Gouty Arthritis Dr noori rheumatologist Gout Definitions Gout







 reabsorbed in")








































































- Slides: 86
Gouty Arthritis Dr. noori rheumatologist
Gout: Definitions Gout is a disease characterized by hyperuricemia and monosodium urate deposition in the body Gouty arthritis is joint inflammation caused by monosodium urate crystals in the synovial fluid and/or joint tissues
Gout is a metabolic disease that most often affects middle -aged to elderly men and postmenopausal women. It results from an increased body pool of urate with hyperuricemia. It typically is characterized by episodic acute and chronic arthritis caused by deposition of MSU crystals in joints and connective tissue tophi and the risk for deposition in kidney interstitium or uric acid nephrolithiasisn.
Women represent only 5– 20% of all patients with gout. Premenopausal gout is rare; it is seen mostly in individuals with a strong family history of gout. Kindreds of precocious gout in young females caused by decreased renal urate clearance and renal insufficiency have been described. Most women with gouty arthritis are postmenopausal and elderly, have osteoarthritis and arterial hypertension that cause mild renal insufficiency, and usually are receiving diuretics.
URATE, HYPERURICEMIA & GOUT Urate: end product of purine metabolism Hyperuricemia: serum urate > urate solubility (> 6. 8 mg/dl): urate>7 men/urate>6 women Gout: deposition of monosodium urate crystals in tissues
HYPERURICEMIA & GOUT Hyperuricemia caused by Overproduction Underexcretion No Gout w/o crystal deposition
Gout: Pathophysiology Uric acid: overproduction vs. underexcretion Mechanisms of urate “production” cellular nucleoproteins/nucleotides (~ 66%) diet (~33%) Mechanisms of urate excretion kidney (~66%) gut (~33%)
Renal Excretion of Uric Acid Completely filtered by the glomerulus Completely (essentially) reabsorbed in the proximal tubule Approximately 50% is secreted back into the tubule in the descending loop Approximately 80% (of the 50% now in the loop) is reabsorbed in the ascending loop
Gout: Clinical Manifestations Acute gouty arthritis Intercritical gout Chronic tophaceous gout Miscellaneous other (e. g. , gouty nephropathy)
Stages of Classic Gout Asymptomatic hyperuricemia Very common biochemical abnormality Defined as 2 SD above mean value Majority of people with hyperuricemia never develop symptoms of uric acid excess Acute Intermittent Gout (Gouty Arthritis) Episodes of acute attacks. Symptoms may be confined to a single joint or patient may have systemic symptoms. Intercritical Gout Symptom free period interval between attacks. May have hyperuricemia and MSU crystals in synovial fluid Chronic Tophaceous Gout Results from established disease and refers to stage of deposition of urate, inflammatory cells and foreign body giant cells in the tissues. Deposits may be in tendons or ligaments. Usually develops after 10 or more years of acute intermittent gout.
Asymptomatic Hyperuricemia alone does NOT make a diagnosis of gout -only a subset of people with hyperuricemia will develop gout -probability of gout increases with higher uric acid levels Asymptomatic hyperuricemia generally requires no treatment
