PRECANCEROUS CONDITIONS OF THE ORAL CAVITY o By

PRECANCEROUS CONDITIONS OF THE ORAL CAVITY o By Arun Babu Joseph
 Lesions considered having a definite risk of malignancy o o o")
Classification ( Bailey) Lesions considered having a definite risk of malignancy o o o Leukoplakia Erythroplakia Chronic hyperplastic candidiasis Conditions that are not themselves premalignant but which are associated with a higher than normal incidence of oral cancer o o o Oral submucous fibrosis Syphilitic glossitis Sideropenic dysphagia Oral conditions about which there is still some doubt as to whether their association with oral cancer is causal or casual o o o Oral Lichen planus Discoid lupus erythematosus Dyskeratosis congenita

Types of oral precancer. Precancerous lesions o Defined as morphologically altered tissue in which cancer is more likely to occur than its apparently normal counterpart. Example o Leukoplakia o Erythroplakia o Mucosal changes associated with smoking habits. o Carcinoma in situ o Bowen disease o Actinic keratosis, cheilitis and elastosis.

Precancerous conditions o Defined as generalized state or condition associated with significantly increased risk for cancer development. Example o Oral sub mucous fibrosis o Syphilis o Sideropenic dysphagia o Oral Lichen planus o Lupus erythematosus


Leukoplakia o o Any white patch or plaque that cannot be characterized clinically or pathologically as any other disease. This definition has no histological connotation.
 Homogenous : lesions that are uniformly white. Non homogenous")
Forms of leukoplakia. (WHO 1980) Homogenous : lesions that are uniformly white. Non homogenous : lesions in which part of the lesion is white and the rest appears reddened. Alternatively 1. ) Homogenous a. ) Smooth b. )Furrowed(fissured) c. ) Ulcerated. 2. ) Non homogenous nodulospeckled: Well demarcated raised white areas interspersed with reddened areas.

According to risk of future development of oral cancer. High risk sites n n n Floor of mouth Lateral or ventral surface of tongue. Soft palate. Low risk sites n n Dorsum of tongue Hard palate Intermediate group n All other sites of oral mucosa.

Etiology Local factors o Tobacco Smokeless and smoking tobacco. o Alcohol o Chronic irritation malocclusion ill fitting dentures, sharp broken teeth, hot spicy food, root piece etc o Candidiasis o Electromagnetic reaction or galvanism
 Regional & systemic factors. o o o o Vitamin deficiency Sideropenic")
Etiology (contd. ) Regional & systemic factors. o o o o Vitamin deficiency Sideropenic anaemia Nutritional deficiency Conditions causing xerostomia ( Salivary gland diseases, Anticholinergic drugs, Radiation. ) Drugs ( Anticholinergics, Antimetabolic, Systemically administered alcohol) Virus ( HSV & HPV) Idiopathic

Histopathological features. Hallmark o Surface hyperkeratosis o Epithelial hyperplasia o Epithelial dysplasia

Keratinization pattern Keratinization of the mucosal epithelium which is normally non-keratinized. Hyperorthokeratosis o Orthokeratosis: In normal state , superficial epithelium, is nearly homogenous, eosinophilic and anuclear with stratum granulosum always present. o Hyperorthokeratosis: abnormal increase in thickness of the orthokeratin layer of stratum corneum in a particular location. Hyperparakeratosis o Parakeratosis: superficial epithelium is flat and acidophilic with pyknotic nuclei. Stratum granulosum may or may not be present. o Hyperparakeratosis: Increased thickness of parakeratotic layer, exceeding the normal thickness.

Epithelium Epithelial thickness v Hyperplasia v Atrophy v Vacuolar degeneration v Acanthosis v Basal cell hyperplasia v Intra-epithelial edema

Epithelial dysplasia § § § § § Drop shaped rete ridges Nuclear hyperchromatism Nuclear pleomorphism Altered nuclearcytoplasmic ratio Excess mitotic activity Loss of polarity of cells Deep cell keratinisation Loss of differentiation Loss of intercellular distance

o o o Epithelial dysplasia seen in 3% of snuff induced leukoplakias and 16% of smoking habit related leukoplakia. Nodular leukoplakia shows higher frequency of epithelial dysplasia Grading

