VULVAL SWELLINGS By Dr Ahmad Essmat Lecturer of

VULVAL SWELLINGS By Dr. Ahmad Essmat Lecturer of Ob/Gyn Alexandria University Dep. of Gyne-oncology El-Shatby Maternity Hospital

Anatomy of the vulva

Swellings of the vulva 1 - Benign swellings: A- Swelling related to the various structures of the vulva. B- Swelling appearing ( presenting) at the vulva. 2 - Malignant swellings
 Swellings arising from the vulva: Congenital. . clitorial cysts Traumatic.")
I- Benign swellings A) Swellings arising from the vulva: Congenital. . clitorial cysts Traumatic. . . vulval hematoma Inflammatory: 1. Acute vulvitis 2. Chronic vulvitis : Specific, nonspecific, viral (condyloma acuminata) Vascular: varicose veins, edema, elephantiasis Cystic: 1. Bartholin cyst 2. Dermoid cyst 3. Sebaceous cyst 4. Lymphatic cyst 5. Endometrioma
: papiloma,")
Neoplastic: � Connective tissue: fibroma, lipoma, leiomyoma, neuroma, hemangioma Lymphangioma � Epithelial (Benign): papiloma, adenoma, tumour of the sweet glands (Hydradenoma) Bartholin gland conditions: cyst, abcess, adenoma. .
 Congenital causes: such as 1‑ Congenital")
I -Benign swellings arising from the vulva. I) Congenital causes: such as 1‑ Congenital hypertrophy of the clitoris 2‑ Congenital hypertrophy of the labia
 Traumatic Hematoma Etiology: � Traumatic: injury by a blunt object or a kick")
II) Traumatic Hematoma Etiology: � Traumatic: injury by a blunt object or a kick � Operative: as incomplete haemostasis at the time of episiotomy � Spontaneous: as ruptured varicose veins C. P � Swelling: tender, painful, bluish and of rapid onset. � Pressure symptoms. Treatment of traumatic hematoma of the vulva � Small & not increasing: conservative treatment: ice packs to followed by hot fomentation to help absorption of the blood � large increasing or causing pressure: Incisions, evacuation of the blood clot, ligature of the bleeding vessels, & closure of the cavity. � Infected hematoma: it is incised & drained (as an abscess and give B. spectrum antibiotics.

Vulval hematoma

III-Inflammatory conditions � Acute: acute vulvitis (result in diffuse swelling due to edema and congestion), acute Bartholinitis and Bartholin abscess (localized swelling in the lower 1/3 of the labia majora) � Chronic specific infections : e. g. tuberculosis, bilharziasis, condylomalata , viral (condyloma accuminata). These may give rise to localized masses.

Condyloma

IV-Vascular conditions: � Edema: due to general edema, PET or acute vulvitis. � Varicose veins: they are tortuous compressible non pulsating dark blue structures. It is associated with varicose veins of the legs � Elephantiasis: it is due to lymphatic obstruction. It can be caused by filariasis, lymphogranuloma inguinale, bilharziasis

Vulval edema

Vulval varicosities
 Bartholin cyst: it is the")
V -Non neoplastic cystic lesions of the vulva a) Bartholin cyst: it is the commonest cysts of the vulva � Types: ◦ Cyst of the duct ◦ Cyst of the gland � Clinical picture: ◦ A painless cystic swelling lying in the substance of the labia majora & is situated at the junction of the upper 2/3 & lower 1/3 of the labia majora. ◦ Dyspareunia. ◦ The vaginal introitus becomes S. shaped.

Bartholin gland cyst

Treatment of Bartholin cyst 1 -Marsupialization Advantages : �Permanent opening & drainage of the Bartholin gland. �Less bleeding, short operative time & good convalesce. 2 -Excision : of the cyst & the gland. It is rarely done due to Excessive bleeding, Time consuming, hematoma, tender scar, loss of the function, Incomplete removal, cellulitis. Indications : 1. Recurrent or persistent abscess or cyst. 2. Postmenopausal cyst: it may represent carcinoma; it is excised and examined microscopically.

