Pericardial diseases Pericardial anatomy PERICARDIAL EFFUSION ETIOLOGY Viral


 • • Viral (most common) Uremic (chronic renal failure) Metastatic (breast")

 • • • Chest pain with respiration, fever Shortness of")
 - not echogenic • Bloody (consider metastatic,")
 • may overestimate amount and not useful if loculated")
 • Superior to M Mode for extent and localization")





























 Neoplasms Uremia Connective tissue disorders (SLE, Scleroderma)")























 – Increased E to A – Shortened Deceleration")

")













- Slides: 93
Pericardial diseases
Pericardial anatomy
PERICARDIAL EFFUSION (ETIOLOGY) • • Viral (most common) Uremic (chronic renal failure) Metastatic (breast or lung CA) Post MI (Dresslers syndrome) Post cardiac surgery (regional) CHF, systemic diseases (lupus, AIDS) Trauma Infectious
HIV
PERICARDIAL DISEASES (CLINICAL PRESENTATION) • • • Chest pain with respiration, fever Shortness of breath Enlarged cardiac silhouette on chest X ray EKG changes with diffuse ST elevation Pulsus paradoxus, tachycardia, hypotension, neck vein distention, decreased heart sounds
PERICARDIAL FLUID • Serosanguinous (clear, pale yellow) - not echogenic • Bloody (consider metastatic, trauma) - may be echogenic • Infectious (brown, milky colored)