Connective tissue o o o Chronic inflammatory cell infiltration is seen in 50% cases. Submucosal, homogenous eosinophilic material is usually seen in the connective tissue. Hyaline degeneration seen in 10 % cases
 than")
Malignant potential o o 0. 3% - 10% cases Higher in women (6%) than men (3. 9%) due to involvement of endogenous factors Leukoplakia associated with chewing habit of tobacco shows higher rate of malignant transformation. Nodular dysplasia has higher risk of malignant transformation than other clinical types.

o o o High risk if Elderly patient Persistence of lesion for several years Female patient Lesion situated on the margins, base of tongue, floor of mouth Erosive lesions

Differential diagnosis v v v Lichen planus Chemical burns Syphilitic mucus patches White sponge nevus Discoid lupus erythematosus Psoriasis
 v v v Leukoedema Hairy leukoplakia Verruca vulgaris Cheek biting")
Differential diagnosis (contd. ) v v v Leukoedema Hairy leukoplakia Verruca vulgaris Cheek biting lesion Electrogalvanic white lesion

Management Ø Ø q o o Elimination of the etiological factor Conservative treatment 13 cis retinoic acid Antioxidant therapy Nystatin therapy

Ø Surgical management n n Ø Biopsy taken for microscopic examination areas with greater surface irregularities. Conventional Surgery Cryosurgery Electrocautery LASER from

Guidelines for treatment o o Biopsy should be done Elimination of etiological factors Conservative /Surgical management if not heal in 2 -3 weeks Conservative treatment applied to large incipient lesions & verrucous lesions

o o Surgical treatment if conservative treatment fails in 3 months Excision of nodular leukoplakia & follow up All patients , re-examination twice a year Re-biopsy after 5 -6 months

ERYTHROPLAKIA q o Also called erythroplasia of Queyrat. Def: Area of reddened, velvety textured mucosa that cannot be identified on the basis of clinical & histopathologic examination as being caused by inflammation or any other disease process.

Etiology o o Idiopathic Alcohol Smoking Secondary infection or superinfection with candidiasis

Clinical features Ø Ø Seen as a non elevated red macule on an epithelial surface. Otherwise asymtomatic. Age and sex Male predilection 6 th & 7 th decade Sites § § § All mucosal surfaces of head & neck area 50% found on vermilion or intraoral surfaces rest evenly divide between larynx & pharynx Intraorally lateral & ventral tongue, oral floor & soft palate are more frequently involved.

Hisopathological features Ø Ø Ø Epithelial dysplasia Cause for the red colour Spinous layer contains cells showing atypia, hyperchromatism, pleomorphism, & increase in the number of mitotic figures.

Differential diagnosis. o o o o Candidiasis Denture stomatitis Tuberculosis Histoplasmosis Area of mechanical irritation Macular hemangioma Telengiectasia. Traumatic lesion

Management o o o 1 % toluidine blue test. Incisional biopsy for microscopic diagnosis. Conservative surgical procedure such as mucosal stripping Destructive techniques such as electrocoagulation, cryotherapy, laser ablation also effective. Extended clinical follow up. Elimination of a suspect irritant

PIPE SMOKERS’ KERATOSIS o q palatal keratosis due to pipe smoking is benign. Any carcinomas related to pipesmoking appears in another site in the mouth and may not be preceded by keratosis.

SMOKELESS TOBACCO-RELATED KERATOSES o o o Hyperkeratotic mucosal lesions Management Diagnosis is based on the history of snuff use and the white lesion in the area where the tobacco is held. Biopsy is required Snuff-dippers’ lesions will resolve on stopping the habit Regular follow-up

Bowens disease Localized intraepidermoid carcinoma o Characterized by progressive scaly or crusted plaque like lesion Causes o Sun exposure o Arsenic ingestion o

Clinical features o o o Sites : male and female genital mucosa and in oral mucosa as erythroplakia, leukoplakia or eryhematous lesion. Skin: red & slightly scaly area on the skin, which eventually enlarges and turns into white or yellowish lesion. Signs: when scales are removed a granular surface without bleeding is seen.

Ø o Histopathology Intraepithelial features of malignancy Management Freezing technique/diathermy/ cauterization/ radiotherapy/ application of cytotoxic drugs.