marsupialization

Marsupialization
 Sebaceous cyst: Is a common, arises from obstruction of sebaceous glands. Such cysts")
B) Sebaceous cyst: Is a common, arises from obstruction of sebaceous glands. Such cysts are usually multiple and small and generally asymptomatic unless they become infected. They contain whitish cheesy material. Spontaneous rupture often occurs, or incision and drainage may be required. If infection is recurrent, the cyst can be excised with use of local anesthesia once the acute inflammation subsides.
Epidermoid (implantation dermoid) cyst: � It is due to implantation of sebum producing skin.")
C)Epidermoid (implantation dermoid) cyst: � It is due to implantation of sebum producing skin. Types: � Congenital (sequestration) dermoid: it is found in the middle line � Acquired: due to implantation of perineal skin at the time of obstetric operation e. g. episiotomy or following circumcision Clinical picture: � The cyst contains creamy yellow keratinous material secreted by the implanted sebum producing skin. � It is lined by stratified squamous epithelium. � Site: �In the perineum & posterior vaginal wall (following obstetric injuries) �At the clitoris: following circumcision Treatment: by excision
Paraurethral cyst (Cysts of the skene’s tubules): Cysts form when the openings of these")
D)Paraurethral cyst (Cysts of the skene’s tubules): Cysts form when the openings of these ducts are blocked due to previous infection. They are multiple, small, and adjunct to the external urethral meatus. The cysts can become infected causing paraurethral abscesses.
 Congenital cysts: Hymenal & clitoridal cyst � Cause: arise from remnants of")
E ) Congenital cysts: Hymenal & clitoridal cyst � Cause: arise from remnants of Wolfian (Gartner' s) duct. It is lined by cubical epithelium � Clinical picture: it becomes infected leading to recurrent abscesses or persistent sinuses � Treatment: excision & histopathology

Clitorial cyst

Gartner`s duct cyst
 : A -Connective tissue neoplasms: � Fibroma : the most common")
VI-(Benign neoplastic conditions) : A -Connective tissue neoplasms: � Fibroma : the most common benign solid vulvar tumors. It arises from the connective tissue of the labia majora �Types: it may be hard or soft. (if it undergoes mucoid degeneration) �Symptoms: usually symptomless � Malignant change into sarcoma may occur (very rare) �Treatment is by excision. � Lipoma: the second most common solid tumors found in the vulvar area, it may reach a big size �Characters: � Soft & lobulated � Fixed to the skin � May be sessile or pedunculated �Treatment: excision � Leiomyoma, neuroma, hemangioma &Iymphangioma

Vulval fibroma

B -Epithelial tumours: � Papilloma: true squamous papilloma which usually small single lesion formed of papillae of stratified squamous epithelium, covering a core of vascular c. t. It should be differentiated from condyloma acuminate and Bilharzial papilloma � Adenoma: it may arise from a‑ Bartholin gland : →a firm nodule at the site of the gland b‑ Skene's tubules c‑Wolffian duct origin � Tumour of sweat gland (Hidradenoma): It appears as a small nodules on the labia majora with red umbilicated top and it may ulcerate. So, it is mistaken for carcinoma Treatment: Any tumour should be treated by excision followed by histopathological examination to exclude malignancy.

Vulval papilloma

�C -Melanoma : careful examination to detect such nevi, Careful evaluation is important since vulvar melanomas tend to be diagnosed at amore advanced stage than melanomas located elsewhere.
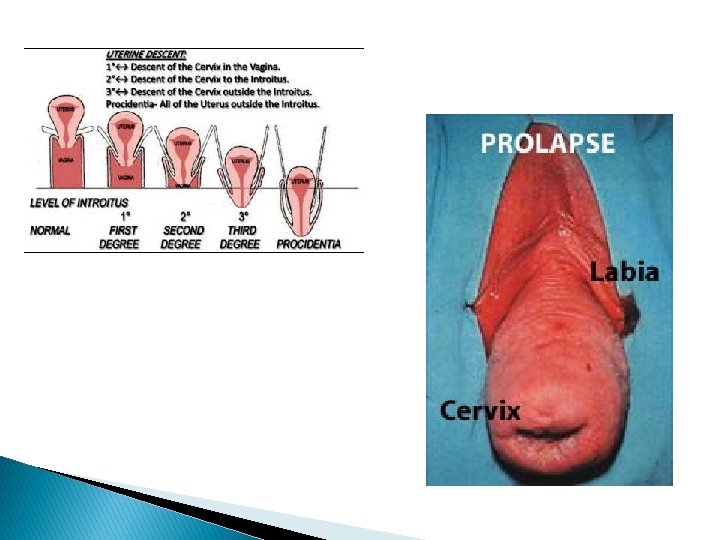
 Swellings presenting (appearing) at the vulva � � Vaginal : prolapse. Uterine :")
B) Swellings presenting (appearing) at the vulva � � Vaginal : prolapse. Uterine : prolapse (II° & III° uterine descend), chronic inversion III° and fibroid polyp. Cervical : grade II° uterine descent, congenital elongation of the cervix & cervical polyp. Round ligament condition. ◦ Hydrocele ofcanal of. Nuck. ◦ Endometriosis. � Conditions of urethra: a‑ Prolapse of urethra. b‑ Caruncle. � Ectopic : endometriotic deposits. � Endometrioma: it is a small nodule partially cystic & partially solid. It becomes tender, bluish & increase in size during menstrual flow Site: ‑At the site of an incision or injury due to implantation At the insertion of the round ligament due to vascular or Iymphatic spread Treatment: is by excision


