode of action ▫ Side effects ▫ Route of administration • Progesterone for prevention of preterm birth (evidence based studies) • Preterm birth prevention: guidelines or recommendations • Management of preterm labor • RTCOG 2015 recommendations
 •")
Definition • Preterm birth: delivery before 37 weeks • Extremely preterm (<28 weeks) • Very preterm (28 to <32 weeks) • Moderate preterm (32 to <37 weeks) • Late preterm: 340/7 to 366/7 weeks

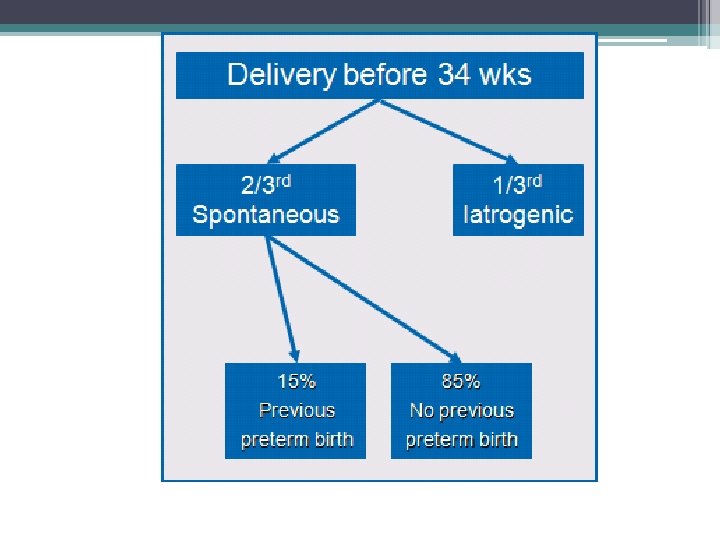
Clinical circumstances associated with preterm birth • Spontaneous preterm labor with intact membranes • Preterm PROM • Indicated preterm delivery (1/3) ▫ Maternal (e. g. pre-eclampsia) ▫ Fetal (e. g. IUGR/fetal compromise

ปจจยเสยงตอการคลอดกอนกำหนด Risk Multiple Pregnancy Previous Preterm OR/RR 57% 3. 6, 15. 830. 2% Short Cervix 2. 5 Pregnancy Interval <18 m 1. 92 OR/RR Anemia 1. 2 Hypertension 1. 2 Periodontal Disease 1. 7 Bacteriuria 2. 3, 3. 4 Vaginosis 2. 16 Premature contraction Elderly (>40 y) 1. 3 Teenage 1. 5 Lack of support, Stress Low BMI (<17 kg/m 2) 2. 4 Lack of Sleep 1. 5 Smoking 3. 21 Strenuous Work 1. 2 >3 hr. standing Work 1. 2 1. 52
 are previous preterm")
Spontaneous preterm birth • The two major important risk factors (singleton) are previous preterm birth and cervical shortening in the second trimester

Preterm birth: previous preterm birth • Recurrence risk 15 -50% • The risk depends on the number and gestational age of previous births • Women with early spontaneous preterm births are far more likely to have subsequent spontaneous preterm births

Syndromic nature of a short cervix
")
Cervical length measurement (GA 16 -24 wk)

Normal cervical length GA 14 -28 wk: a normal, bell-shaped curve • 15 mm – 2 nd centile • 20 mm – 5 th centile • 25 mm – 10 th centile • 35 mm – 50 th centile • 45 mm – 90 th centile Cervical length is not significantly affected by parity, race/ethnicity, or maternal height

Definition of short CL TVS CL; GA 16 -28 wk • ≤ 20 mm in women with no prior PTB • < 25 mm in women with a prior PTB

Risk factors of SPTB • Previous PTB • Short cervix • Multiple pregnancy

Why the United States preterm birth rate is declining The preterm birth rate in the US declined to 11. 4% in 2013, the lowest level since 1997. Reasons: • A reduced teenage birth rate • Fewer higher-order multiple births • A public policy shift to prevent nonmedically indicated births at < 39 weeks’ gestation • Smoking bans in several stages • Interventions such as progesterone supplement, and the use of cerclage in selected populations Schoen CN, et al. Decline in preterm birth. Am J Obstet Gynecol 2015; 213: 175 -80.

