PAPULOSQUAMOUS DISEASES Psoriasis Lichen planus Lichen nitidus Pityriasis

 • Psoriasis • Seborrheic dermatitis")








 • This disorder can be a life-threatening medical")
, “distal”, asymmetric oligoarthritis Mutilating arthritis")

 • Factors influencing selection of treatment: – Age – Type of psoriasis")
 • Localized psoriasis – – – – – Topical glucocorticoids Intralesional triamcinolone")
 • Generalized psoriasis – – – – Narrow-Band UVB Phototherapy Oral PUVA")








 PSORIASIS • lesions may be localized in the major skin folds, such")






















, puberty, •")
 Immune responses to Malassezia furfur (P. ovale): Part of the •")







- Slides: 70
PAPULOSQUAMOUS DISEASES • Psoriasis • Lichen planus • Lichen nitidus • Pityriasis rosea • Pityriasis rubra pilaris • Seborrheic dermatitis • Pityriasis lichenoides et varioliformis acuta • Parapsoriasis
PAPULOSQUAMOUS DISEASES (II) • Psoriasis • Seborrheic dermatitis
PSORIASIS Psoriasis is a common, genetically determined, inflammatory and hyperproliferative skin disease. Psoriasis is a hereditary disorder of skin with several clinical expressions. The most frequent type is psoriasis vulgaris, which occurs as chronic, recurring, scaling papules and plaques.
