Pharmacology of Enteral Agents Oral Sedation Advantages Acceptance




 Extracellular Membrane Intracellular CYP 3 A 4")



… ROUTE – – – – IV IM SUBCUTANEOUS ORAL RECTAL INHALATION TRANSDERMAL")











")









 Metabolism/excretion; Liver/urine Advantages – Sedation")
 Usual dosage; 1 o prior to appt – Adults; 2 -10 mg")
 Usual dosage 1 hour prior to appt – Adult 2 -4 mg")
 Usual dosage one hour prior to appt – Adult; 10 -30 mg")
 Usual dosage one hour prior to appt – Adult; 0. 25 mg")
 Usual dosage one hour prior to appt – Adult; 0. 25 -1")
 Usual dosage 15 -30 min prior to appt – Not recommended for")
 Usual dosage 1 hour prior to appt – Adult; 10 mg –")

 Usual dosage 1 hour prior to appt – Adult; 50 -100")
 Usual dosage 1 hour prior to appt – Adult; 50 -100 mg")

 Usual dosage 1 hour prior to appt – Adult; 25 -50 mg")




 Chlordiazepoxide (LIBRIUM) Cdlonazepam (KLONOPIN) Cloraxepate (TRANXENE) Diazepam (VALIUM) Estazloam")



")





 Indicated for the treatment of insomnia Plasma half-life: 1. 5 -5. 5")

- Slides: 63
Pharmacology of Enteral Agents
Oral Sedation… Advantages – – – – Acceptance Administration Low cost Decreased incidence of adverse reactions Decreased severity of adverse reactions No needles Various dosage forms Decreased severity of allergic reactions Disadvantages – – – – – Patient compliance Delayed onset Erratic absorption Inability to titrate Inability to readily alter level of sedation Prolonged duration Not for severe anxiety levels Adverse drug-drug interactions Special training and permit
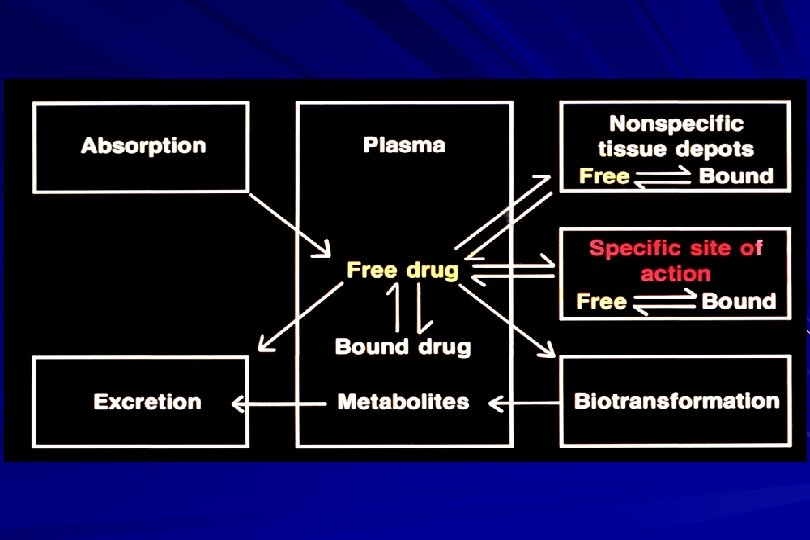
Terminology… Absorption—the process by which a drug enters the circulation – Factors affecting absorption Drug form (tablet, capsule, elixir) Gastric emptying Acidity Presence of food and types of food GI motility Most drugs are absorbed in the small intestine
Alterations in Drug Absorption P-glycoprotein carrier system – Found in the plasma membranes in the intestine, proximal tubules of the kidney, brain, liver, testes – Acts as a pump for drugs and toxins being transported away from tissues, out of the tissues Part of the “first pass effect” – “Gate-keeper” for cytochrome P 450 system
P-glycoprotein (P-gp) Extracellular Membrane Intracellular CYP 3 A 4
Terminology… First Pass Effect--initial extensive metabolism in the liver as the drug travels from the small intestine via the hepatic portal system through the liver – Results in reduction of plasma concentration – Important for benzodiazepines with low bioavailability Triazloam Midazolam
FIRST PASS METABOLISM
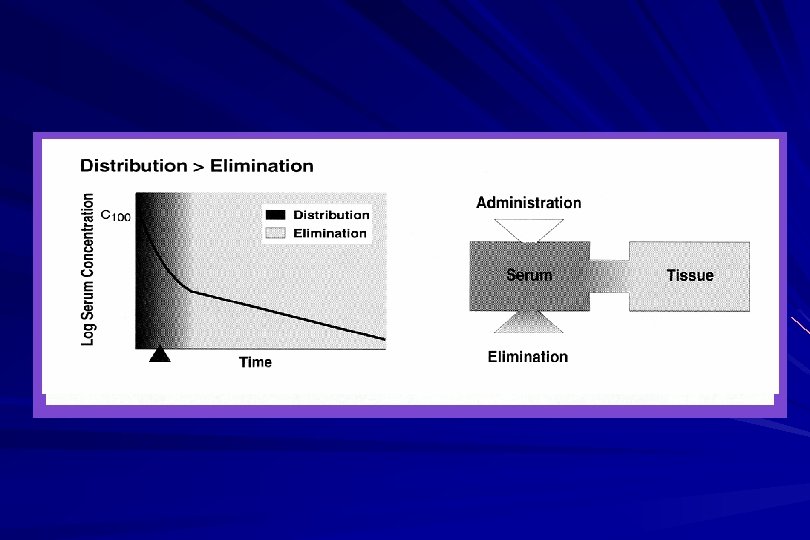
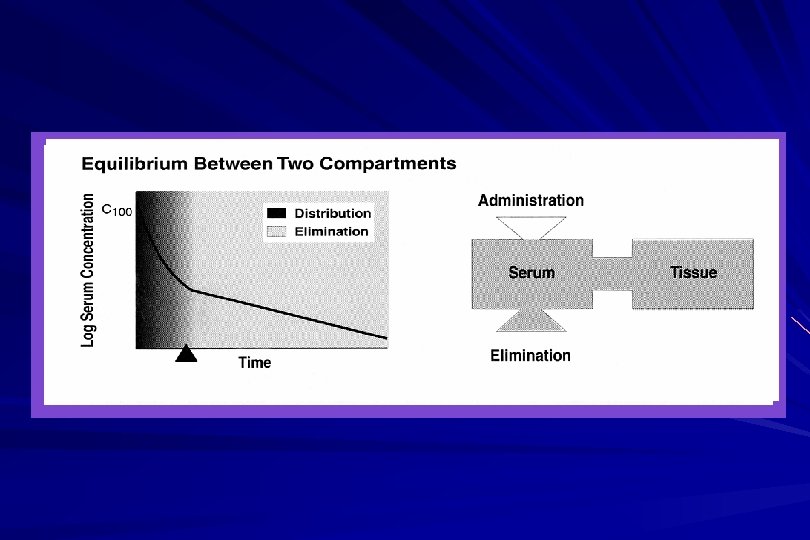
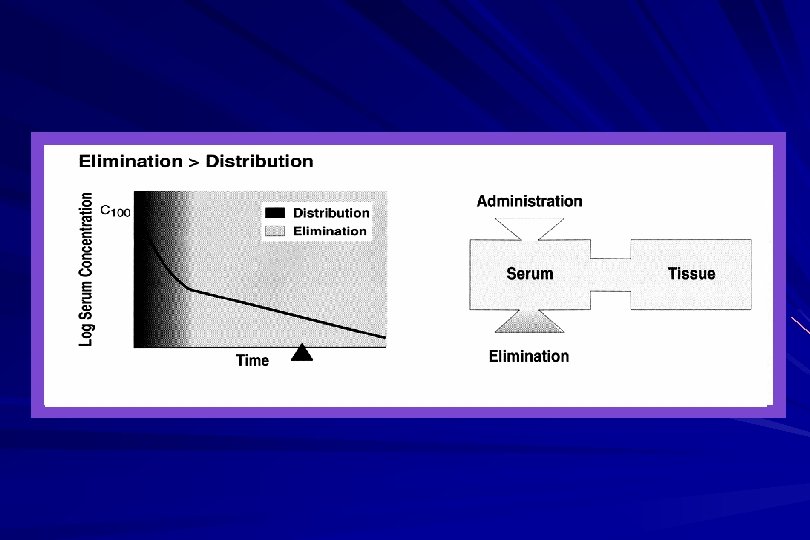
Terminology… Distribution—process by which the drug in the plasma enters target tissues, depot tissues, metabolic and excretory sites Factors affecting distribution – – Lean-body mass vs. fat content Concentration of plasma proteins Malnutrition Age Pregnancy – Competition for protein binding sites from other drugs
Bioavailability (%)… ROUTE – – – – IV IM SUBCUTANEOUS ORAL RECTAL INHALATION TRANSDERMAL BIOAVAILABILITY 100 75 to </=100 5 to <100 30 to <100 5 to < 100 80 to </=100