Strategy in the prevention of PTB Identification of risk factors 1. No prior history of PTB 2. Prior history of PTB 3. Twins (triplets) in the current pregnancy Short cervix at scan

Strategy in the prevention of PTB What is a short cervix? Risk factor No Risk factor CL <20(15) mm Prior PTB <25 mm Twins <25 mm Triplets <25 mm

Strategy in the prevention of PTB • Progesterone • Cervical cerclage • Cervical pessary

Progesterone and preterm birth prevention

“Progesterone deficient state” has been proposed to be a mechanism of disease in preterm labor

Proposed mechanisms of action reported for progesterone to prevent preterm birth • Stimulate transcription of ZEB 1 and ZEB 2, which inhibit connexin 43 (gap-junction protein that helps synchronize contractile activity) and oxytocin-receptor gene • Decrease prostaglandin synthesis, infection-mediated cytokine production (antiinflammatory effects) by fetal membranes/placenta • Changes in PR-A and PR-B expression (decreased PR-A/PR-B ratio keeps uterus quiescent) • Membrane-bound PR in myometrium • PRs, when stimulated by progesterone, help selected gene promotion, or prevent binding of other factors • Interfere with cortisol-mediated regulation of placental gene expression • Nongenomic pathways • Reduce cervical stromal degradation in cervix • Alter barrier to ascending inflammation/infection in cervix • Reduce contraction frequency in myometrium • Attenuate response to hemorrhage/inflammation in decidua • Alter estrogen synthesis in fetal membranes/placenta • Alter fetal endocrine-mediated effects

Progesterone in pregnancy maintenance • Myometrial quiescence • Inhibit cervical ripening Progesterone: a key hormone for pregnancy maintenance

Progesterone Side effects Maternal : headache, nausea, coughing, local irritation, and breast tension GDM ? Fetal: no teratogenic effects Long term effects ?
: a multicentre, randomised, double-blind trial")
Vaginal progesterone prophylaxis for preterm birth (the OPPTIMUM study): a multicentre, randomised, double-blind trial Vaginal progesterone had no harm on outcomes in children at 2 years of age (vaginal progesterone = 430 VS placebo = 439). Norman JE, et al. Vaginal progesterone prophylaxis for preterm birth (the OPPTIMUM study): a multicentre, randomised, double-blind trial. Lancet 2016 Feb 23.
 Depot proluton (17 -alphahydroxyprogesterone caproate) 250 mg/ 1 ml")
Type Dose/Route Picture Price (B) Depot proluton (17 -alphahydroxyprogesterone caproate) 250 mg/ 1 ml Ampule IM 112 Cyclogest (micronized progesterone) 200 mg, 400 mg Pessary Vagina -, 62 Utrogestan (micronized progesterone) 100 mg, 200 mg Capsule Vagina/Oral 12, 24 8% Crinone gel (micronized progesterone) 90 mg Gel Vagina 162 Duphaston (dydrogesterone) 10 mg Tablet Oral 20
")
Evidence based studies (till October 2016)

Progesterone for the prevention of preterm birth in singleton pregnancy

Conclusions • The use of progesterone is associated with benefits in infant health following administration in women considered to be at increased risk of preterm birth due either to a prior preterm birth or where a short cervix has been identified on ultrasound examination. Dodd JM, Jones L, Flenady V, Cincotta R, Crowther CA. Prenatal administration of progesterone for preventing preterm birth in women considered to be at risk of preterm birth. Cochrane Database of Systematic Reviews 2013, Issue 7.
,")
Prevention of SPTB : Which one is superior? • 17 -alpha-hydroxyprogesterone caproate (17 OHPC), vaginal progesterone, oral progesterone • Cost, compliance, side effects, adverse reactions, long term effects (mother and baby)