Chronic hyperplasic candidiasis. o o Dense chalky plaques of keratin Plaques thicker & more opaque than leukoplakia Commonly seen at the oral commisures, extending into adjacent skin & face. High degree of malignant change

o o o Treatment nystatin, amphotercin, or miconazole to eliminate the infection Treatment necessary for many months & reinfection common Surgical excision for persistent lesions.

Oral Lichen planus o o o First described by Erasmus Wilson in 1869 Inflammatory condition of skin presenting with characteristic violaceous , polygonal, pruritic papules. Lace like pattern. Buccal mucosa ( 84%) lips, tongue, gingiva, floor of mouth & palate.

Etiology Ø Ø Immunology Cell mediated immune response Autoimmunity Immunodeficiency Genetic factors Infections Drugs & chemicals

Ø Ø Ø Psychogenic factors Habit Miscellaneous Deficiency of vitamin B 1, B 6, & C, electric potential difference, anaemia, & patients with secondary syphilis. Trauma & malnutrition

Clinical features o o o Burning pain of the oral mucosa Appearance Oral lesion characterized by white & gray velvety thread like papules in a linear angular or retiform arrangement forming typical lacy reticular patterns, rings and streaks over the oral mucosa. Wickham’s striae--- tiny white elevated dots present at the intersection of white lines.

Types of oral lichen planus o o o o Reticular type Papular Plaque Atrophic form Bullous form Hypertrophic form Annular form

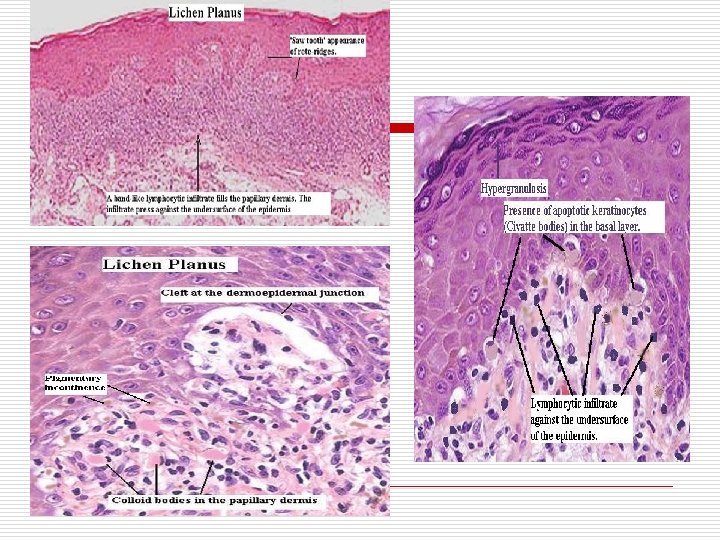
Histopathological features of oral lichen planus o o o Hyperkeratosis Prominent granular layer Basal cell degeneration (may form colloid bodies) Heavy lymphocyte infiltration (T cells) in the upper epidermis Saw tooth dermoepidermal junction.

Differential diagnosis o o o o o Leukoplakia Candidiasis Pemphigus Lupus erythematosus Drug induced lesion White sponge nevus Ectopic geographic tongue Cheek biting Lichenoid drug reaction
 Association between")
Malignant potential o o 1. 2 % malignant change (Silverman et al) Association between LP & oral cancer seen only with atrophic or erosive LP.

Management o o Removal of cause Medical therapy Steroids In most patients with erosive & ulcerative lesion topical steroids are commonly used. If severe, systemic steroids are used. Topical Antifungal agents. Vitamin A analogues Cyclosporine

Surgical therapy. Indications o When the conventional methods fail in ulcerative lesions o In case of small solitary lesions Cryosurgery & cauterization have also been tried. o

Others o o Psychotherapy Dapsone therapy PUVA therapy Symptomatic

Treatment options o o o o Group 1 lichen planus of reticular or atrophic variety without symptoms. No treatment is required Regular follow up Diazepam for anxiety Group 2 lichen planus of reticular or atrophic variety with mild to moderate pain and burning Local application of benzocaine 10 % for burning 2 mg Diazepam Topical corticosteroid Intralesional steroid for quicker relief. Regular follow up.
 Group 3 Erosive lichen planus o o Immediate biopsy Local")
Treatment options (Contd. ) Group 3 Erosive lichen planus o o Immediate biopsy Local control of pain Intralesional steroid If infected, antibiotics. Group 4 lichenoid reaction o o Discontinue offending drug Local application of benzocaine