PERICARDIAL EFFUSION (M Mode Echocardiography) • may overestimate amount and not useful if loculated or localized • useful for timing of RV wall motion relative to mitral valve opening • Caution when only anterior echo free space present
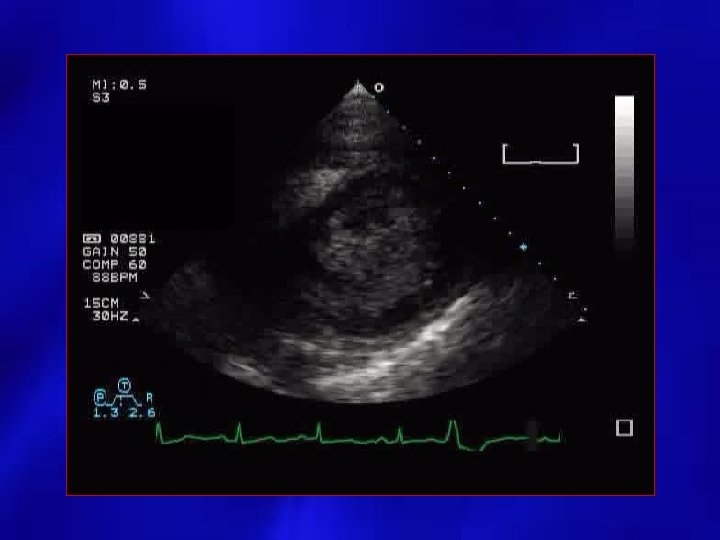
PERICARDIAL EFFUSION (2 D Echocardiography) • Superior to M Mode for extent and localization by use of multiple views • Assess for diastolic collapse of right heart chambers, IVC size and change with inspiration/expiration • Identify intrapericardial process (clot, tumor, fibrin strands) • Differentiate pericardial from pleural effusion by recognition of descending aorta • Non diagnostic for pericardial thickness
Parasternal long axis LV Effus DAO AO LA
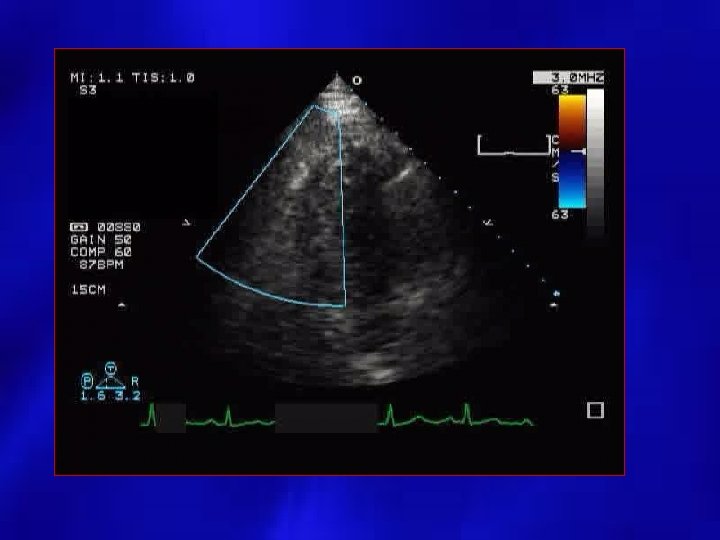
Parasternal Short Axis
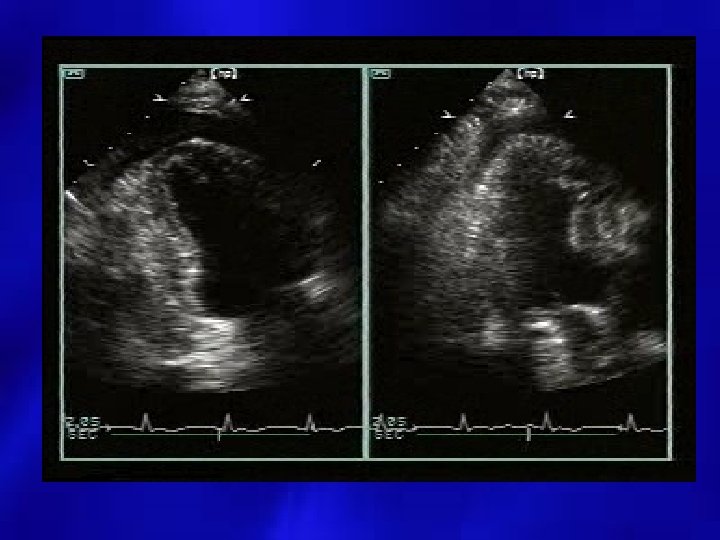
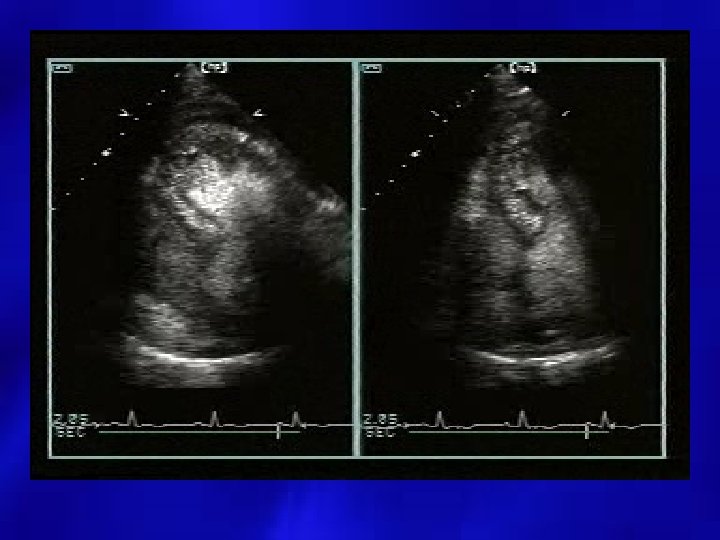
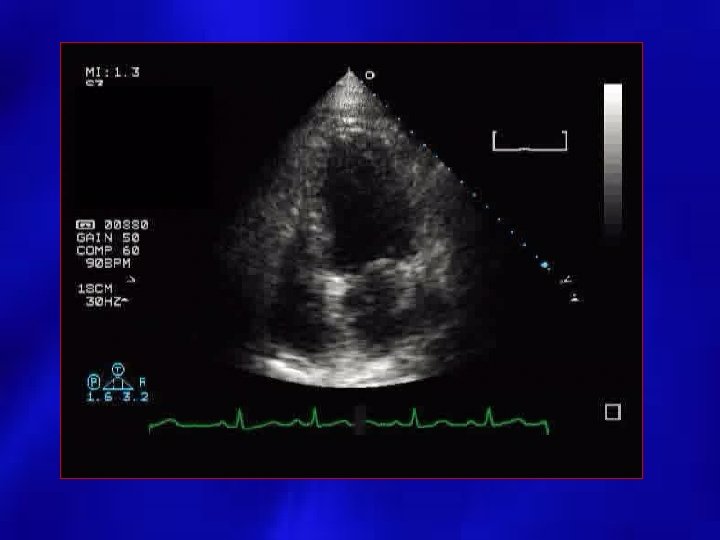
Apical 4 C
Subcostal view
Fibrous Strands
Unequal distribution
M Mode echo
M-Mode RV collapse/ Delayed RV Relaxation
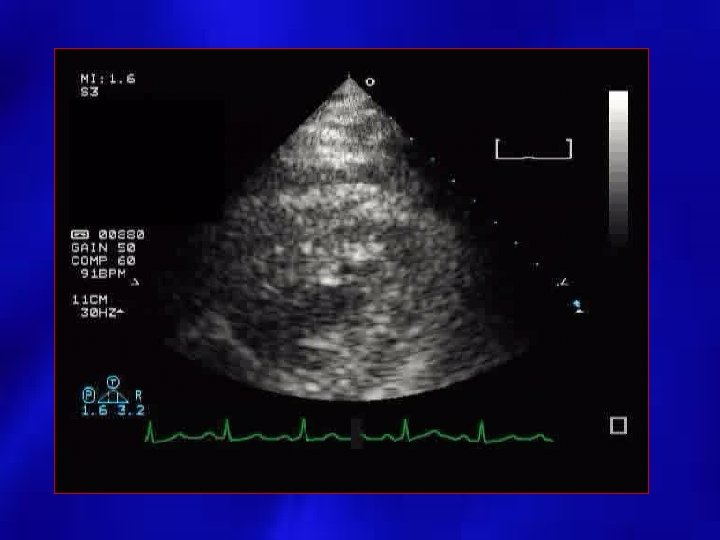
PERICARDIAL EFFUSION: SIZE • SMALL: echo free space present posterior and < 1 cm. • MODERATE: echo free space present anterior and posterior < 1 cm. • LARGE: echo free space anterior and posterior > 1 cm.
Small Pericardial Effusion