Singleton gestations Prior PTB 17 -OHPC Vaginal progesterone Oral progesterone 1. Johnson JW, 1975 2. Meis PJ, 2003 Short CL � 1. da Fonseca EB, 2003 (MP) 2. Majhi P, 2009 (MP capsule) 3. Maher MA, 2012 (Pgel) 1. O’Brien JM, 2007 (Pgel) 2. Norman JE, 1. Rai P, 2009 (MP) 1. Glover MM, 2011 (MP) 2016 (MP) Prior PTB + short CL � 1. Keeler SM, 2009 2. Grobman WA, 2012 1. Fonseca EB, 2007 (MP capsule) 2. Hassan SS, 2011 (Pgel) 3. Romero R, 2012 (MP, Pgel) 1. Norman JE, 1. De. Franco EA, 2007 (Pgel) 2. Cetingoz F, 2011 (MP) 3. Romero R, 2012 (MP, Pgel) 2016 (MP) No RCT � 1. Winer N, 2015 No RCT
 Authors Regimens Population")
17 OHPC Singleton gestations and prior SPTB (unknown or normal CL) Authors Regimens Population GA (wk) Efficacy Meis PJ, 2003 17 -OHPC 250 mg IM/wk VS placebo (until GA 37 wk) 463 women and 16 -20 6/7 Reduction in PTB prior SPTB at 20 - wk < 37 wk (36. 3% vs 54. 9%, 366/7 wk RR 0. 66, CI 0. 54 -0. 81) <35 wk (20. 6% vs 30. 7%, RR 0. 67, CI 0. 48 -0. 93) <32 wk (11. 4% vs 19. 9% RR 0. 58, CI 0. 37 -0. 91)) Reduction in IVH (RR 0. 81) Reduction in supplemental oxygen (RR 0. 62) Based mostly on this clinical trial , 17 -OHPC has been recommended for all women with prior SPTB 20 -36 6/7 wk

17 - α hydroxyprogesterone caproate does not prevent preterm birth in patients with a short cervix

Vaginal progesterone Many studies show that vaginal progesterone can reduce PTB in ▫ Singleton gestations, prior SPTB, unknown or normal CL ▫ Singleton gestations, no prior SPTB, short CL ▫ Singleton gestations, prior SPTB, short CL

• Vaginal progesterone, but not 17 OHPC, has local antiinflammatory effects at the maternal-fetal interface and the cervix, and protects against endotoxin-induced PTB Furcron AE, et al. Vaginal progesterone, but not 17 OHPC, has anti-inflammatory effects at the murine maternal-fetal interface. Am J Obstet Gynecol 2015

Prevention of SPTB in singleton pregnancy Vaginal progesterone is superior to 17 -OHPC

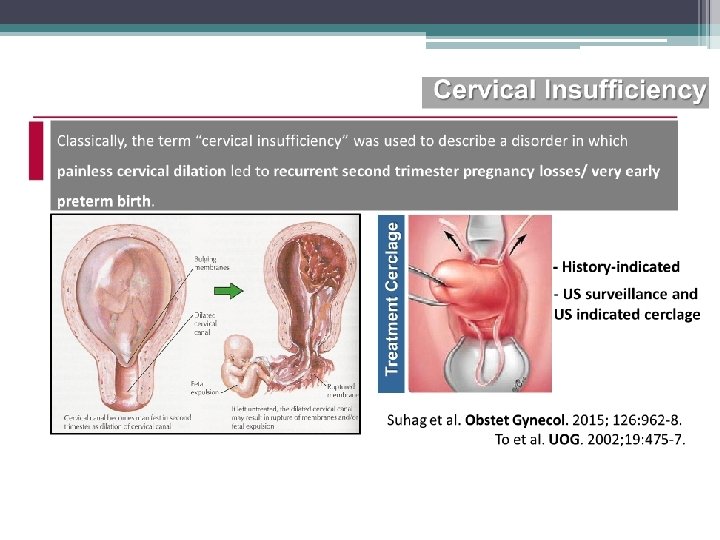
Cervical cerclage
 Efficacy Berghella V,")
Singleton gestations, short CL Cervical cerclage Authors Regimens Population GA (wk) Efficacy Berghella V, 2005 (metaanalysis; 4 RCTs) Cerclage (305) VS no cerclage(302) 607 women with CL < 25 mm < 24 wk No reduction in PTB GA < 35 wk
 Efficacy")
Singleton gestations, prior PTB, short CL Cervical cerclage Authors Regimens Population GA (wk) Efficacy Berghella V, 2011 (metaanalysis; 5 RCTs) Cerclage VS no cerclage 504 women with prior PTB and CL < 25 mm < 24 wk Reduction in PTB GA < 35 wk (RR 0. 70) Reduction in composite neonatal morbidity and mortality (RR 0. 64)