Hydrocele of the canal of Nuck: � Processus vaginalis peritonei that fills with peritoneal fluid can give rise to a hydrocele located high in the labia majora. A concurrent inguinal hernia. � Occurs in 30% of cases.

II -Malignant swellings �Invasive squamous cell carcinoma ◦ 4% of female genital cancer. ◦ Naked eye appearance. �Ulcer, �Raised nodular �Fungating papillomatous ◦ Sites: �The clitoris �Labia majora. �Other less frequent malignant tumours of the vulva include � Malignant melanoma � Sarcomas � Leiomyosarcoma, � Rhabdosarcoma � Epithelioid sarcoma). � Blood borne metastatic lesions in the vulva is extremely rare e. g � Endodermal sinus tumours � Breast carcinoma.

Cancer vulva

� N. B. : Neoplasms of the Bartholin’s are exceptionally rare and are commonly malignant (columnar cell adenoma or carcinoma).
 Definition: Abnormal nourishment of cells, the term is applied")
Chronic vulval dystrophies (Vulval dermatoses) Definition: Abnormal nourishment of cells, the term is applied to lesions characterized by: 1. Hyperkeratosis = thickening of the horny layer. 2. Abnormal thickening or thinning of the epithelium. 3. Chronic inflammation in the subepithelial C. T. (dermis).

Vulval dystrophy
 A) Non- neoplastic")
Classifications: international society for the study of vulvar disease (ISSVD 1989) A) Non- neoplastic disorders The group now termed non-neoplastic epithelial disorders was formerly referred to as vulvar dystrophies; it was renamed under a classification scheme adopted in 1989 by the International Society for the. Study of Vulvar Disease. 1. Lichen sclerosus (hypoplastic dystrophy) 2. Squamous cell hyperplasia (formly hyperplastic dystrophy) 3. Other dermatoses: ◦ ◦ ◦ Seborrheic dermatitis Psoriasis Lichen planus Tinea cruris Behçet's syndrome
 Vulval intraepithelial neoplasia (VIN) (formly dystrophies with atypia): � Squamous (VIN ) ◦")
B) Vulval intraepithelial neoplasia (VIN) (formly dystrophies with atypia): � Squamous (VIN ) ◦ Mild dysplasia ◦ Moderate dysplasia ◦ Severe dysplasia + carcinoma in situ (CIS) � Non-Squamous ◦ Paget's disease ◦ Melanoma in situ (VIN)

Disorder Symptoms Vulvar signs Usual onset Lichen sclerosus Pruritus, burning, pain - Crinkled or parchment like appearance, -Hpopigmented-to-pink atrophic plaques - Resorption of labia minora and clitoral hood Post-menopause Squamous cell hyperplasia Pruritus - Thickened, whitish hyperkeratotic patches, - Excoriations, fissures Adulthood Biopsy findings - Hyperkeratosis, - Hyperkeratosis (thicker than with - Epidermal thinning, loss of rete ridges, lichen sclerosus), - Lengthening and distortion of rete - vacuolar degeneration, pegs, proliferation of cellular - Chronic upper dermal inflammation, elements, dermal inflammation - Homogenized dermis Treatment Potent topical corticosteroids; - Topical testosterone propionate; - Possibly systemic retinoids a. Without atypia topical corticosteroid 1% b. With atypia local destructive therapy