Moderate Pericardial Effusion
Large Pericardial Effusion
PERICARDIAL EFFUSION: POSSIBLE SOURCES OF FALSE POSITIVES • • • Pleural effusion Pericardial tumor or cyst Dilated coronary sinus LV pseudoaneurysm Large hiatal hernia
LSVC Dilated Coronary Sinus
Pericardial Cyst Subcostal
2 C: Posterior echo free space
DOPPLER • Assessment of flow velocities across mitral/tricuspid valves, LV outflow, and hepatic veins • Presence of respiratory variation > 20% in left heart flow velocities and more marked in right heart • Should be performed in all patients with suspicion or evidence of pericardial disease
Tamponade Case Study
Pericardiocentesis • Needle aspiration of the pericardial effusion • Usually performed with needle entering subxiphoid • Echo guided – Evaluate fluid initially from subcostal – Imaging performed from the apical position
Little effusion available from subcostal
Differentiation with Ascites
Case 2 • • • 56 year old female transferred from outside hospital know breast cancer possible malignant pericardial effusion Pericardiocentesis
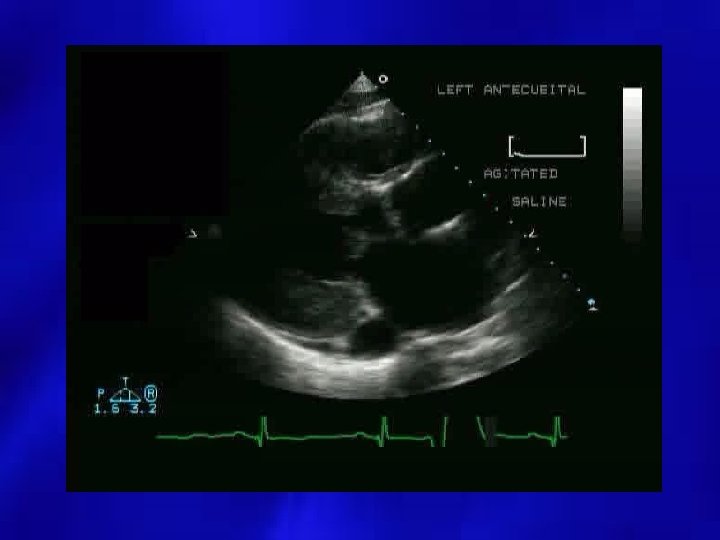
Agitated Saline - injected into the pericardial space for verification of needle placement
Before After pericardiocentesis
Case 4 • Patient presents post MI • New pericardial effusion • What is the differential?