Oral submucous fibrosis o o Ø Insidious chronic disease affecting any part of the oral cavity and sometimes the pharynx Very common in the Indian subcontinent Juxta epithelial inflammatory reaction fibroelastic changes of lamina propria + epithelial atrophy stiffness of oral mucosa & trismus

Etiopathogenesis o o o Chillies Tobacco Betel nut Nutritional deficiency Defective iron metabolism
 o o o Bacterial infections Collagen disorders Immunological disorders Genetic susceptibility")
Etiopathogenesis (Contd. ) o o o Bacterial infections Collagen disorders Immunological disorders Genetic susceptibility Altered salivary composition

Clinical features Age & sex o o Affects both sexes Majority between 20 -40 years. Site distribution o o Most frequent location buccal mucosa & retromolar areas. Also commonly involves soft palate, palatal fauces, uvula, tongue & labial mucosa.

Symptoms Onset is insidious Early symptoms Burning sensation of oral mucosa, aggravated by spicy food Vessiculation, ulceration, pigmentation, recurrent stomatitis and defective gustatory sensation may also be present Late symptoms Gradual stiffening of the oral mucosa Trismus Dysphagia Referred pain in the ears and deafness nasal voice

Signs o o Earliest sign is blanching of the mucosa Becomes slightly opaque and white Mucosa acquires a marble like appearance. Later mucosa becomes stiff and vertical fibrous bands appear.

Clinical stages of oral submucus fibrosis o o o Stage of stomatitis and vesiculation. Stage of fibrosis Stage of sequelae & complications.

Histopathological features. o o o Epithelium Most cases oral epithelium is markedly atrophic. The atrophic epithelium exhibits intercellular edema (18 %), signet cells( 13%), and epithelial atypia (7%). Sometimes atrophic epithelium is associated with hyper-orthokeratosis Liquefaction degeneration of the basal cell layer. Rete pegs are completely lost

o o o Connective tissue. It shows vesicles which are caused by sub epithelial accumulation of fluid. Inflammatiory cells are mostly mononuclear: eosinophils & occasionally plasma cells maybe seen. Pindborg has described the connective tissue changes in 4 consecutive stages 1. ) Very early stage 2. ) Early stage 3. ) Moderately advanced stage 4. ) Advanced stage

Diffuse hyalinization of subepithelial stroma with few, small fibroblastic nuclei and with pigment incontinence from the overlying epithelial melanin .

Epithelial atypia in OSMF o o Irregular epithelial stratification, increased number of mitotic features, nuclear pleomorphism, hyperchromatism and loss of polarity of cell. Spongiosis especially in the basal cell layer. Signet cells seen in the basal layer. Marked reduction in melanin pigmentation in basal cell layer.

Malignant potential o o From diverse intra oral locations Atrophic epithelium Hyperkeratotic Intracellular edema + Basal cell hyperplasia Epithelial atypia + hyperplasia Carcinoma

Management o o Reduction of habit / behavioral therapy Medical therapy n n Vitamin rich diet along with iron therapy Dexamethasone 4 mg (1 ml) combined with hylase, 1500 I. U. in 1 ml is injected into the affected area biweekly for 8 -10 weeks. Vitamin E may also be used with the above combination. Placental extract

Surgical treatment o o Aim is to relieve trismus, prevent further fibrosis & to provide neo vascularization of fibrous tissue. Indications v Marked limitation of opening of mouth. v Biopsy reveals neoplastic changes v Marked dysphagia

Surgical options o o o Excision of fibrous bands followed by use of tongue flaps as a graft Excision of fibrotic bands, followed by reconstruction using bilateral full thickness nasolabial flap New technique is of bilateral palatal flap to cover the exposed area, in combination with bilateral temporalis myotomy & coronoidectomy

Laser o o o Carbon dioxide laser surgery alleviates the functional restriction. Under GA laser is used to incise the buccal mucosa and vaporize the submucosal connective tissue to the level of buccinator muscle. Hemostasis is provided by lased surface itself and the mouth opening increases immediately.

o Oral physiotherapy o o Oral exercises are advised in early and moderately advanced cases. Includes mouth opening and ballooning of the mouth. Cryosurgery Diathermy