Prognosis of Non- neoplastic disorders: Hyperplastic dystrophy + atypia→ 5 -10% will develop carcinoma
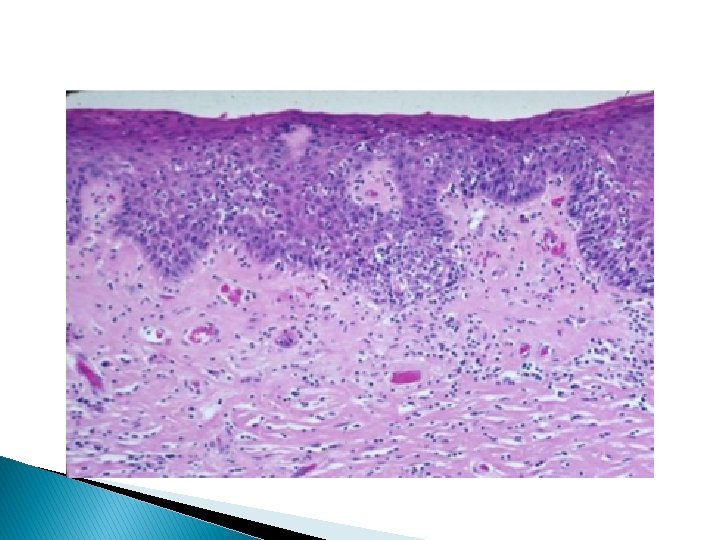
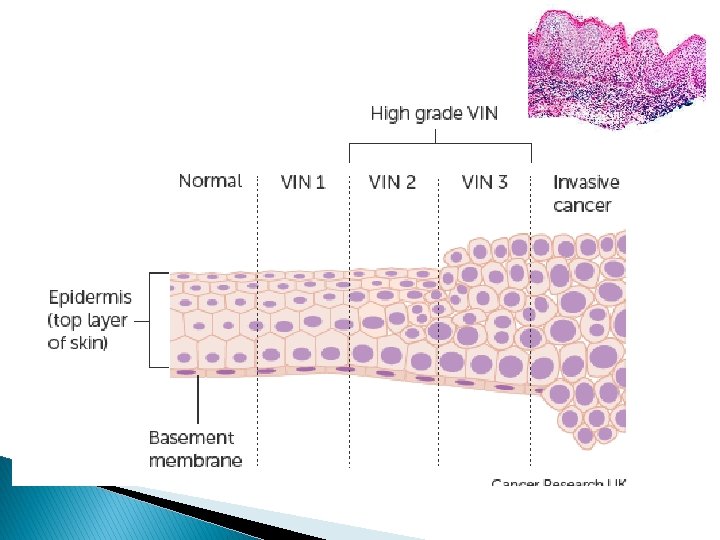
Vulval intraepithelial neoplasia(VIN) � Characterized by disordered maturation and nuclear abnormalities (as loss of")
B)Vulval intraepithelial neoplasia(VIN) � Characterized by disordered maturation and nuclear abnormalities (as loss of polarity, pleomorphism, large dark nuclei with increased mitotic figures which may be atypical and irregular nuclear membrane). � Grades: � VIN 1 abnormalities present in the lower third of the epithelium � VIN 2 abnormalities present in the inner 2/3 of the epithelium � VIN 3 abnormalities occupy the full thickness of the surface epithelium � No invasion of the basement membrane.

VIN Risk Factors: � Increased with advancing age, although recently occur in young women below 35 years � HPV infection � Smoking � Low soecieconomic state � Young age at first birth � squamous hyperplasia � High coffee consumption and vitamin A deficiency. � DM, hypertension