Terminology… Biotransformation—metabolic pathways in the body, primarily the liver, convert absorbed drugs into different chemical configurations, usually with the end result of making the drug less active and more readily excretable (polar and water soluble) – Phase I—utilizing Cytochrome P 450 – Phase II—conjugation
Phases of Metabolism Phase I – Oxidation, hydrolysis, or reduction increasing the drugs water solubility Phase II – Attachment of an additional molecule creating an inactive and more water soluble compound Glutathione, conjugation, glucuronidation, sulfation, acetylation, methylation
Metabolism R Phase I R Hepatocyte Billiary capillary OH R Phase II O - Glucuronide
Cytochrome P 450… Genetically determined super family of enzymes found in the liver and gut to detoxify endogenous and exogenous substances – – Blood flow the liver Activity and concentration of enzymes Liver disease Basis for the pharmacokinetic drug interactions most frequently encountered in dentistry. (CYP 3 A 4 isoenzyme inhibition)
Terminology… Excretion– process by which a drug in the circulation is removed from the body (urine, bile, feces) – Renal function and disease – Water solubility and chemistry of a drug or metabolite
*Peripheral compartment
Enhanced Bioavailability of Triazolam following Sublingual Versus Oral Administration. Scavone JM et al, J. Clinical Pharm 1986; 26: 208 -210 AUC greater for sublingual than orally – 28. 9 vs 22. 6 ng-hr/ml Sublingual peak plasma concentration greater – 4. 7 vs 3. 9 ng/ml No difference in elimination half-life and the time of peak concentration
Enhanced Bioavailability of Triazolam following Sublingual Versus Oral Administration. – First-pass extraction bypassed Clinical effects may likewise be enhanced by sublingual administration. 4 3 PLASMA TRIAZOLAM CONCENTRATION (ng/ml) The bioavailability of sublingual triazolam increased by an average of 28% vs oral administration Scavone JM et al, J. Clinical Pharm 1986; 26: 208 -210 0. 5 mg oral 2 0. 5 mg sublingual 1 . 7 . 4 . 2 0 2 4 6 8 10 12 14 16 18 HOURS AFTER DOSE
Triazolam Pharmacokinetics After Intravenous, Oral and Sublingual Administration 16 14 12 Triazolam Route Of Administration 6 TRIAZOLAM (ng/ml) Fraction absorbed relative to IV was 20% greater SL vs Oral Bioavailability 44% (oral) 53% (sublingual) SL avoid first-pass metabolism producing earlier and higher peak concentrations Kroboth, PD et al J Clin Psychopharm 15: Aug 95 259 -262 4 2 0 0 2 4 6 TIME (hr) 8 10 12
Terminology… Half-life—time required to reduce the amount of drug in the circulation by one-half – – – Age Disease Blood flow to liver Idiosyncrasy—unusual/unpredictable response to a drug – Hyperalgesia – dysphoria
Terminology… Toxicity—Adverse effect that is a direct extension of a drug’s therapeutic actions (loss of consciousness) Therapeutic Index—ratio of the toxic dose of a drug to its therapeutic dose: the higher the ratio, the greater the relative safety of the drug