CLASSIFICATION • Psoriasis vulgaris – Acute guttate – Chronic plaque – Inverse – Palmoplantar • Psoriatic erythroderma • Pustular psoriasis • Psoriatic arthritis
PSORIASIS VULGARIS
Epidemiology • Age of onset: May begin at any age. Uncommon < 10 years. Early: • • • Peak incidence at 22. 5 years of age (in children the mean age of onset is 8 years). Late: About age 55. Sex: Equal incidence. Race: Low incidence in West Africans, Japanese; very low incidence or absence in North and South American Indians. Heredity: Polygenic trait. HLA-B 13, B 17, Bw 57, HLA-Cw 6 ( aerlier age of onset and with a positive family history) Triggering Factors: Physical trauma (Koebner’s phenomenon), infections (acute streptococcal), stress, drugs ( glucocorticoids, lithium, antimalarials, interferon, beta-adrenergic blockers), heavy alcohol, smoking Comorbid disease: Psoriatic arthritis, Crohn’s disease, cancer, depression, non-alcoholic fatty liver disease, metabolic syndrome (or components of it), cardiovascular disorders.
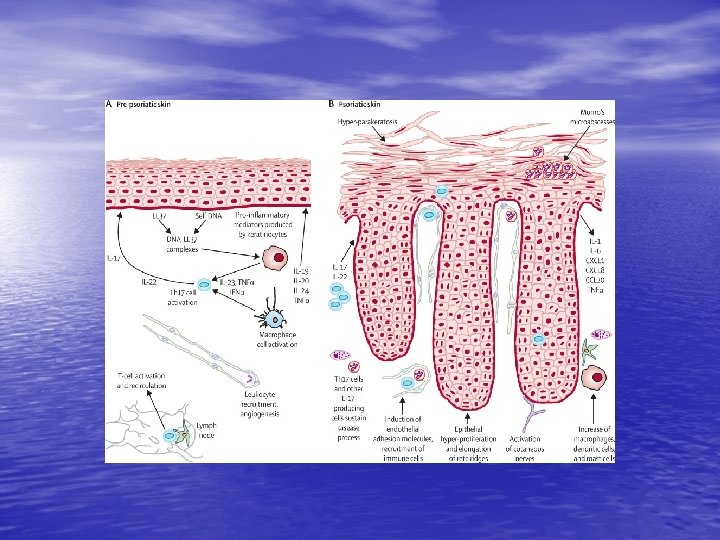
Pathogenesis • A chronic inflammatory disorder with polygenic predisposition combined with • • triggering environmental factors such as trauma, infection, or medication. Psoriasis is a T-lymphocyte-mediated autoimmune disease (mixed Th 1 and Th 17 disease). T cells and cytokines play a pivotale role ( overexpression of type 1 cytokines