Cervical pessary • Be used for cervical insufficiency
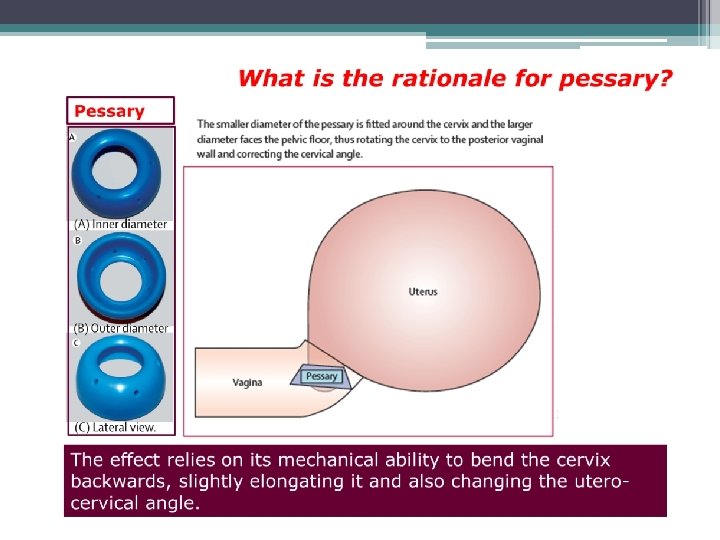

Cervical pessary Conclusions • The cervical pessary seems an affordable, safe, and reliable alternative for prevention of PTB in a singleton pregnancy with short CL (< 25 mm) at midtrimester (GA 18 -24 wk). • In view of the differences in outcomes between Hui et al. and the PECEP trial, further research is urgently needed to confirm the efficacy of cerclage pessary in prevention of preterm birth.

Progesterone for the prevention of preterm birth in preterm labor

Progesterone for the prevention of preterm birth in preterm labor Conclusions: • Progesterone may attenuate the shortening of cervical length and reduce the frequency of uterine contractions. • There is currently insufficient evidence to recommend progesterone for primary adjunctive tocolysis and maintenance tocolysis.

Progesterone for the prevention of preterm birth in PPROM Conclusions: • Insufficient evidence to assess effect of progesterone in women with PPROM

Progesterone for the prevention of preterm birth in multiple pregnancy

Progesterone for the prevention of preterm birth in multiple pregnancy Conclusions: • The evidence does not support the use of any type of progesterone for prevention of PTB in multiple gestations with unknown CL nor short CL.
 In twin pregnancies with a short cervical")
Strategy in the prevention of PTB (2016) In twin pregnancies with a short cervical length: • Vaginal progesterone may be effective in the reduction of adverse perinatal outcomes. • RCT is needed to confirm this hypothesis. • Does not reduce the rate of PTB in unselected twin cohorts. • Should not be used in the prevention of PTB in twin pregnancy. Cervical pessary could be beneficial in pregnant women with a short cervix carrying twins.

Preterm birth prevention: guildlines or recommendations

Algorithm for use of progesterone in prevention of PTB in clinical care (SMFM and ACOG, 2012) Singletons No prior SPTB Prior SPTB Single TVU CL at 18 -24 wk 17 OHPC CL ≤ 20 mm CL >20 mm Vaginal progesterone Routine obstetric care Serial TVU CL At 16 -236/7 wk CL < 25 mm CL ≥ 25 mm Cerclage; continue 17 OHPC Continue 17 OHPC SMFM. Progesterone and preterm birth prevention. Am J Obstet Gynecol 2012.