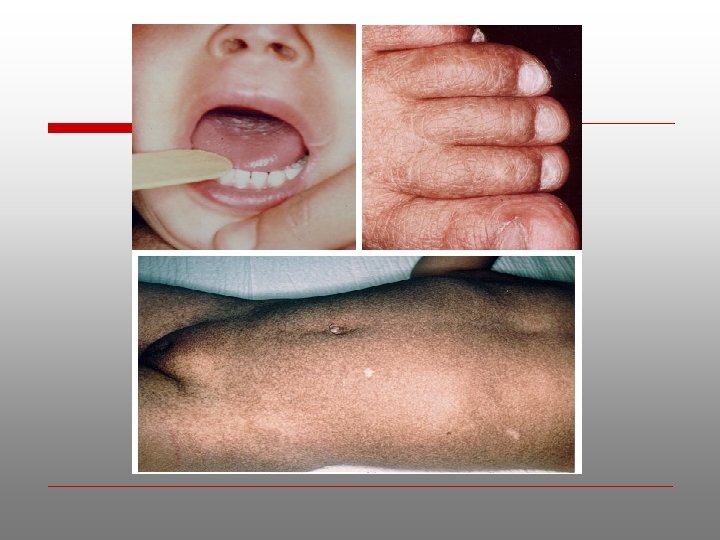
Dyskeratosis Congenita o o Zinssner-Engman-Cole syndrome. Rare genokeratosis Characterized by 3 typical signs oral leukoplakia, dystrophic nails and pigmentation of skin. Other features frail skeleton, mental retardation, small sella turcica , dysphagia, transparent tympanic membrane, deafness, epiphora, eyelid infection, urethral anomalies, small testes and hyperhidrosis of the palms and soles

Oral manifestations o o o 5 and 15 years Diffusely distributed vesicles and ulcerations followed by accumulation of white patches of necrotic epithelium and sometimes superimposed monilial infection over tongue & buccal mucosa 14 -20 years recurrent ulceration and development of erythroplasia or red mucosal lesion. 20 -30 years development of erosive leukoplakia and carcinoma.

Histology o Skin lesion shows increased number of melanin containing chromatophores and increased vascularity. o Depending on stage of disease epithelium may show dysplasia. Laboratory finding o Pancytopenia Radiographic feature o There maybe severe periodontal bone loss Management o No specific treatment. o Periodic check up.

Discoid Lupus Erythematosus o o o Oral lesions consists of circumscribed, somewhat elevated white patches usually surrounded by a telengiectatic halo. Epithelial dysplasia maybe seen on histological examination, this may lead onto malignant transformation. Malignant change usually occurs in those lesions adjacent to vermilion border. More often in men than women Such patients advised to avoid bright sunlight and when in open air to apply an ultraviolet barrier cream to the lips.
 o o In 1936, Ahlbom")
Sideropenic dysphagia ( Plummer-vinson syndrome, Paterson- Kelly syndrome. ) o o In 1936, Ahlbom showed the relationship between sideropenic dysphagia and oral cancer. Particularly common in Swedish women. Sideropenic dysphagia leads to epithelial atrophy which is excessively vulnerable to carcinogenic agents. Anaemia responds to iron supplements. But it is not known whether such treatment reduces risk of subsequent malignant change.

Syphilitic glossitis. o o o Prior to antibiotic era Atrophy of overlying epithelium. Atrophic epithelium more vulneralble to irritants Squamous cell carcinoma can develop in syphilitic glossitis even in the absence of oral leukoplakia. Active syphilis must be treated. Regular follow up is required.

Just remember this…… ü ü ü Common precancerous conditions are Leukoplakia, erythroplakia, Submucous fibrosis & Oral Lichen Planus High chance of malignancy seen in speckled leukoplakia, dysplastic leukoplakia, erythroplakia, submucous fibrosis etc. Etiology of most of the lesions are chemical irritants such as tobacco, betel etc.

Just remember this…. . ü Management includes : Ø Ø Ø Stop any associated habits e. g. betel quid or smoking Treat candidal infection and/or iron deficiency. Biopsy to assess dysplasia Assess risk of premalignant change on clinical & histological findings Consider ablation of individual lesions Regular follow up

- Slides: 80