Measles is an acute highly contagious viral disease













 Positive for Ig. M")
 Roseola infantum (exanthem subitum) Infectious mononucleosis meningococcemia Drug rashes.")

























- Slides: 42
Measles is an acute highly contagious viral disease caused by measles virus
Etiology/agent factor paramyxovirus. morbillivirus it is spherical in appearance , measuring about 100~150 nm in diameter ØIt has an outer envelope composed of Mprotein, H-protein, F-protein, and internal core is RNA. Ø Only one antigenic type of measles virus is known.
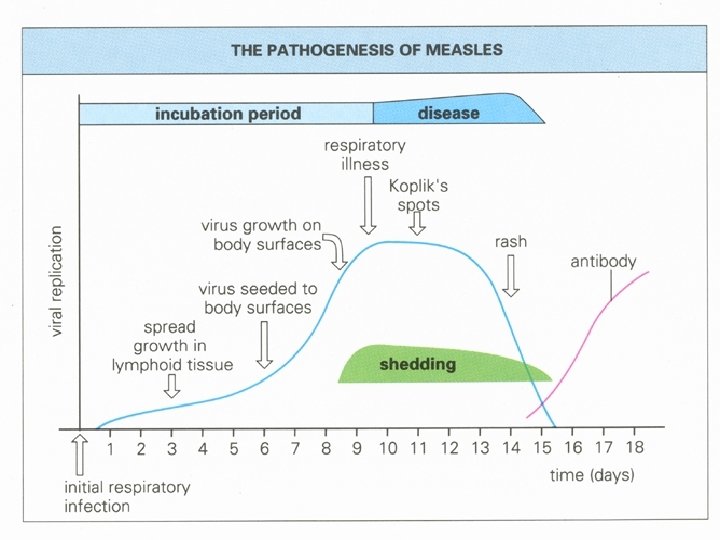
Agent factor Source of infection • cases. of measles, but not carriers No animal reservoir • . Communicability - Highly infectious during prodromal period and at the time of eruption Infective period - 3 days before and 5 days after the appearance of rash Secondary attack rate> 80%
Host factors Age- 6 months to 3 years even up to 10 years Immunity – life long immunity lack of vaccination (need cold chain) poor hygiene vitamin A deficient -> low mucosal defense Incidence equal in both sexes Malnourished children are susceptible
PATHOGENESIS measles virus respiratory tract epithelial cells(multiply lymphoid tissue Primary viremia Reticuloendothelial cells ↓ blood ( 2 ndry viremia)) general toxic symptoms
Clinical features Prodromal stage Eruptive stage Post-measles stage
Measles clinical type Typical type Last 3~4 days. Fever; Catarrhal inflammation of URT; Koplik’s spots; conjunctivitis Incubation period is approximately 7~18 days. Atypical measles Mild measles Hemorrhagic measles Toxic and shock like measles
Koplik ‘s spot
COMPLICATIONS Bronchopneumonia diarrhea Myocarditis Encephaliti s Otitis media Flare-up of T. B SSPE Laryngitis;
Measles encephalitis sequelae deafness seizures mental disorders 1/1000 cases
SSPE sub-acute sclerosing panencephalitis –inflammatory disease –defective virus (often lacking M protein early infection with measles is a risk factor decrease since vaccination program rare (7/1, 000 cases of measles)
IMMUNOSUPPRESSION AND MEASLES TEMPORARY DEPRESSION OF IMMUNE RESPONSE Tuberculin +ve individuals may temporarily become ve MAY GET REACTIVATION OF HERPES, TUBERCULOSIS Don’t see with vaccine strain
DIAGNOSIS Serodiagnosis Significant increase in Ig. G (need two samples) Positive for Ig. M Isolation RT-PCR
DIFFERENTIAL DIAGNOSIS Rubella (German measles) Roseola infantum (exanthem subitum) Infectious mononucleosis meningococcemia Drug rashes.