UK guidelines: 2015 Short cervix plus prior history of PTB or midtrimester loss between GA 16 -34 wk Offer a choice of either prophylactic vaginal progesterone or prophylactic cervical cerclage plus no prior history of PTB Offer prophylactic vaginal progesterone < 25 mm (GA 16 -24 wk) plus PPROM in a previous pregnancy or a history of cervical trauma Consider prophylactic cervical cerclage
 and vaginal")
FIGO recommendations regarding the use of transvaginal sonographic cervical length (TVS CL) and vaginal progesterone use for the prevention of preterm birth Population All pregnant women with a singleton gestation Recommendation TVS CL measurement at 19– 23 6/7 weeks for all pregnant patients. Vaginal progesterone administered to women with a CL ≤ 25 mm. Vaginal progesterone 200 mg vaginal soft capsules or 90 mg vaginal gel of micronized progesterone Time using progesterone Treatment should begin at the time of the diagnosis of a short cervix until 36 6/7 weeks, labor, or rupture of membranes. Risk assessment TVS CL on all patients regardless of obstetrical history. Other recommendation When a TVS is not available other devices may be used as a screening tool to measure objectively and reliably the CL.

RTCOG recommendations: 2015 Prevention of SPTB
 Progesterone, cerclage or pessary plus singleton or no history")
Strategy for PTB prevention (2016) Progesterone, cerclage or pessary plus singleton or no history of prior PTB Short cervix Micronized progesterone or Gel progesterone 200 mg/daily until 36+6 wk 90 mg/daily until 36+6 wk +Early application of pessary? shows improvement of outcome plus prior history of PTB Vaginal progesterone or cerclage or pessary The optimal treatment may depend upon adverse events, cost and patient/clinician preferences. < 25 mm plus twins in the current pregnancy RCTs are needed to demonstrate if vaginal progesterone might improve neonatal outcome Pessary shows improvement of outcome in subgroups

Cost-effectiveness and decision analyses • Combination of universal TVS CL screening and vaginal progesterone administration to women with a short cervix is a cost-effective intervention that prevents PTB and associated perinatal morbidity and mortality. • Universal TVS CL and treatment with vaginal progesterone for singleton gestations in the US would result in an annual reduction of approximately 30, 000 PTB before GA 34 weeks and of 17, 500 cases of major neonatal morbidity or neonatal mortality. Conde-Agudelo A. Vaginal progesterone to prevent preterm birth in singleton gestations with short cervix: clinical and public health implications. Am J Obstet Gynecol 2016, 214: 235 -42.

What is the role for magnesium sulfate for fetal neuroprotection?

Mechanism of magnesium sulfate for fetal neuroprotection Not well understood, but potential neuroprotective actions include ▫ ▫ ▫ ▫ Antioxidant effects Reduction in proinflammatory cytokines Blockage of glutamate activated calcium channels Stabilization of membranes Increased cerebral blood flow Prevention of large blood pressure fluctuations Prevention of cerebral convulsions

Magnesium sulfate for women at risk of preterm birth for neuroprotection of the fetus • 5 RCTs; N = 6145 babies • Results: Antenatal magnesium sulfate therapy given to women at risk of preterm birth ▫ Reduction in the rate of CP (RR=0. 68; 95%CI=0. 540. 87 ▫ Reduction in the rate of substantial gross motor dysfunction (RR=0. 61; 95%CI=0. 44 -0. 85) The number of women needed to be treated to benefit one baby by avoiding cerebral palsy is 63 Doyle LW, Crowther CA, Middleton P, Marret S, Rouse D. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. Cochrane Database of Systematic Reviews 2009, Issue 1.

Different magnesium sulfate regimens for neuroprotection of the fetus for women at risk of preterm birth • No RCTs • Conclusions: Not enough research has been carried out to show what is the best dose of, and how best to provide, magnesium sulfate to mothers prior to very preterm birth to protect the baby’s brain Bain E, Middleton P, Crowther CA. Different magnesium sulphate regimens for neuroprotection of the fetus for women at risk of preterm birth. Cochrane Database of Systematic Reviews 2012, Issue 2.