Patient Considerations… Factors determining variability in patient response: – Age (very young and old) – Genetics (CYP) – Disease states – ETOH consumption – Normal biological variations – Pharmacokinetic factors
Special Considerations… Pediatric patients – Weight and dosage calculations – Enhanced vagal responses – Ability to swallow solid dose forms – Taste variations – Increased likelihood of aspiration
Special Considerations… Geriatric patients – Phiz changes: decreased functional reserve cerebral, renal and hepatic blood flow – Chronic diseases – Multiple medications – Decreased intestinal absorption – Decreased receptor populations – Decreased lean body mass – Decreased plasma protein binding – Decreased initial doses of sedatives
Medically Compromised Patients Drug interactions Altered response to drugs Need for adjunctive medications Stress-reduction protocol
Factors in Drug Selection and Dosage… Age Weight Medical status Level of anxiety
Pharmacologic Principles for Oral Sedative Drugs… All produce CNS depression – Drowsiness, dizziness – Drug interactions—CNS depressants Warnings – Drowsiness—don’t drive, legal decision, etc – May be habit forming – Accompanied by a responsible adult Food interactions – Presence of food delays gastric emptying and delays onset/reduces effectiveness of agents
Principles Continued Re-administration of Oral Agents – NOT recommended secondary to accumulation When more than one agent is used the dosage of both agents must be reduced Variable effects of oral sedation Dosage of sedatives should be reduced in children, elderly, and the medically compromised patients
FDA Pregnancy Categories… A—studies fail to demonstrate a risk to the fetus in the first trimester, no evidence of risk in later trimesters. The possibility of fetal harm appears remote B—either animal studies have not shown a risk, but there are no controlled studies in pregnant women, or animal studies have shown a fetal risk that was not confirmed in controlled studies in women
FDA Pregnancy Categories… C—animal studies have shown a risk but no controlled studies in women, or there are no studies in women or animals. Drugs should be given only if the potential benefits justify the potential risks to the fetus D—there is positive evidence of fetal risk. If the drug is needed in a life-threatening situation or for a serious disease for which safer drugs cannot be used or are ineffective X—the drug is contraindicated in women who are or may become pregnant
Standard Dose The standard dose of a drug is based on trials in healthy volunteers and patients with average ability to absorb, distribute, metabolize and eliminate the drug The standard dose will not be suitable for every patient
Benzodiazepines… Mechanism of action – GABA receptor agonist (facilitator) Metabolism/excretion; Liver/urine Advantages – Sedation – Wide therapeutic index – Antianxiety effects – Useful for producing sleep the night before – Reversal agent (flumazenil)
Diazepam (Valium) Usual dosage; 1 o prior to appt – Adults; 2 -10 mg – Children; 0. 15 -0. 3 mg/kg Onset; 1 hr, peak concentration in 2 hrs Duration; 1 -3 hours Contraindications – Allergy, narrow angle glaucoma Precautions – Drug interactions at CYP 3 A 4 and CYP 2 C 19 Availability – 2, 5, and 10 mg tablets; syrup 10 mg/5 cc Active metabolites—yes Pregnancy category D