EP application • 56 year old female comes into the hospital after being discharged from outside hospital after pacemaker insertion • Continued severe chest pain • When pacer activated, diaphragm stimulated
Pericardial Effusion by TEE
Pericardial Disease: Constriction versus Restriction
Constrictive Pericardial Diseases: Etiologies • • • Idiopathic/recurrent pericarditis Post cardiac surgery Prior chest radiation Infectious (Tuberculosis) Metastatic process Difficult diagnosis to establish
Less Common Etiologies • • Infectious (Fungal) Neoplasms Uremia Connective tissue disorders (SLE, Scleroderma) • Drug Induced (Procainamide, hydralazine) • Trauma • Post MI (Dressler’s)
Clinical Signs • • • Shortness of breath Peripheral edema Increased jugular venous pressure Normal heart size on chest X ray Similar in presentation to CHF Often confused with restrictive cardiomyopathy
Physiology • Dissociation between intrathoracic and intracardiac pressures • Normally with inspiration, intrathoracic pressure falls and intrathoracic structures fall • In constriction, the pressure change is not transmitted to intrapericardial structures and cavities
2 D Imaging • Pericardial thickening – TEE more reliable than TTE, but CT or MRI is the better method for thickness evaluation • Paradoxical septal motion – Respiratory Variable – Septal shift leftward with inspiration • Increased IVC diameter, lack of resp change
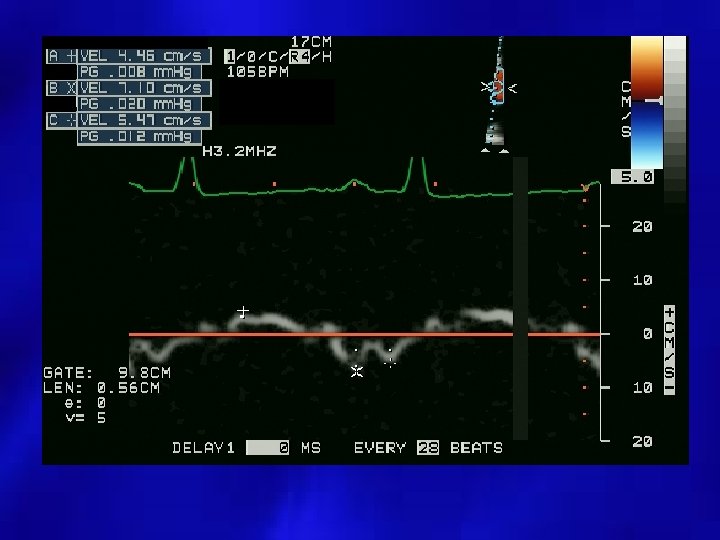
M-mode Evaluation • Parietal pericardial tracking with epicardial/endocardial motion • M Mode posterior LV wall motion is flat during mid and late diastole • Respiratory variation in ventricular chamber size
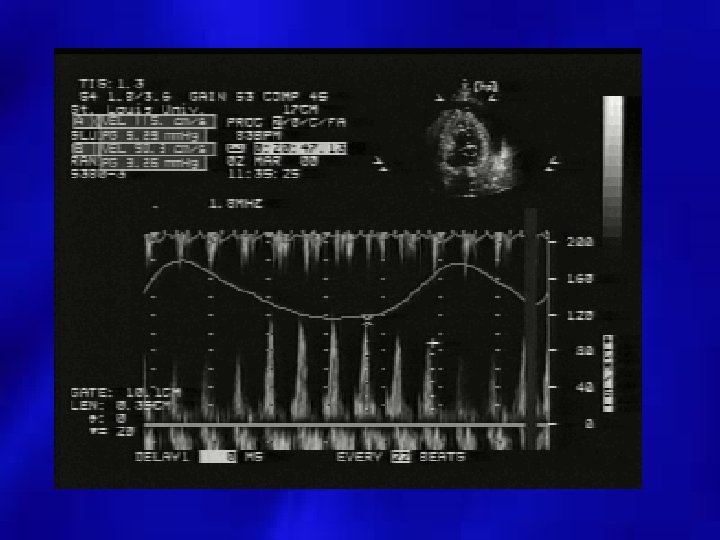
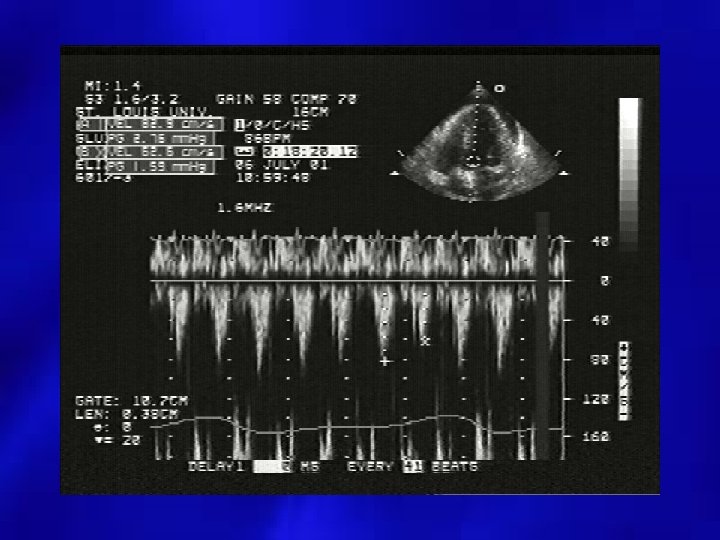