like IL-1, IL-6, IL-8, IL-12, IFN gamma and TNF alpha ) The underlying pathophysiology involves epidermal proliferation and differentiation, angiogenesis and the cellular immune system. Dysregulated interactions of innate and adaptive components of the immune system with resident cutaneous cell types. 1) Cross-talk between innate (macrophages, mast cells, granulocytes) and adaptive immunity( Tcells) 2) Interleukin-23 / Th 17 axis 3) Effect on resident T cells of the skin (antimicrobial peptides, cytokines and chemokines secreted by keratinocytes act as chemoattractants for infiltrating immune cells) 4)Effect on vascular endothelial cells ( the inflammatory milieu leads to induction and activation of a range of pro-angiogenic factors – VEGF - , TNF alpha-governed proinflammatory environment in psoriatic skin induces endothelial adhesion molecules which facilitate the recruitement of circulating leucocytes in psoriatic skin.
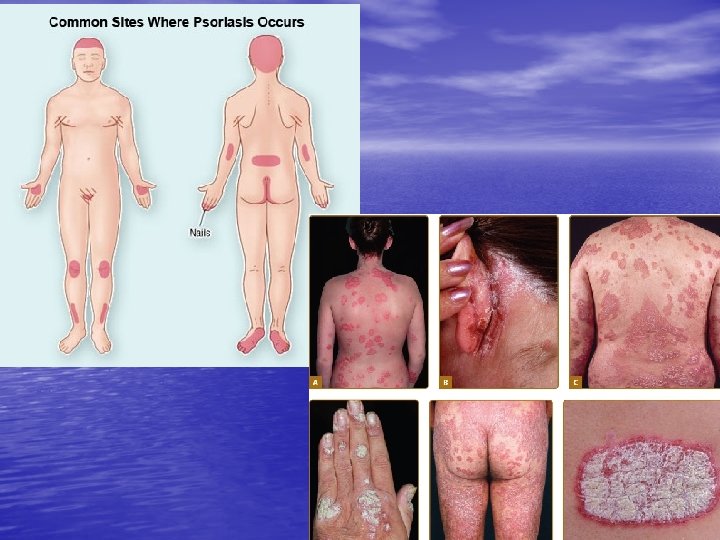
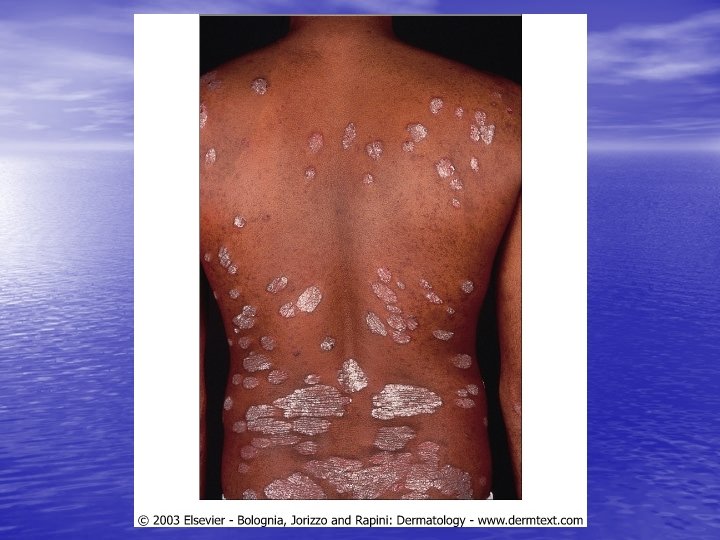
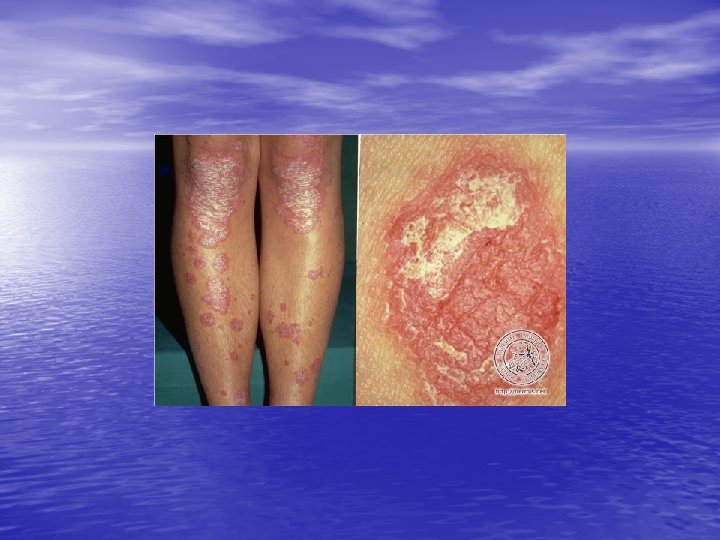
Physical • Acuteexamination Guttate Type: Eruption of small salmon-pink • • papules (guttate: Latin gutta, “drop”), with or without scales, disseminated, generalized, mainly on the upper trunk, strongly associated with streptococcal throat infection, frequent