Lorazepam (Ativan) Usual dosage 1 hour prior to appt – Adult 2 -4 mg – Child; 0. 05 mg/kg not to exceed adult dose Onset; 1 hour Duration; 2 -4 hours Containdications – Allergy, narrow angle glaucoma Precautions – – Excessive sedation Not to be used in patients with primary depressive disorder or psychosis Active metabolites—No Pregnancy category--D
Oxazepam (SERAX) Usual dosage one hour prior to appt – Adult; 10 -30 mg – No child dose Onset; 1 hour Duration; 2 -4 hours, peak at 3 hours Contraindications—allergy Precautions—same as other sedative agents Availability – 10, 15, 30 mg capsules and 15 mg tablets Active metabolites—No Pregnancy category—D
Triazolam (HALCION) Usual dosage one hour prior to appt – Adult; 0. 25 mg – Not recommended for children Onset; 1 hour, peak plasma level 2 hours Duration; 1 -3 hours Contraindications—pregnancy Precautions—can produce anterograde amnesia. Excessive sedation in elderly Availability – O. 125 and 0. 25 mg tablets Active metabolites—No Pregnancy category—X
Alprazolam (XANAX) Usual dosage one hour prior to appt – Adult; 0. 25 -1 mg – Not recommended for children Onset; 1 hour, peak in 1 -2 hours Duration; 1 -3 hours Contraindications—allergy and narrow angle glaucoma Precautions – Drug interactions at CYP 3 A 4 Availability – 0. 25, 0. 5 and 1 mg tablets Active metabolites—No Pregnancy category--D
Midazolam (VERSED) Usual dosage 15 -30 min prior to appt – Not recommended for adult – Child; 0. 25 -0. 5 mg/kg not to exceed 20 mg Onset; 15 -30 minutes Duration; 30 min to 1 hour Contraindications – – Allergy Narrow angle glaucoma Precautions – Drug interactions at CYP 3 A 4 Availability; syrup 2 mg/cc Active metabolites—No Pregnancy category—D
Zolpidem (AMBIEN) Usual dosage 1 hour prior to appt – Adult; 10 mg – Not recommended for children Onset; 1 hour peak effect in 1. 6 hours Duration; 2 -3 hours Contraindications; allergy Precautions; same as other oral sedatives Availability; 5 and 10 mg tablets Active metabolites—No Pregnancy category—B
Antihistamines… Sedation is a common action of some H-1 receptor antagonists Additional beneficial effects; anticholinergic actions and some reduction in salivation – Hyproxyzine – Diphenhydramine
Hydroxyzine (ATARAX, VISTARIL) Usual dosage 1 hour prior to appt – Adult; 50 -100 mg – Child; 1. 1 -2. 2 mg/kg Onset; 30 min, peak effect 2 hours Duration; 3 -4 hours Contraindications; allergy Precautions; same as other oral sedatives Availability – Atarax; 10, 25, 50, 100 mg tabs; syrup 10 mg/5 cc – Vistaril; 25, 50, 100 mg capsules; oral susp 25 mg/5 cc Active metabolites—No Pregnancy category—D
Diphenhydramine (BENADRYL) Usual dosage 1 hour prior to appt – Adult; 50 -100 mg – Child; 1. 5 mg/kg not to exceed adult dose Onset; 1 hour Duration; 4 -6 hours Contraindications; allergy Precautions; anticholinergic actions; – Worsen asthma, glaucoma GI/urinary obstruction Availability; 25, 50 mg tabs; elixir 12. 5/5 cc Active metabolites—No Pregnancy category—B