Up. To. Date 2016: Antenatal administration of magnesium sulfate for fetal neuroprotection Recommendations • GA 24 – 32 wk • Imminent preterm delivery (PPROM and intact preterm labor) within 24 hr • Magnesium sulfate: 4 gm IV loading dose followed by a 1 gm/hr infusion. This therapy is discontinued by 24 hr after initiation if delivery has not occurred. • Indomethacin for tocolysis • Avoiding retreatment for women who do not deliver after an initial course

Diagnosis • Definitions of preterm labor vary, but the research criteria commonly hold it to be contractions occurring at a rate of 4 in 20 min or 8 in 1 hr with at least one of the followings: cervical change over time or dilatation greater than 1. 0 (2. 0) cm or cervical effacement of at least 80 %

RTCOG: Recommendations of preterm labor and preterm premature rupture of membranes management: 2015

Premature labor • Identify and manage causes /risk factors of premature labor • Monitor maternal and fetal well-being GA > 34 wk GA > 24 -33+6 wk Contraindications to inhibit labor No Yes • NPO • IV fluid • Single course corticosteroids for fetal lung maturity • Inhibit uterine contractions (Tocolytic drugs) • Mg. SO 4 for fetal neuroprotection (GA<32 wk) • Monitor uterine contractions • Monitor fetal well-being • Antibiotic for GBS prophylaxis if failed inhibition • NPO • IV fluid • Antibiotic for GBS prophylaxis • Monitor uterine contractions • Monitor fetal well-being • Gentle vaginal delivery

Contraindications to inhibit labor • • • Severe preclampsia, eclampsia Placental abruption Nonreassuring fetal status Chorioamnionitis Severe fetal anomalies (incompatible with life) Fetal death in utero

PPROM Diagnosis: Sterile speculum exam: fluid from cervix and /or vagina and/or nitrazine test or fern test • USG: GA, EFW, AFI, presentation, fetal growth and anomalies • Vaginal and rectal swab: culture/sensitivity; Urine : culture/sensitivity • CBC • Fetal surveillance Evaluation for chorioamnionitis, placental abruption, fetal death, nonreassuring test, advanced labor No GA > 24 -33+6 wk GA > 34 wk Yes Delivery • Antibiotic for GBS prophylaxis • Broad spectrum antibiotics if chorioamnionitis found Expectant management • Serial evaluation for chorioamnionitis, labor, placental abruption, fetal well-being, fetal growth • Single course corticosteroids for fetal lung maturity • Antibiotics for prolonged latency period • Delivery if chorioamnionitis, placental abruption, nonreassuring test, advanced labor, GA > 34 wk • Mg. SO 4 for fetal neuroprotection (if GA < 32 wk) • Antibiotic for GBS prophylaxis • Broad spectrum antibiotics if chorioamnionitis found Delivery

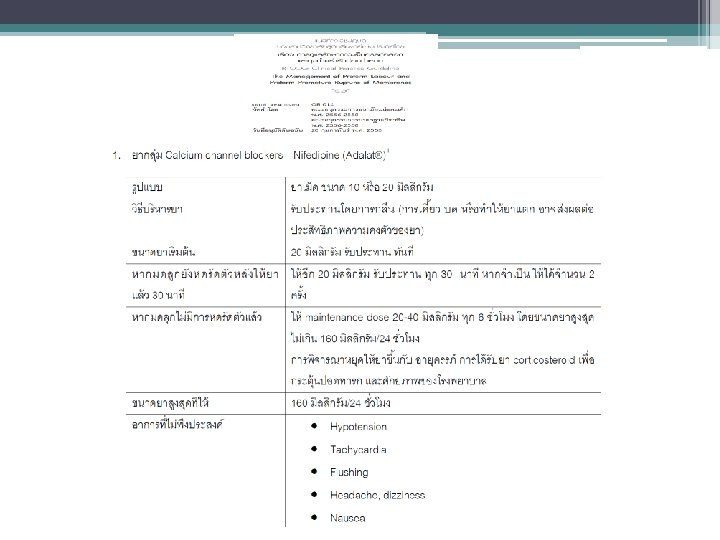
Tocolytic drugs • Calcium channel blocker: nifedipine • Beta–agonists: terbutarine, salbutamol • COX inhibitor: indomethacin • Oxytocin receptor antagonist: atosiban • Magnesium sulfate