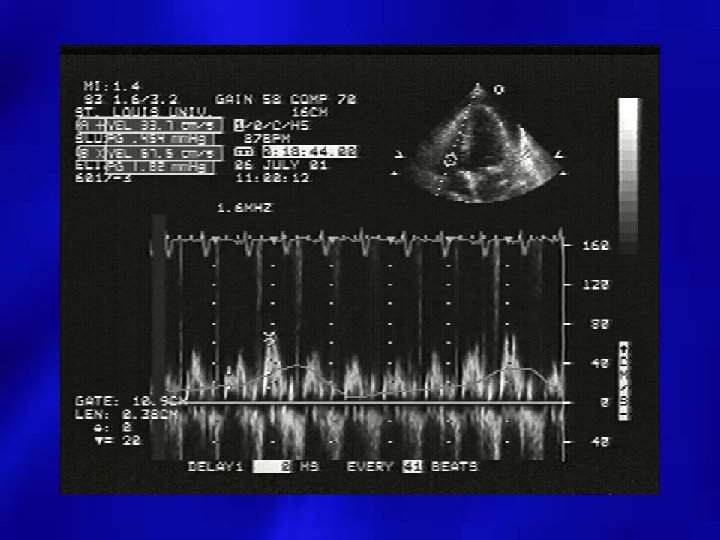
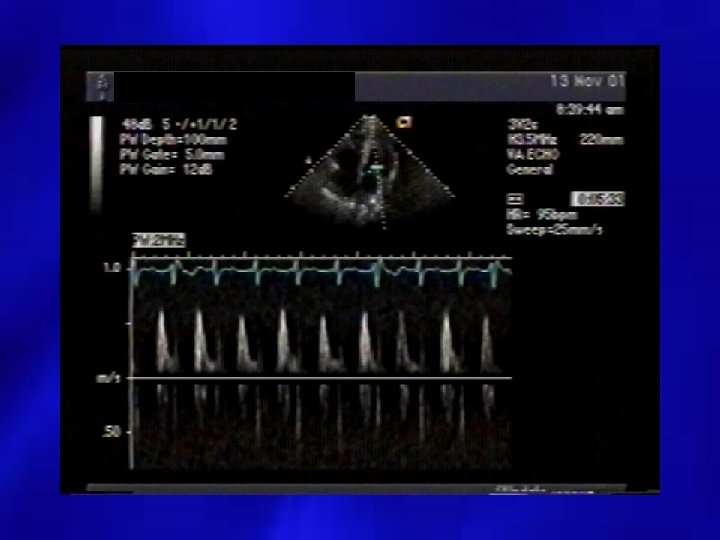
Doppler Evaluation • Pulsed Doppler respiratory flow velocity variation at mitral valve, pulmonary veins – Variation greater than 25% – Left side velocities decrease with inspiration – Diastolic Decrease in PV velocities – Right side increases with inspiration • Shortened mitral deceleration time that decreases more with inspiration
Decreased Mitral Inflow with Inspiration
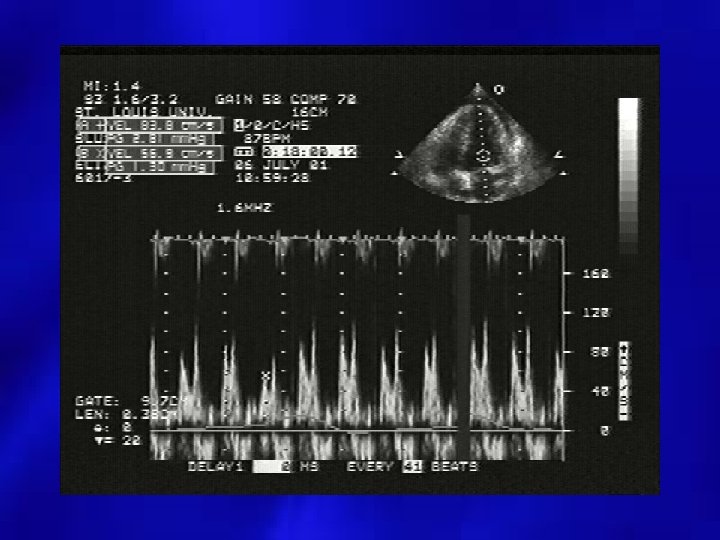
Tricuspid Inflow Increased with Inspiration
Tissue Doppler • In 20 to 40% of patients, Mitral filling may not meet criteria • Sitting patient reduces preload and may reveal variation • Tissue Doppler provides best marker for detection of constriction • TDI velocity >8 -15 cm/sec is diagnostic to rule out restriction Ha et al. JASE 2002; 15: 1468 -71.