Phenothiazines… Traditionally used in the treatment of some major psychiatric diseases Some members of this group possess significant sedative activity Otherapeutic actions – Anticholinergic – Antidopaminergic – Anti-adrenergic – antiemetic
Promethazine (PHENERGAN) Usual dosage 1 hour prior to appt – Adult; 25 -50 mg – Child; 2. 2 mg/kg as a sole agent 1. 1 mg/kg in combination with other drugs Onset; 1 hour peak effect 2 hours Duration; 3 -4 hours (may persist 12 hrs) Precautions – Use with caution in pts with Sz disorders – Tardive dyskinesias Availability; 12. 5, 25, 50 mg tabs; – Syrup 6. 25 and 25 mg/5 cc – Suppositories 12. 5, 25, 50 mg Active metabolites—No Pregnancy category—C New FDA warning: (2006) this drug is no longer indicated in children under 2 years of age…and should be used with great caution in any child (all preps of the drug)
Drug Interaction Involving Sedative Agents Pharmacokinetic interactions – One drug inhibits or stimulates the absorption, distribution, metabolism or excretion of another drug Increased activity of some Benzos by erythromycin which inhibits CYP 3 A 4 isoenzyme Pharmacodynamic interactions – Interaction of 2 drugs as a result of a common physiologic effect Increased CNS depression with co-administration of opioid and Benzodiazepine
Drug Interaction Involving Sedative Agents Summation; interaction between 2 drugs in which the effect of both drugs is approximated by the simple additive effect of each drug given separately – 1+1=2 Potentiation; interaction in which total effect of both drugs given together is greater than predicted by the sum of each drug given separately – 1+1>2
Drug Interaction Involving Sedative Agents Antagonism; the reduction in the effect of one drug by another – Competitive – Non-competitive – Physiologic
Clinically Significant Drug Interactions of Sedatives Inhibitors of benzodiazepine oxidation – – – Azole antifungal drugs (NIZORAL) 2 Cimetidine (TAGAMET) 3 Disulfiram (ANTABUSE) 3 Diltiazem (CARDIZEM) 2 Fluvoxamine (LUVOX) 3 Indinavir (CRIXIVAN) 2 Macrolide antibiotics (ERYC) 2 Nefazodone (SERXONE) 3 Omeprazole (PRILOSEC) 3 Oral contraceptives 3 Protease inhibitors (NORVIR) 2
Oxidatively Metabolized Benzodiazepines Alprazolam (XANAX) Chlordiazepoxide (LIBRIUM) Cdlonazepam (KLONOPIN) Cloraxepate (TRANXENE) Diazepam (VALIUM) Estazloam (PROSOM) Flurazepam (DALMANE) Halazepam (PAXIPAM) Quazepam (DORAL) Trazolam (HALCION)
Drugs Which Reduce Effect of Benzodiazepines Primarily triazolam and midazolam – Stimulate metabolism Rifamycins (RIFAMPIN) 2 -3 Carbamazepine (TEGRETOL) 3 Theophylline (THEO-DUR) 2
Extensive Impairment of Triazolam and Alprazolam Clearance by Short-Term Low-Dose Ritonavir: The Clinical Dilemma of Concurrent Inhibition and Induction J Clinical Psychopharm 19: Aug 99, 293 -296 Early exposure of low-dose ritonavir will produce important impairment of alprazolam as well as triazolam clearance, similar to ketoconazole The hazard of an interaction will persist until the dosage and/or duration of exposure to ritonavir produces sufficient CYP 3 A induction to offset the inhibitory effects of ritonavir