in young adults and children Chronic Stable (plaque) Type: Sharply marginated, dull-red plaques with loosely adherent, lamelar, silvery-white scales. Single lesion or lesions localized to one or more predilection sites: elbows, knees, sacral-gluteal region, scalp, plm/soles. Sometimes only regional involvement(scalp), often generalized. Special Sites – Palms and Soles – Scalp – Inverse Psoriasis (perianal, genital and body folds) – Nails: pitting, subungual hyperkeratosis, onycholysis, the oil spot (pathognomonic)
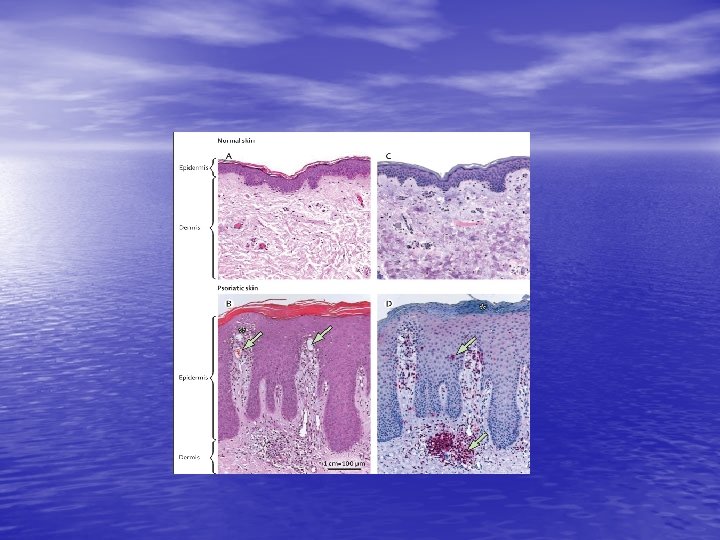
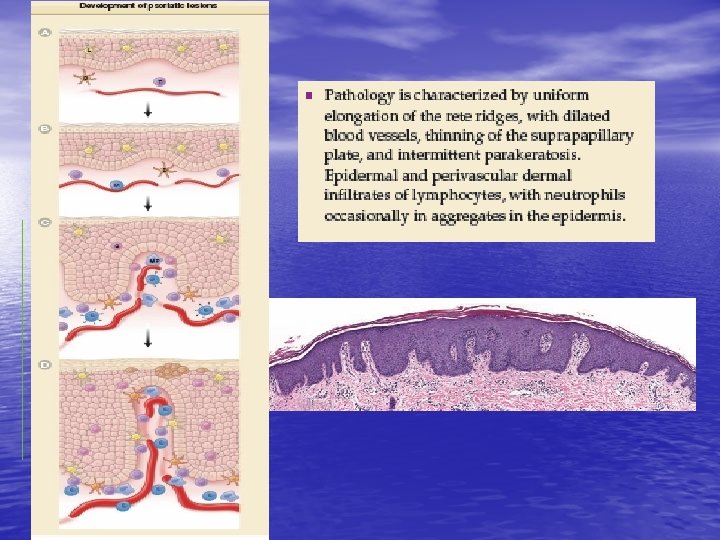
Laboratory examinations • Dermatopathology • Culture: Throat culture
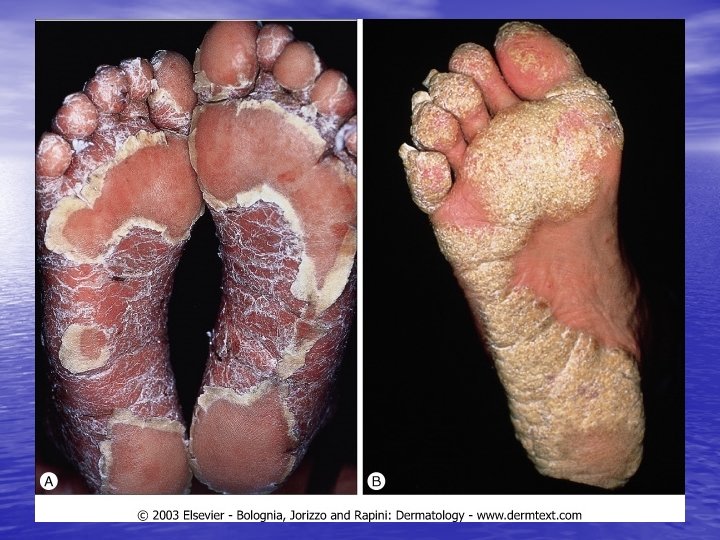
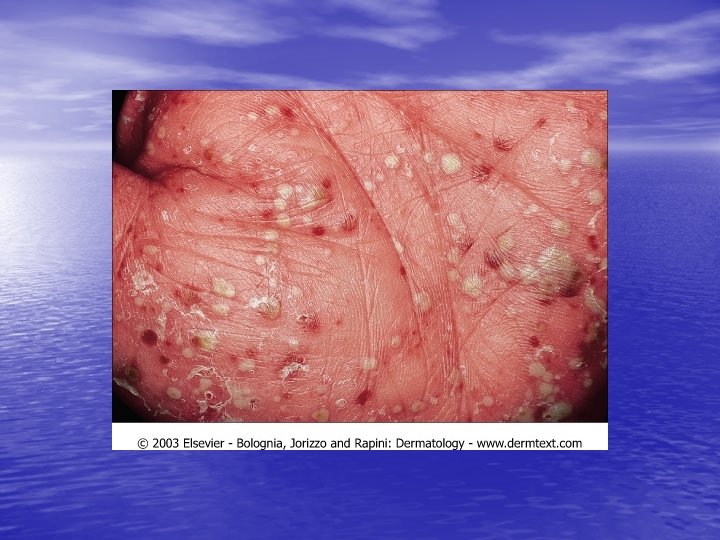
Palmoplantar psoriasis • Chronic, relapsing eruption limited to palms and soles. • • • Numerous very typical sterile, yellow, deep-seated pustules that evolve into dusky-red crusts. Incidence: Low as compared to psoriasis vulgaris Age of onset: 50 to 60 years. More common in females (4: 1) Symptoms: Stinging, burning, itching. Eruptions come and go, in waves. Differential diagnosis: Tinea manus, tinea pedis, dyshidrotic eczema, contact dermatitis, HSV infection. Course: Persistent for years and characterized by unexplained remissions and exacerbations.