Acute tocolysis for preterm labor • Nifedipine VS Betamimetics ▫ A significant reduction in �delivery within 7 d of initiation of treatment and before 34 wks’ gestation �respiratory distress syndrome �necrotizing enterocolitis �intraventricular hemorrhage �neonatal jaundice �admission to the neonatal intensive care unit ▫ A significantly fewer maternal adverse events ▫ Maintenance nifedipine tocolysis ineffective in prolonging gestation or improving neonatal outcomes Conde-Agudelo A, et al. Nifedipine in the management of preterm labor: a systematic review and metaanalysis. Am J Obstet Gynecol 2011; 204: 134. e 1 -20.

Nifedipine as a tocolytic agent today • The optimal initial dose appears to be 10 mg orally or sublingually. • If contractions persist, this dose could be repeated every 15 -20 min up to a maximal total dose of 40 mg during the first hr of treatment and then 20 mg orally every 6 -8 hr for 2 -3 d. • Side effects: hypotension, tachycardia, palpitations, flushing, headaches, dizziness, nausea

The U. S. FDA is warning that terbutaline administered by injection or through an infusion pump should not be used in pregnant women for prevention or prolonged )beyond 48 -72 hours (treatment of preterm labor due to the potential for serious maternal heart problems and death. In addition, oral terbutaline tablets should not be used for prevention or treatment of preterm labor.

Should women with preterm contractions but without cervical change be treated?

Preterm contraction without cervical change • Regular preterm contractions are common; however, these contractions do not reliably predict which women will have subsequent progressive cervical change. • In a study of 763 women who had unscheduled triage visits for symptoms of preterm labor, only 18% gave birth before GA 37 wk and only 3% gave birth within 2 wk of presenting with symptoms. • No evidence exists to support the use of prophylactic tocolytic therapy, home uterine activity monitoring, cerclage, or narcotics to prevent preterm delivery in women with contractions but no cervical change. • Conclusions: Women with preterm contractions without cervical change, especially those with a cervical dilation of less than 2 cm, generally should not be treated with tocolytics.

Should tocolytics be used after acute therapy?

Maintenance therapy with tocolytics is ineffective for preventing preterm birth and improving neonatal outcomes and is not recommended for this purpose.
-34 wk •")
Antenatal steroid therapy for fetal maturation • Preterm labor: GA 24 (23)-34 wk • PROM: GA 24 (23)-34 wk • Reduction of RDS, PNM, and morbidities • A single course recommended

Antenatal steroid therapy for fetal maturation • A single repeat course of antenatal corticosteroids should be considered in women who are less than 340/7 weeks of gestation who have an imminent risk of preterm delivery within the next 7 days, and whose prior course of antenatal corticosteroids was administered more than 14 days previously. • Rescue course corticosteroids could be provided as early as 7 days from the prior dose, if indicated by the clinical scenario.
 given intramuscularly 24 hr")
Antenatal steroid therapy for fetal maturation • Betamethasone (12 mg) given intramuscularly 24 hr apart for 2 doses • Dexamethasone (6 mg) given intramuscularly every 12 hr for 4 doses

Is there a role for antibiotics in preterm labor?

Antibiotics should not be used to prolong gestation or improve neonatal outcomes in women with preterm labor and intact membranes. This recommendation is distinct from recommendations for antibiotic use for preterm PROM and group B streptococci carrier status

Antibiotics for prolonged latency for PPROM • RCOG: Erythromycin 250 mg po q 6 hr for 10 days • NICHD-MFMU, ACOG: Ampicillin 2 gm and erythromycin 250 mg IV q 6 hr for 48 hr then amoxicillin 250 mg and erythromycin (250 -333 mg) po q 8 hr for 5 days • RTCOG: Ampicillin 2 gm IV q 6 hr for 48 hr and erythromycin 250 mg po q 6 hr for 48 hr then ampicillin 250 mg and erythromycin base 333 mg po q 8 hr for 5 days

Antibiotics for GBS prophylaxis • Pen G sodium 5 million units IV stat then 2. 5 -3 million units IV q 4 hr • Ampicillin 2 gm IV stat then 1 gm IV q 4 hr • Cefazolin 2 gm IV stat then 1 gm IV q 8 hr • Clindamycin 900 mg IV q 8 hr • Vancomycin 1 gm IV q 12 hr

Is there a role for nonpharmacologic management of women with preterm contractions or preterm labor?