Treatment Supportive and symptomatic Vit-A 2 lacs IU given orally for 2 days in children older than 1 yr Treatment of complication
Prognosis Self limiting ds , unless complicated Recovery prolonged with respiratory complication Deaths may occur Mortality 90% of deaths due to respiratory or neurological Respiratory complication more common in young child Neurological complication more common in older children
Prevention . Protection person. Control source of infection Interruption of transmissions of the susceptible 1. Active immunization. Lived attenuated measles vaccine. 2. Passive immunization. gamaglobulin
M u m p s Mumps is an acute self limiting disease characterized by fever, parotid swelling and tenderness
Etiology Paramyxovirus, Single stranded R. N. A virus Single strain known Human is only reservoir
Epidemiology Age : 5 -9 yrs Infective period : 7 days before and 7 days after appearance of parotid swelling Winter and spring Spread by droplets Isolation: 5 dayss after appearance of parotid swelling
Pathogenesis Infection Replication in resp. epithelium Lymph node viremia Salivary glands, CNS , pancreas, testis, thyroid, ovaries, heart, kidne ys, liver and synovia.
Clinical features Incubation period : 16 -18 days Asymptomatic to mild non specific symptoms Typical presentation start with prodrome , lasting 1 -2 days and consisting of fever, headache, vomiting, body ache, Parotitis , usually bilateral in 70% Submandibular gland may also be involved
Diagnosis Mainly clinical Leucopenia with relative lymphocytosis, raised serum amylase ↑Ig. G between acute and convalescent sample Virus isolation
Differential diagnosis Parotid swelling may caused by other infection and noninfectious condition. Influenza and para influenza virus CMV , EBV, enterovirus, HIV, Purulent parotitis –S. aureus. Obstruction to stensons duct, collagen vascular ds
complication Abortion Meningoencephaliti s Orchitis and oophoritis pancreatitis myocarditis Conjunctiviti s thyroiditis nephritis arthritis Optic neuritis pneumonia thromboc ytopenia
Treatment No specific treatment Prognosis Excellent even when complicated by meningoencephalitis
Prevention Live attenuated vaccine Given along with MMR Efficacy-90% 2 doses , at 16 -18 months and at 5 yrs
Rubella German measles 3 day measles Mild exanthematous disease of infants and children Major clinical significance : transplacental infection and congenitatl reubella syndrome
Etiology Togaviridae Single stranded RNA Ultrasensitive to light , heat and uv rays 3 structural protiencore, E 1, E 2 Human is only revervoir
Epidemiology Preschool and school age Incidence decreased CRS incidence decreased
pathogenesis Infection Most important risk factor for severe congenital defect is the gestational age at the time of infection Replication in respiratory epithelium Regional lymph node clinical symptoms viremia
Clinical manifestation Post natal rubella is mild, self limiting infection , difficult to differentiate from other viral illnesses Prodrome phase: low grade fever, sore throat , red eyes , headache , malaise , LN pathy. Forchhiemer spo: tiny red colored lesion on oropharynx Subclinical infection are common In children ist manifestation of rubella is rash, begin on face and neck, small irregular macule and progress extremities. rash last for 3 days 25 -40% of children may not have rash
Differential diagnosis Measles Mycopl asma Adenovi rus Entero viruses Erythe ma infectio sum Epstien –Barr virus
Complication Post infectious thrombocytopenia • 2 wks after onset of rash • Self limiting Arthritis • Begins within 1 week of onset of exthanthem • Self limiting • Most serious complication of post natal rubella • Onset within 7 days after the onset of rash • Some times progressive rubella panencephalitis Encephalitis CRS
CONGENITAL RUBELLA SYNDROME In 1941 an ophthalmologist described a syndrome of cataract and congenital heart ds associated with maternal infection with rubella. Cataract and retinopathy deafness Congenital heart disease LBw Psychomotor retardation Microcephaly Intracranial calcification Neonatal purpura
CRS contd…… Most common complicationnerve deafness Unilateral or b/l cataract are most severe ocular complication encephalitis PDA is most common cardiac defect PRP
Treatment No specific Tt. Supportive Tt. Long term follow –up for CRS
Prognosis Postnatal rubella CRS Excellent prognosis Poor prognosis No long term follow-up Long term follow-up
Prevention Live attenuated RA 27/3 strain Two doses along with measles and mumps At 15 -18 months and 5 yrs