Generalized acute pustular psoriasis (Von Zumbusch) • This disorder can be a life-threatening medical • problem with an abrupt onset. It starts with a burning fiery-red diffuse erythema that spreads in hours with pinpoint pustules appearing in clusters. Fever, weakness, severe malaise, fast pulse, leukocytosis, shedding of nails, hair loss, skin tenderness Special types: Impetigo herpetiformis, acrodermatitis continua of Hallopeau
Psoriatic arthritis • • Rare before age 20 Sero(-), “distal”, asymmetric oligoarthritis Mutilating arthritis (bone erosion, osteolysis or ankylosis. “Axial” (sacroiliac, hip, cervical) Dactylitis (sausage fingers) May be present (in 10% of patients) without any visible psoriasis Often psoriatic involvement of fingertips and periungual skin Massive nail involvement by psoriasis is frequent
777
Management (1) • Factors influencing selection of treatment: – Age – Type of psoriasis – Site and extent of involvement – Previous treatment – Associated medical disorders
Management (2) • Localized psoriasis – – – – – Topical glucocorticoids Intralesional triamcinolone acetonide Topical anthralin Topical vitamin D analogues( calcipotriene, 0. 005%, ointment and cream) Topical tacrolimus, 0. 1% Tazarotene ( a topical retinoid, 0. 05 and 0. 1% gel ) Topical dithranol and coal tar Topical PUVA, UVB Salicylic acid Moisturizing
Management (3) • Generalized psoriasis – – – – Narrow-Band UVB Phototherapy Oral PUVA Photochemotherapy Oral Retinoids Methotrexate Cyclosporine Diet Monoclonal Antibodies and Fusion Proteins: Infliximab, Etanercept, Adalimumab, Ustekinumab (IL 12/23)
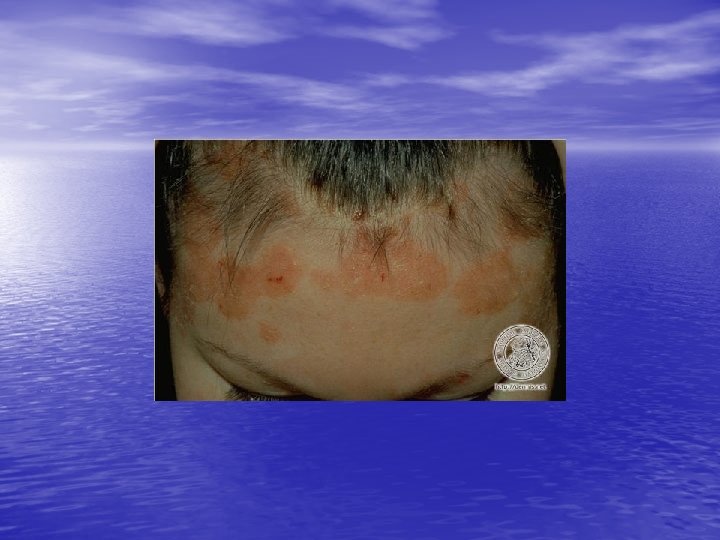
q. GEOGRAPHIC TONGUE Also known as benign migratory glossitis The condition usually presents as asymptomatic erythematous patches with serpiginous borders, resembling a map. These lesions characteristically have a migratory nature.
RELATED PHYSICAL FINDINGS q. NAIL CHANGES IN PSORIASIS.
Ø Generalized Pustular Psoriasis § is a distinctive characterized by acute variant of psoriasis. Attacks are fever that lasts several days and a sudden generalized eruption of sterile pustules 2– 3 mm in diameter. § The pustules are disseminated over the trunk and extremities, including the nail beds, palms, and soles. § The pustules usually arise on highly erythematous skin, first as patches and then becoming confluent as the disease becomes more severe.