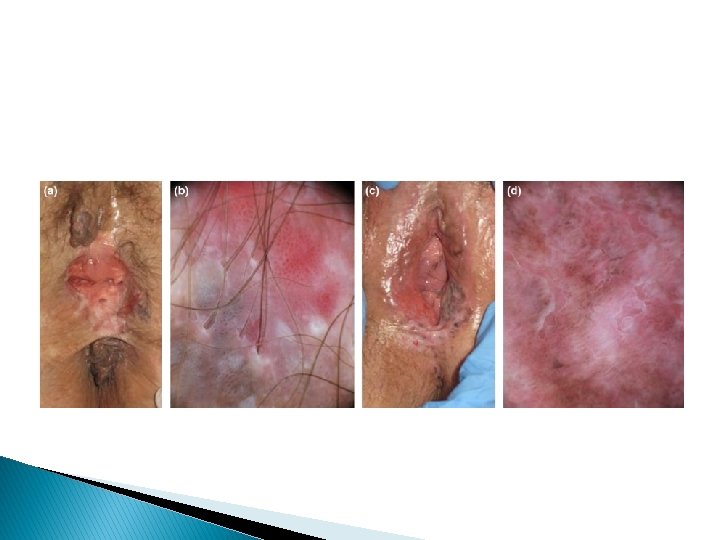
Clinical picture: � Pruritus vulva lasting for more than 6 months or not responding to treatment must be biopsed. � Condyloma should be biopsed to determine whether underlying neoplasm is also present � Lesion may be white, velvety, erythematous, ulcerated or pigmented.
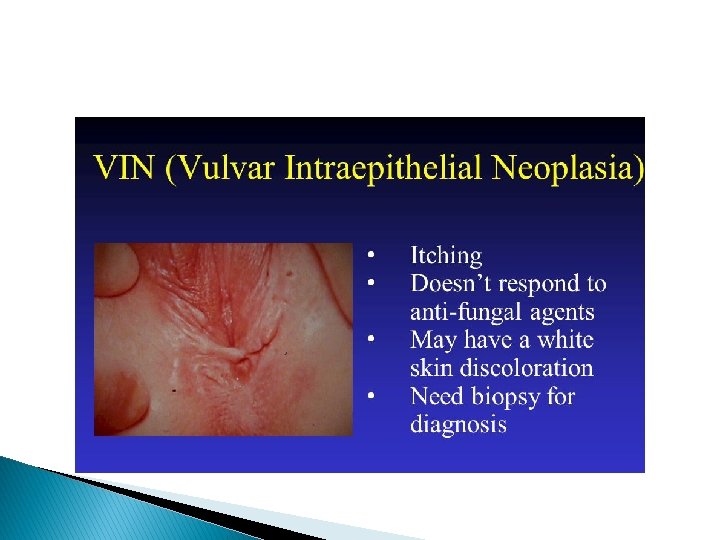

Diagnosis of VIN: � Careful inspection, Colposcopic examination with 5 % acetic acid (cells become white) � Biopsy or toludine blue may aid in the localizing the site for biopsy.
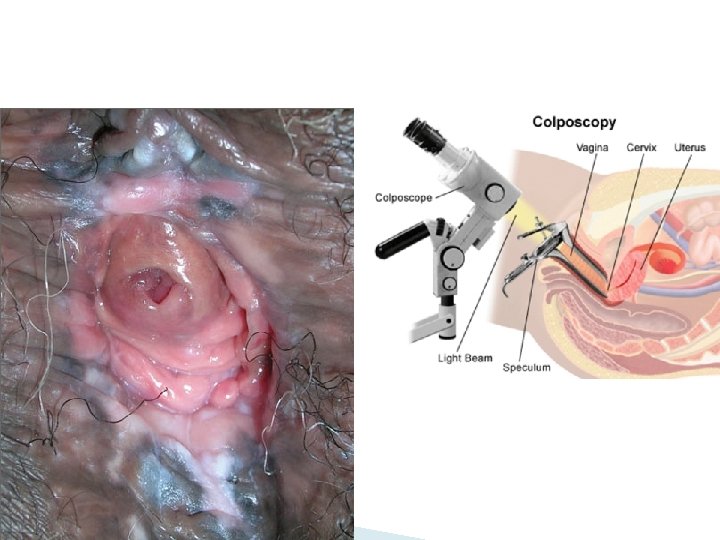

Cervix should also be evaluated by colposcope because the lesion is usually multifocal. � Treatment of VIN: � Wide local excision: � ◦ In cases with CARCINOMA IN SITU ◦ In patients above 40 years � If only VIN present it cures 75% of cases (disadvantage: disfigurement of vulva). � Laser evaporation: ◦ Young patient ◦ Recurrence 10 -20% associated highly with smoking

Invasive cancer of the vulva � Vulva contains a variety of tissues and hence all types of tumours can occur in the vulva. Many types have been recorded, both benign and malignant. � Vulval malignancies account for about 4% 5% of all genital malignancies. � Varieties: include

Squamous cell carcinoma Basal cell carcinoma Malignant melanoma Bartholin gland carcinomas Metastatic Verrucous carcinoma Sarcoma 92% 2 -3% 2 -4% 1% 1% <1% 1%

