Pleural procedures Dr anan esmail parietal pleura supplied







")
")
")
")


")


 Transudate, some exudates Red (bloody)")




 Lymphocytes malignancy Lymphoma > 80% chronic rheumatoid pleurisy")











 Histological confirmation")





























- Slides: 64
Pleural procedures Dr. anan esmail
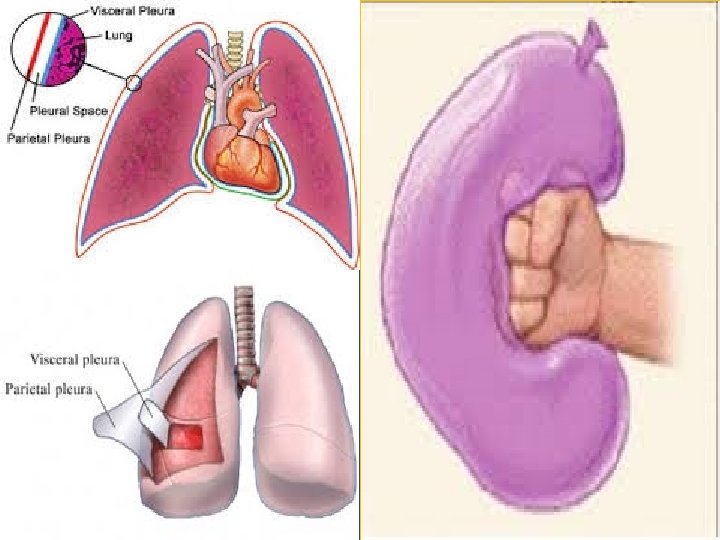
parietal pleura supplied by systemic capillaries nerve ending visceral pleura supplied by bronchial capillaries no nerve ending
In the normal pleural space there is approximately 0. 1 - 0. 2 m. L/kg body weight of pleural fluid (PF)
The formation of PF is a function of parietal pleura
The PF then moves Into lymphatic ducts
Pleural disease • Pleural Effusions • Pneumothorax • Mesothelioma
Pleural Effusions mechanisms that lead to accumulation of pleural fluid? ?
Pleural Effusions Increased hydrostatic pressure in microvascular circulation (congestive heart failure)
Pleural Effusions Decreased oncotic pressure in microvascular circulation (Hypoalbuminemia )
Pleural Effusions Impaired lymphatic drainage from the pleural space (malignant effusion)
Pleural Effusions Movement of fluid from peritoneal space (ascites )
Pneumothorax air in the pleural space
Pneumothorax Classification Spontaneous Traumatic Iatrogenic
Mesothelioma malignant tumor of the pleura (asbestos)
Pleural investigation diagnostic procedures Therapeutic procedures
Indications For Thoracentesis new finding of a pleural effusion
observation Suggested diagnosis Color of fluid Pale yellow (straw) Transudate, some exudates Red (bloody) Malignancy, BAPE, PCIS, or pulmonary infarction if trauma Excluded White (milky) Chylothorax or cholesterol effusion; EVM of CVC be established atwith thelipid infusion brown Some diagnoses can bedside by visual inspection of the fluid Long-standing bloody effusion; rupture of amoebic liver abscess black Aspergillus niger infection Yellow-green Rheumatoid pleurisy Greenish tint Biliopleural fistula
Character of fluid Pus Empyema Viscous Mesothelioma Turbid Inflammatory exudates Satin-like sheen Cholesterol effusion Looks like urine Urinothorax Odor of fluid Putrid Anaerobic Empyema Ammonia Urinothorax
Pleural fluid serum CBC glucose Protein LDH
Normal Pleural Fluid less than 500 nucleated cells/L 2% neutrophils 0% basophils 7 - 11% lymphocytes 61 - 77% macrophages 9 -30% mesothelial
nucleated cell count virtually never diagnostic some settings in which the count may be helpful: above 50, 000/micro. L • complicated parapneumonic effusions above 10, 000/micro. L • pancreatitis, lupus pleuritis
Tuberculous (most common) Lymphocytes malignancy Lymphoma > 80% chronic rheumatoid pleurisy
PF eosinophilia Causes: Pneumothorax PF eosinophil count of > 10% of the total nucleated cells Hemothorax fungal disease Parasitic disease drug induced Churg strauss
Pleural fluid serum CBC glucose Protein LDH
low pleural fluid glucose concentration Rheumatoid pleurisy parapneumonic effusion or empyema Malignant effusion Lupus pleuritis Esophageal rupture
Pleural fluid serum CBC glucose Protein LDH
The Light's Criteria traditional method of differentiating Transudates And exudates
if at least one of the following three criteria is present, the fluid is defined as an exudate: Pleural fluid protein/serum protein ratio greater than 0. 5 Pleural fluid LDH/serum LDH ratio greater than 0. 6 Pleural fluid LDH greater than twothirds the upper limits of the laboratory's normal serum LDH