• Bed rest , sedation, and hydration have been recommended to women with symptoms of preterm labor to prevent preterm delivery, these measures have not been shown to be effective for the prevention of preterm birth and should not be routinely recommended. • The potential harm, including venous thromboembolism, bone demineralization, and deconditioning, and the negative effects, such as loss of employment, should not be underestimated.

Preterm labor and multiple gestations • Tocolytics to inhibit labor: greater risk of maternal complications • Prophylactic tocolytics: not reduce the risk of preterm birth or improve neonatal outcomes • Antenatal corticosteroids (magnesium sulfate for fetal neuroprotection): recommended
 • If")
Timing of cord clamping for preterm babies (born vaginally or by C/S) • If a preterm baby needs to be moved away from the mother for resuscitation, or there is significant maternal bleeding: ▫ consider milking the cord and ▫ clamp the cord as soon as possible. • Wait at least 30 sec, but no longer than 3 min, before clamping the cord of preterm babies if the mother and baby are stable. • Position the baby at or below the level of the placenta before clamping the cord.

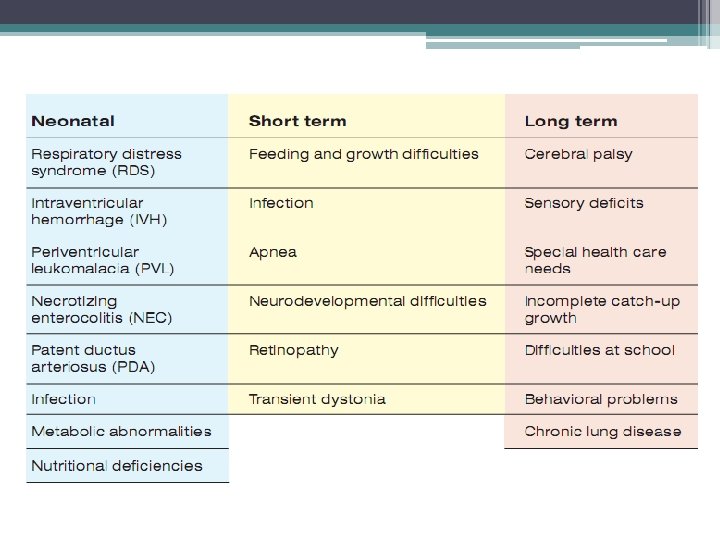
Take home message • PTB: leading cause of neonatal morbidity and mortality • 2/3 of PTB: spontaneous PTL and preterm PROM • 3 major risk factors of SPTB: previous SPTB, short CL and multiple gestations • Prevention of SPTB: progesterone supplementation, prevention of non-medically indicated late PTB and early PTB, cervical cerclage/pessary, smoking cessation, judicious use of ART • Vaginal progesterone is superior to 17 OHPC for prevention of SPTB in women with singleton pregnancy and short CL with or without prior PTB • Progesterone can not prevent SPTB in PPROM and multiple pregnancy • Cervical pessary may be beneficial in pregnant women with a short cervix carrying twins

Take home message • Nifedipine is a tocolytic agent today • Insufficient evidence to recommend progesterone for primary adjunctive tocolysis and maintenance tocolysis. • Dexamethasone for fetal lung maturation: GA 23 -34 wk; 1 rescue course if administration > 1 weeks and GA < 34 wk • Antibiotics for prolonged latency for PPROM: ampicillin 2 gm and erythromycin 250 mg IV q 6 hr for 48 hr then amoxicillin 250 mg and erythromycin (250 -333 mg) po q 8 hr for 5 days • Antibiotics for GBS prophylaxis: ampicillin 2 gm IV stat then 1 gm IV q 4 hr • Good cooperation with NICU
- Slides: 95