Squamous cell carcinoma of vulva � Vulvar squamous cell carcinomas begin as small areas of epithelial thickening that resemble leukoplakia but, in the course of time, progress to create firm, indurated, exophytic tumours or ulcerated, endophytic lesions. � Incidence: ◦ Occur mainly in P. M. women ◦ The mean age at diagnosis is 65 years ◦ More frequent in obese, hypertensive, diabetic patients with atherosclerosis

Etiology& pathogenesis � 1 - age : 60 to 70 years � 2 - HPV : TYPE 16, 18 � 3 -VIN AND CIS � 4 -SQUAMOUS CELL HYPERPLASIA � 5 - SMOOKING � 6 - HERPES SIMPLEX TYPE 2 � 7 - HIV infection and immunodeficiency syndromes � 8 - Lymphogranuloma venereum and granuloma inguinale

Clinical picture 1. The clinical manifestations are pain, local discomfort, itching, and exudation because superficial secondary infection is common. 2. Vulval lump 3. Vulval lesion which may be raised, ulcerated, pigmented, or warty in appearance 4. Other symptoms are bleeding, discharge or dysuria 5. Many are misinterpreted as dermatitis, eczema, or leukoplakia for long periods N. B. Most lesions occur on the labia majora and less commonly the labia minora. The clitoris and perineum are less common sites

� Diagnosis: ◦ Careful inspection of the vulva especially in those cases with long standing pruritus ◦ Assessment of groin lymph nodes ◦ Pelvic examination ◦ Colposcopic examination of the cervix and vagina to exclude associated intraepithelial neoplasia of the lower genital tract ◦ Biopsy and histopathological examination is the definitive diagnosis

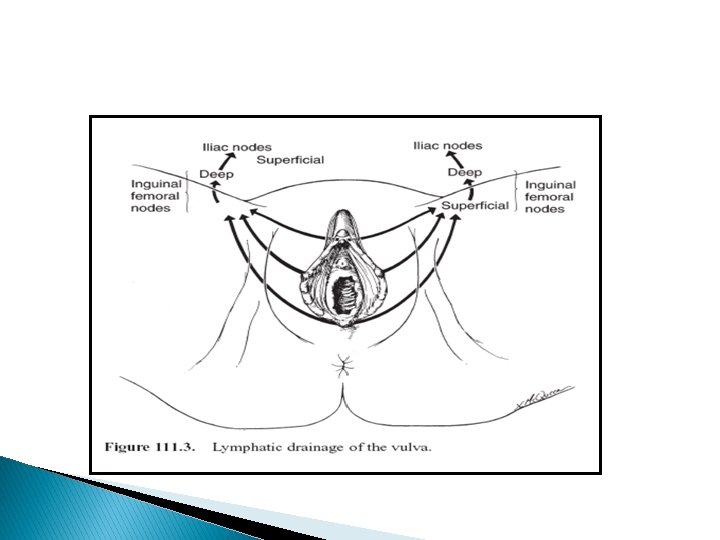
Spread � Risk of metastatic spread is linked to the size of tumour, depth of invasion, and involvement of lymphatic vessels. The inguinal , femoral , pelvic, iliac, and periaortic lymph nodes are most commonly involved. Ultimately, lymphohematogenous dissemination involves the lungs, liver, and other internal organs. � Direct: to adjacent structures as vagina, urethra, and anus. Kissing ulcer may result from extension to the other side � Lymphatic: ◦ Common pathway: to superficial inguinal glandsdeep inguinal glanddeep femoral gland (along lymph node of cloquet or Rosenmuller gland found in femoral canal) external iliac glandcommon iliac glandaortic gland. � N. B: crossing between two sides along mons veneris � Blood: liver - lungs. . . etc ◦ Uncommon pathway: bypassing the superficial inguinal glandsinternal pudendal vesselsinternal iliac group
 Stage I Tumour confined to the")
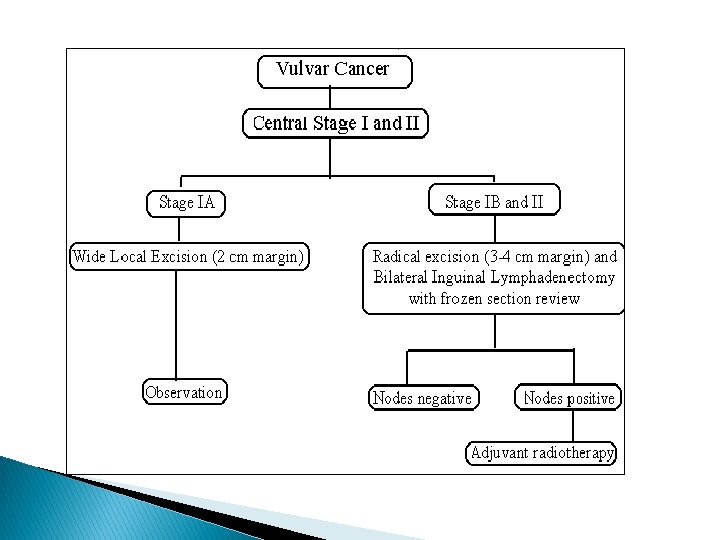
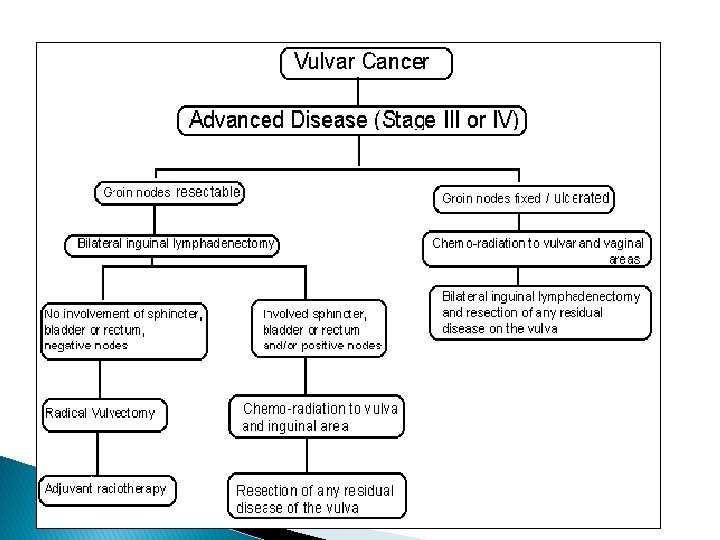
Stage 0 Carcinoma in-situ, intraepithelial carcinoma (VIN III) Stage I Tumour confined to the vulva and/or perineum - 2 cm or less in greatest dimension, nodes are not palpable. stage II Tumour confined to the vulva and/or perineum - more than 2 cm in greatest dimension, nodes are not palpable. stage III Tumour of any size with: Adjacent spread to the lower urethra and/or the vagina, or the anus, and/or Unilateral regional lymph node metastasis Stage IV IVA: Tumour invades any of the following: Upper urethra, bladder mucosa, rectal mucosa, pelvic bone and/or bilateral regional node metastasis. IVB: Any distant metastasis including pelvic lymph nodes.