the fluid is defined as an exudate if: Pleural fluid protein greater than 2. 9 g/d. L (29 g/L) Pleural fluid cholesterol greater than cholesterol 45 mg/d. L Pleural fluid LDH greater than 0. 45 times the upper limit of the normal serum LDH
Processes that always cause a transudative effusion
Processes that may cause a transudative effusion, but usually cause an exudative effusion
Causes of exudative pleural effusions Infectious Bacterial pneumonia Tuberculous Malignancy Pancreatitis Pulmonary embolism Postcardiac injury syndrome Chylothorax Hypothyroidism Lupus pleuritis Rheumatoid pleurisy
exudative pleural effusions clinical history physical examination imaging studies thoracentesis with chemical Cytological are sufficient to obtain a definitive diagnosis
exudative pleural effusions When the underlying pathology remains undiagnosed (25% of cases) Histological confirmation is required
Closed pleural biopsy useful in conditions where the pleura is diffusely involved
Closed pleural biopsy considered in the setting of an undiagnosed lymphocytic effusion lymphocytes is greater than 80 percent
Closed pleural biopsy The diagnostic yield of a closed pleural biopsy is 70 to 90 percent in exudative pleural effusions due to tuberculosis
Closed pleural biopsy greater number of biopsies increase the sensitivity
Closed pleural biopsy Ultrasound guidance can improve the yield of percutaneous biopsy
Closed pleural biopsy Pneumothorax complicated 11 percent
CT guided cutting needle biopsy is typically used to diagnose malignancy
CT guided cutting needle biopsy sensitivity of 87 percent in patients with suspected malignant effusions with negative cytology
CT guided cutting needle biopsy pneumothorax occurred in only 4 percent of cases
thoracoscopy diagnostic thoracoscopy Therapeutic thoracoscopy
thoracoscopy percutaneous insertion of an endoscope into the pleural space
thoracoscopy Thoracoscopy can be performed under either local or general anesthesia
thoracoscopy It can be used to directly visualize and collect specimens from both the pleura and pleural space
thoracoscopy Thoracoscopic pleural biopsy has a diagnostic yield for malignant pleural effusions that is superior to percutaneous pleural biopsy
advanced disease associated with greater sensitivities sensitivity of cytology 45 to 90% percutaneous pleural biopsy 30 to 50% CT guided needle biopsy 87% biopsy with thoracoscopy 95 to 100%
Pleural investigation diagnostic procedures Therapeutic procedures
Chest tube Thoracostomy tube placement into the pleural cavity performed to drain abnormal collections of air or fluid
Chest tube Indications pneumothorax
Chest tube Indications hemothorax
Chest tube Indications chylous effusion
Chest tube Indications malignant effusion
Chest tube Indications parapneumonic effusion empyema
strong indicators for the need for pleural space drainage PF p. H ˂7. 20 Glucose < 60 mg/d. L or a high LDH > 1000 IU/L positive bacterial culture p. H is the most sensitive of these parameters
pleurodesis instillation of a sclerosing agent over the pleural surfaces The sclerosant agents used most commonly are talc and doxycycline
pleurodesis Doxycycline is a less effective alternative to talc
pleurodesis Talc slurry administered via chest tube appears equally effective compared with aerosolized talc administered via insufflation during thoracoscopy
pleurodesis indication Malignant pleural effusion refractory nonmalignant pleural effusions recurrent primary spontaneous pneumothorax secondary spontaneous pneumothorax
pleurodesis adverse effects Pain Fever gastrointestinal symptoms