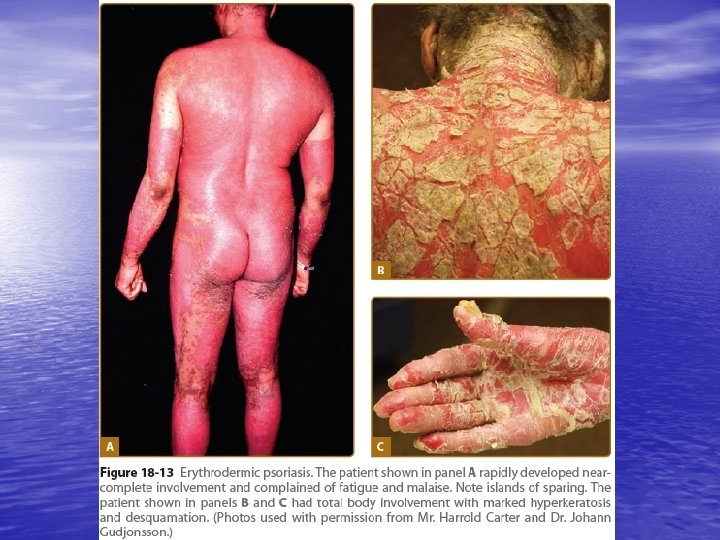
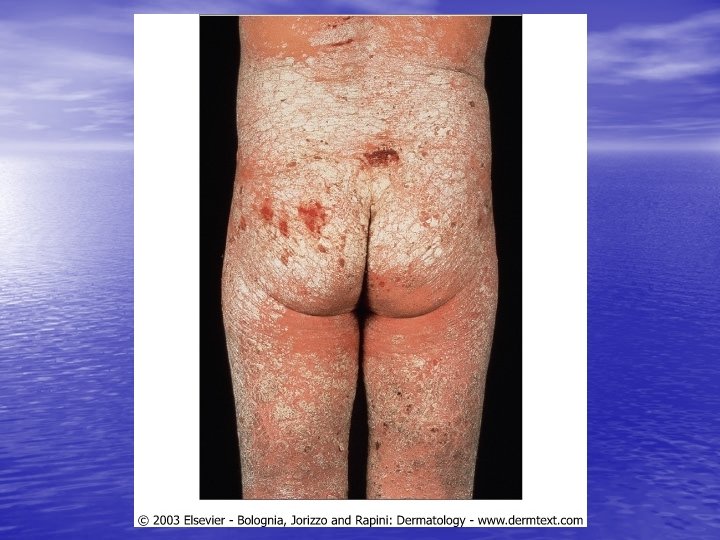
ERYTHRODERMIC PSORIASIS • generalized form of the disease that affects all body sites, including the face, hands, feet, nails, trunk, and extremities • Erythema is the most prominent feature, and scaling is different • Instead of thick, adherent, white scale there is superficial scaling. • Psoriatic skin is often hypohidrotic due to occlusion of the sweat ducts
INVERSE (FLEXURAL) PSORIASIS • lesions may be localized in the major skin folds, such as the axillae, the genito-crural region, and the neck. • Scaling is usually minimal or absent, and the lesions show a glossy sharply demarcated erythema, which is often localized to areas of skin-to-skin contact. • Sweating is impaired in affected areas.