Treatment of carcinoma of the vulva: � Stage I, II, and early stage III: radical vulvectomy and bilateral inguinal femoral node dissection. This operation � removed the entire vulva, including the clitoris, subcutaneous tissue, and inguinal femoral nodes. (Butterfly incision ). This is rarely done nowadays The deep pelvic nodes are rarely removed unless the inguinal nodes are involved. Most gynecologists now remove only the inguinal and femoral nodes at the time of operation and treat the deep pelvic nodes with external radiation if superficial nodes are involved with tumor. � Recently, modifications have been introduced to decrease the incidence of wound breakdown. These modifications include: �

◦ Performing the inguinal femoral node dissection through separate inguinal incisions, then completing the radical vulvectomy. ◦ Inpatients with stage I A lesions invading to a depth of less than 1 mm , wide local excisionwith 2 Cm safety margin and observation only. �
:")
� Advanced disease (stage III &IV):

� Complications the vulva: of surgery of carcinoma of ◦ Wound breakdown + infection (decrease in three incision techniques) ◦ Thromboembolism ◦ Secondary hemorrhage ◦ Chronic leg edema ◦ Parathesia over the upper legs ◦ Impaired sexual function

Prognosis: ◦ Patients with lesions less than 2 cm in diameter have a 60% to 80% 5 -year survival rate after treatment with one-stage vulvectomy and lymphadenectomy ◦ Larger lesions with lymph node involvement yield a less than 10% 5 -year survival rate.

Bartholin gland cyst

marsupialization

Clitorial cyst

Gartner`s duct cyst

Vulval hematoma

Vulval edema

Vulval varicosities

Vulval fibroma

Vulval papilloma

Condyloma

Vulval dystrophy

Cancer vulva

Thank You
- Slides: 82