Viral infection Viral meningitis Viral infection is the



 Mumps Influenza Herpes simplex Varicella zoster Epstein-Barr HIV")



 in adults")







 vaccine. • In developed countries where polio is")
- Slides: 19
Viral infection
Viral meningitis Viral infection is the most common cause of meningitis, and usually results in a benign and self-limiting illness requiring no specific therapy. It is a much less serious illness than bacterial meningitis unless there is associated encephalitis.
Clinical features The condition occurs mainly in children or young adults, with acute onset of headache and irritability and the rapid development of meningism. In viral meningitis, the headache is usually the more severe feature. There may be a high pyrexia, but focal neurological signs rarely occur.
Viruses Enteroviruses (echo, Coxsackie, polio) Mumps Influenza Herpes simplex Varicella zoster Epstein-Barr HIV
Investigations The CSF usually contains an excess of lymphocytes, but glucose and protein levels are commonly normal or the protein level may be raised. Management There is no specific treatment and the condition is usually benign and self-limiting. The patient should be treated symptomatically in a quiet environment. Recovery usually occurs within days, although a lymphocytic pleocytosis may persist in the CSF.
VIRAL ENCEPHALITIS • Common viruses causing viral encephalitis Arboviruses Enteroviruses HSV
Pathology Inflammation can occur in the cortex, white matter, basal ganglia and brain stem, and the distribution of lesions varies with the type of virus. In herpes simplex encephalitis, the temporal lobes are usually primarily affected. Clinical features Viral encephalitis presents with acute onset of headache, fever, focal neurological signs (aphasia and/or hemiplegia) and seizures. Disturbance of consciousness ranging from drowsiness to deep coma. Meningism occurs in many patients.
Herpes simplex encephalitis The majority of cases of herpes simplex encephalitis (HSE) in adults are caused by HSV-1. 10% are caused by HSV-2, usually associated with immuno-compromise or occurring in the neonate. The herpes virus leads to inflammation, infection and necrotizing lesions particularly in the inferior and mesial temporal lobes which may also involve the orbital frontal cortex and limbic structures.
Route of infection Primary infection usually develops in the oropharyngeal mucosa before the virus is transported by retrograde transneuronal spread via the trigeminal nerve to establish latency in the olfactory bulb or trigeminal ganglion.
Clinical feature The onset of HSE is with fever, headache and alteration of consciousness which may develop gradually or rapidly over amatter of hours. The most common manifestations are personality change, dysphasia with progressive behavioral disturbance and occasional psychotic features. Less typical features include the development of hemiparesis or a visual field defect (particularly superior quadrantic). Focal or generalized seizures are often associated with olfactory or gustatory hallucinations
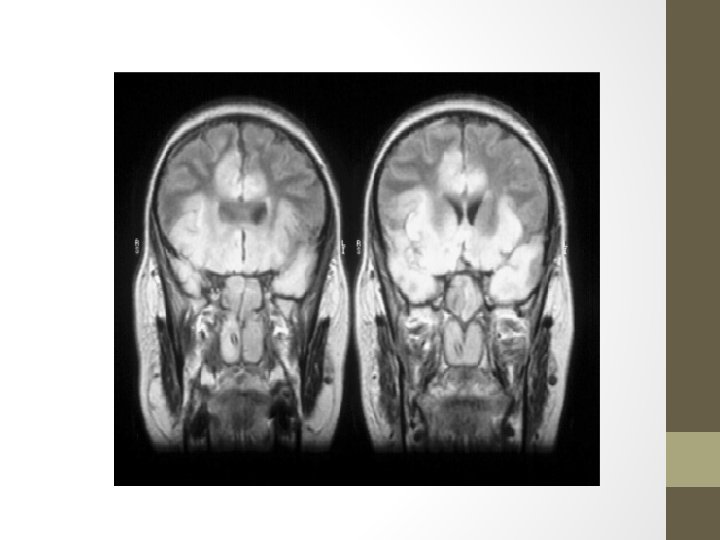
• Diagnosis q. The EEG show periodic sharp-wave complexes from temporal lobe on low amplitude background q. CT-scan low density lesion within the temporal lobe with mass effect. q. MRI-high signal intensity on T 2 q CSF-Lymphocytic pleocytosis, elevated protein, normal or glucose q. PCR to detect HSV DNA in CSF q. CSF may contain RBCs (due to necrosis in the brain tissue)
• Treatment: / Acyclovir (10 mg Kg every 8 hour IV for more than 1 hr for 3 weeks) +good hydration Anticonvulsant therapy (seizure occur in 30%), so Clonazepam, or phenytoin are recommended
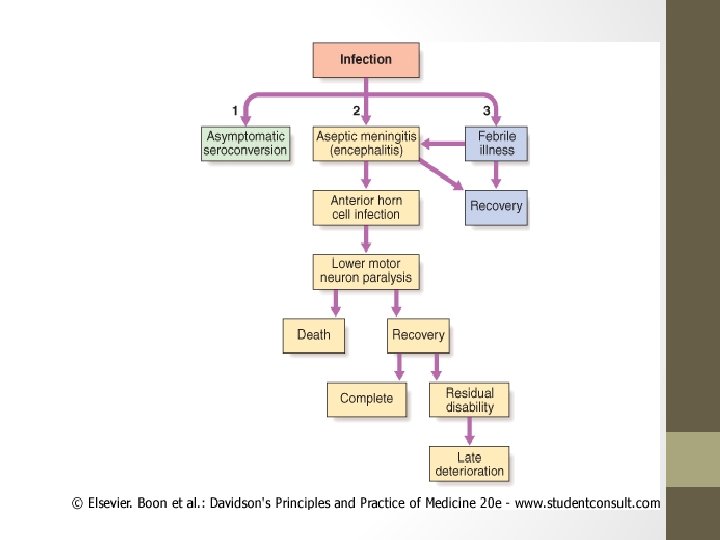
POLIOMYELITIS • The disease is caused by one of three polioviruses, which are a subgroup of the enteroviruses. • It is much less common in developed countries following the widespread use of oral vaccines but is still a problem in the developing world. • Infection usually occurs through the nasopharynx.
• The virus causes a lymphocytic meningitis and infects the grey matter of the spinal cord, brain stem and cortex. • There is a particular propensity to damage anterior horn cells, especially in the lumbar segments.
Prevention • immunisation with live (Sabin) vaccine. • In developed countries where polio is now very rare, the live vaccine has been replaced by the killed vaccine in childhood immunisation schedules management • In the early stages, bed rest is imperative because exercise appears to worsen the paralysis or precipitate it. • At the onset of respiratory difficulties, a tracheostomy and ventilation are required. Subsequent treatment is by physiotherapy and orthopaedic measures.