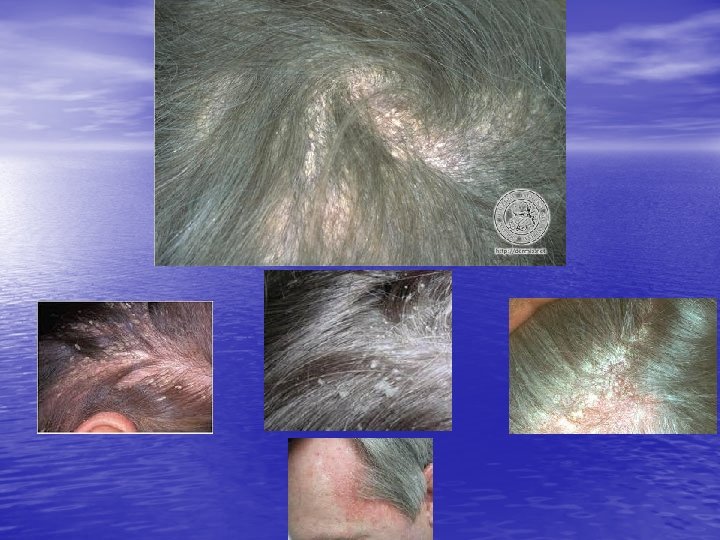
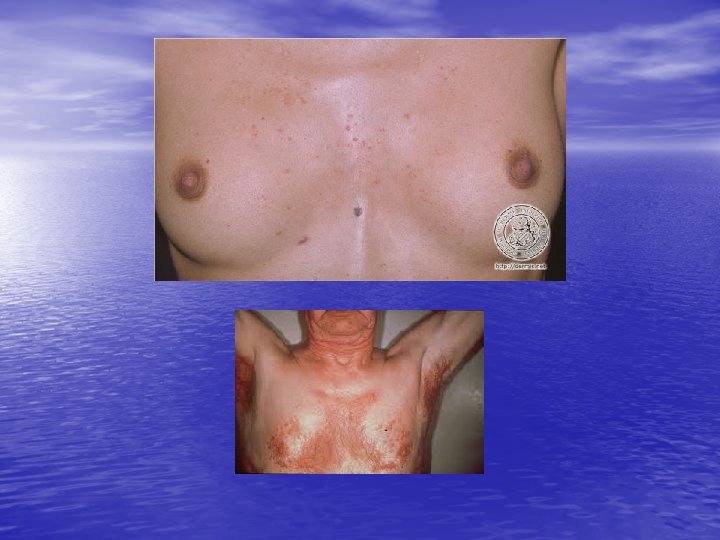
SEBORRHEİC DERMATİTİS SD is a very common chronic dermatosis characterized by redness and scaling and occuring in regions where the sebaceous glands are most active, such as the face and scalp, the presternal area, and the body folds.
EPIDEMIOLOGY AND ETIOLOGY • Age of Onset: Infancy (within the first months), puberty, • • most between 20 and 50 years or older Infantile SD: Usually begins about one week after birth and may persist for several months Adult SD: Chronic relapsing course; dandruff ( pityriasis capitis simplex), non-purulent otitis externa, intertrigo Sex: More common in males Predisposing and Exacerbating Factors: Hereditary diathesis, parkinson’s disease, some neuroleptic drugs, emotional stress, HIV disease
PATHOGENESİS • 1) Immune responses to Malassezia furfur (P. ovale): Part of the • • normal resident skin flora. Studies on the cellular immunity have yielded contradictory results. The inflammation may be irritant ? caused by toxic metabolites, lipase and reactive oxygen species. 2) Active sebaceous glands: Often associated with sebum overproduction. 3) Abnormal composition of the skin surface lipids ( increased triglycerides and cholesterol, decreased squalene and FFA ) and imbalance of the microbial flora
HİSTORY AND SKİN LESİONS • Gradual onset • Seasonal variations: Worse in winter, sunlight ( dual effect) • Pruritus is variable, often increased by perspiration • Hairy areas of head, face, trunk, body folds, genitalia
COURSE AND PROGNOSIS • The condition improves in the summer and flares • • • in the fall. Recurrences and remissions Infantile and adolescent SD disappears with age. Differential diagnosis: Atopic dermatitis, irritant diaper dermatitis, psoriasis, langerhans-cell hystiocytosis, Leiners’ disease, Wiskott Aldrich syndrome
MANAGEMENT • This chronic disorder requires initial therapy • • • followed by chronic maintenance therapy Initial topical therapy: Glucocorticoid cream or lotion, ketoconazole cream, pimecrolimus cream, tacrolimus ointment, medicated shampoos (selenium sulfide, zinc pyrithione, ketoconazole, tar) Systemic therapy: Itraconazole, fluconazole Maintenance therapy