Constrictive Tissue Doppler E/E’ and PCWP are inversely correlated in patients with constrictive disease Mitral -Increased E/A ratio Tissue Doppler –Increased Tissue Velocities • Note E/e’ is “normal” despite increased filling pressures due to increased longitudinal annular motion in Constrictive processes Ha et al, Circulation. 2001; 104: 976 -978
Additional Doppler findings • Expiratory decrease in hepatic diastolic forward flow and increases in hepatic vein flow reversals
Normal Hepatic Flow Systolic and diastolic phasic flow
Constrictive Hepatic Vein Flow Increased forward flow with inspiration, backflow with expiration Adapted from Haley et al JACC, 2004; 43; 271 -275
Technical Concerns • COPD – May cause respiratory variability but not usually at the onset of inspiration/expiration – Mitral Inflow pattern is not necessarily increased E/A ratio as in constriction – SVC flow varies in COPD, not in constriction
Constriction Case
Mitral Inflow
Tissue Doppler Medial Lateral
Apical 4 Chamber view
Cardiac Catheterization Calcification LV function
Infiltrative/Restrictive Systemic Diseases
Etiology • Noninfiltrative – – – Idiopathic Familial HCM Scleroderma Diabetic • Infiltrative – Amyloidosis – Sarcoidosis • Storage – Hemochromatosis – Fabry’s • Hypereosinophilic Syndrome • Carcinoid
2 D Findings • • • Bilateral Atrial Enlargement Normal LV cavity size and function Hyperechoic Myocardium Possible Pericardial Effusion Dilated Hepatic Veins Granular appearance of the myocardium “Ground glass”
Amyloid Parasternal Long
Amyloid Apical 4
Doppler Findings • Mitral Filling (Late) – Increased E to A – Shortened Deceleration Time • Pulmonary and Hepatic Veins – Prominent Early Diastolic Filling – Increased Reversed Flow during Atrial Contraction • Pulmonary Hypertension
Restrictive filling
Hepatic Veins Prominent diastolic reversal (Y decent)
Indices of patients with elevated LV filling pressures • • Enlarged LA size (> 28 ml/m 2) E/A ratio > 2 DT <150 Pulmonary Vein S/D < 40% Pulmonary Vein A wave velocity > 25 cm/s E/e’ ratio > 15 Vp flow propagation < 40 cm/sec
Mitral / Tricuspid Inflow Constriction vs Restriction Normal I Mitral Tricuspid Constriction E I E Restriction I E
Tissue Doppler Constrictive • Average velocities 14. 8 cm/sec • Normal or enhanced longitudinal expansion Restrictive • Average velocities 4. 1 cm/sec • Restricted myocardial motion • Increases sensitivity to detect Constriction to 98. 4% • except in pts with MAC, LV dysfunction Garcia, et al. JACC 1996 Jan; 27(1): 108 -14, Sengupta et al. Am J Cardiol. 2004 Apr 1; 93(7): 886 -90
Mixed Constrictive/ Restrictive Physiology • Incidence varies, but around 20% of patients • May be found in Radiation Induced, CABG • Increased Mortality in Mixed physiology
Comparison Restrictive Constrictive LV wall thickness Increased Normal LA diameter Increased E/A ratio Increased Decel time Shortened IVRT Shortened LV diameter Decreased Normal Peak E wave Increased Palka et al. Circulation 2000; 102; 655 -662.
Normal Restrictive Constrictive Mitral Tissue S D S D Pulmonary Vein Tricuspid S D S Adapted From Hoit, Management of Effusive and Constrictive Pericardial Heart Disease Circulation 2002; 105; 2939 -2942 Hepatic Veins D
Case 1 Restrictive vs. Constrictive • 68 year old male • Admitted with shortness of breath • Known history of Amyloidosis
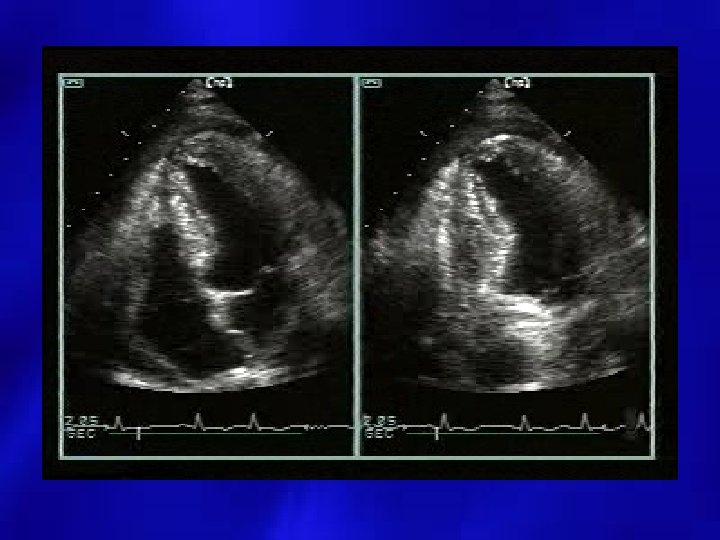
INS EXP
INS EXP
INS EXP
INS EXP