Extensive Impairment of Triazolam and Alprazolam Clearance by Short-Term Low-Dose Ritonavir: The. Clinical Dilemma of Concurrent Inhibition and Induction J Clinical Psychopharm 19: Aug 99, 293 -296 3 30 2 WITH RITONAVIR t 1/2 = 22. 7 hr CL = 32 ml/min PLASMA ALPRAZOLAM (ng/ml) PLASMA TRIAZOLAM (ng/ml) 20 WITH RITONAVIR t 1/2 = 50 hr CL = 15 ml/min 1 0. 7 CONTROL t 1/2 = 3. 7 hr CL = 317 ml/min 0. 4 0. 2 10 7 4 CONTROL t 1/2 = 3. 7 hr CL = 317 ml/min 2 1 4 8 12 16 20 HOURS AFTER DOSE 24 4 8 12 16 20 24 28 32 HOURS AFTER DOSE
Drug Interactions Involving Phenothiazines… Beta-blockers 2 – Increased effect of both drugs Cisapride (PROPULSID) 1 – Increased cardiac toxicity of cisapride Dofetilide (TIKOSYN) 1 – Increased cardiac toxicity of dofetilide Ethanol 2 – Increases CNS depression Quinolones 1 – Increased cardiac toxicity of quinolones Paroxetine (PAXIL) 2 – Increased phenothiazine effects via CYP 2 D 6 inhibition
Oral Erythromycin and the Risk of Sudden Death from Cardiac Causes Ray et al. NEJM September 9, 2004 1089 -1096 1, 249, 943 person-years of follow-up – 1476 confirmed sudden death from cardiac causes. – CYP 3 A inhibitors studied: nitroimidazole antifungal agents, diltiazem, verapamil, and troleandomycin Each doubles the AUC for a CYP 3 A substrate Evaluated the association of oral erythromycin and the risk of sudden death of cardiac cause – – – By itself In conjunction with CYP 3 A inhibitors The control was amoxicillin
Oral Erythromycin and the Risk of Sudden Death from Cardiac Causes Ray et al. NEJM September 9, 2004 1089 -1096 The risk of sudden death from cardiac causes among patients currently using erythromycin was twice as high as that among those who had not used the antibiotic. No significant increase in risk in former users of erythromycin or those currently using amoxicillin The use of erythromycin and concurrent use of CYP 3 A inhibitors: 5 times as high to suffer sudden death of cardiac origin No increased risk in patients using amoxicillin and CYP 3 A inhibitors
Why Do Some Cases Not Go Well? Not “sleepy” enough Too “sleepy” Behavior difficulties
Why Do Some Cases Not Go Well? There is not a single enteral agent intended to be used for an office based sedation – Off label use of drugs with a primary indication: short term treatment for insomnia triazolam (Halcion) Off label indications: None Found – Management of anxiety disorders, premedication, skeletal muscle disorders, alcohol withdrawals Diazepam (Valium) Off label indications: None clinically relevant
Why Do Some Cases Not Go Well? Since there are no drugs specifically intended for enteral sedation in a dental office one should expect variability Quality of sedation is based on the drugs pharmacokinetic and pharmacodynamics properties – Pharmacodynamic tolerance
Triazolam (Halcion) Indicated for the treatment of insomnia Plasma half-life: 1. 5 -5. 5 hours Peak plasma level in approximately 2 hours – Peak levels of 1 -6 ng/ml – Peak levels dependent upon initial dose and pharmacokinetics.
Why Such Variability? Pharmacokinetics – Absorption – Distribution – Metabolism – Excretion