ASYMPTOMATIC A- meaning without indicates that there are no symptoms associated Patient will be unaware of what is happening Gout can only be determined with the help of a physician
Management of Asymptomatic Hyperuricemia Determine the cause Address contributing factors Hypertension Obesity Alcoholism Hyperlipidemia At this time, specific urate-lowering drugs are not indicated
Clinical Course of Classic Gout
Presenting Symptoms Systemic: fever rare but patients may have fever, chills and malaise Musculoskeletal: Acute onset of monoarticular joint pain. First MTP most common. Usually affected in 90% of patients with gout. Other joints knees, foot and ankles. Less common in upper extremities Postulated that decreased solubility of MSU at lower temperatures of peripheral structures such as toe and ear Skin: warmth, erythema and tenseness of skin overlying joint. May have pruritus and desquamation GU: Renal colic with renal calculi formation in patients with hyperuricemia
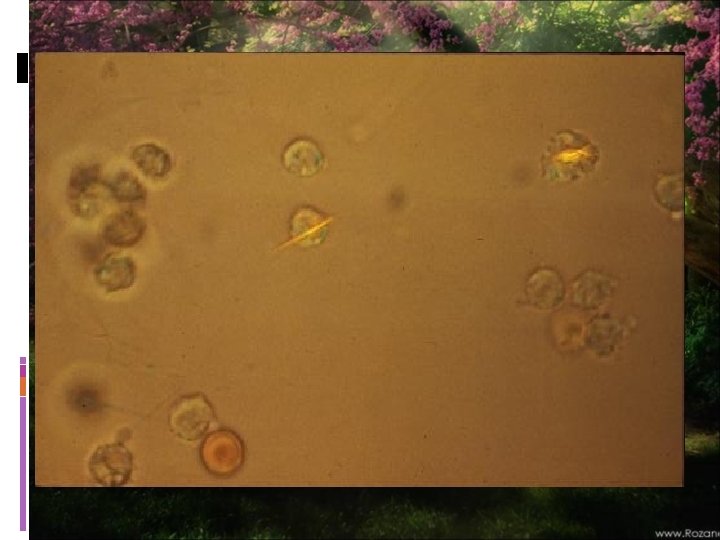
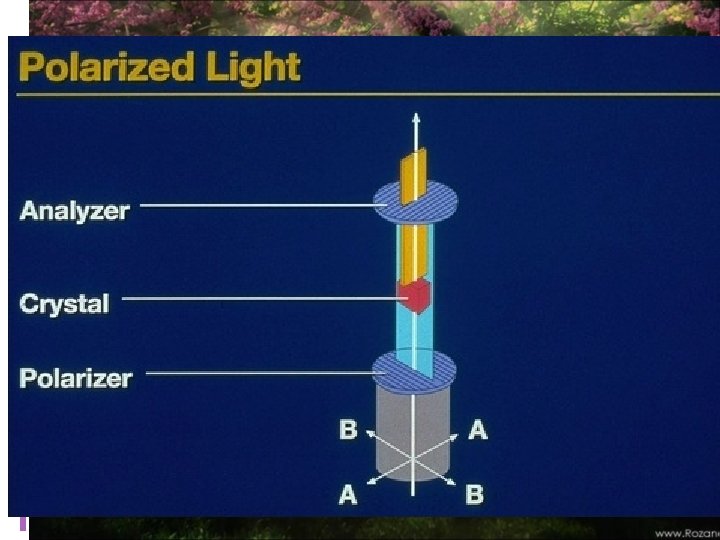
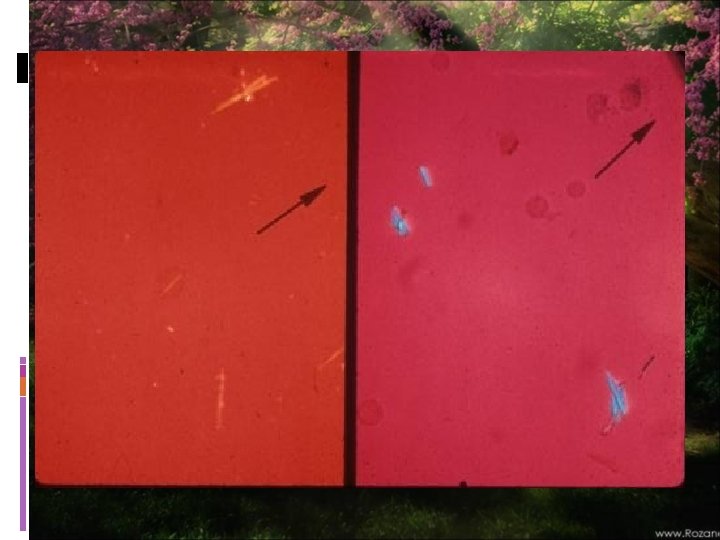
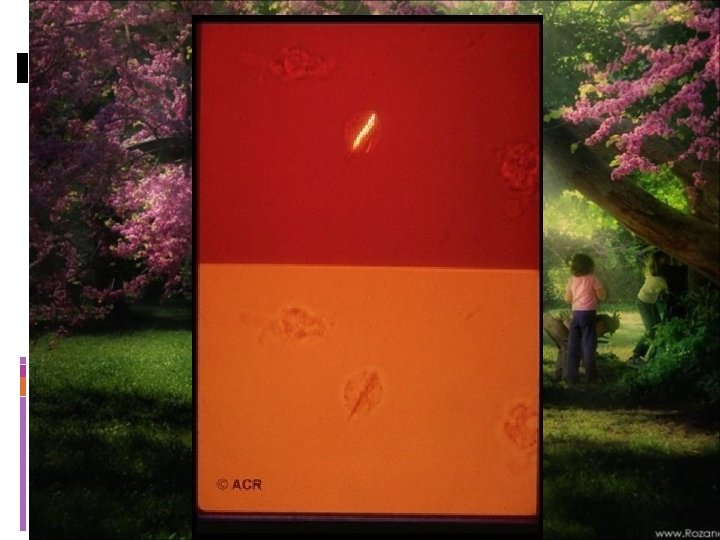
Acute Gouty Arthritis: Diagnosis Observation of monosodium urate crystals in synovial fluid leukocytes Monosodium urate crystals are needle-shaped negatively birefringent
ACUTE gout Sever and sudden onset Involve one or a few joints Frequently starts nocturnally Joint is warm, red, and tender
Laboratory Diagnosis diagnosis ideally should be confirmed by needle aspiration of acutely or chronically involved joints or tophaceous deposits. Acute septic arthritis, several of the other crystalline-associated arthropathies, palindromic rheumatism, and psoriatic arthritis may present with similar clinical features. During acute gouty attacks, needle-shaped MSU crystals typically are seen both intracellularly and extracellularly. With compensated polarized light these crystals are brightly birefringent with negative elongation.
Synovial fluid leukocyte counts are elevated from 2000 to 60, 000/ L. Effusions appear cloudy due to the increased numbers of leukocytes. Large amounts of crystals occasionally produce a thick pasty or chalky joint fluid. Bacterial infection can coexist with urate crystals in synovial fluid; if there is any suspicion of septic arthritis, joint fluid must be cultured
SYMPTOMS Joint pain Affects one or more joints : hip, knee, ankle, foot, shoulder, elbow, wrist, hand, or other joints Great toe, ankle and knee are most common Swelling of Joint Stiffness Warm and red Possible fever Skin lump which may drain chalky material
Synovial Fluid Findings Needle shaped crystals of monosodium urate monohydrate that have been engulfed by neutrophils
Diagnosis Definitive diagnosis only possible by aspirating and inspecting synovial fluid or tophaceous material and demonstrating MSU crystals Polarized microscopy, the crystals appear as bright birefringent crystals that are yellow (negatively birefringent)
Diagnosis Definitive diagnosis only possible by aspirating and inspecting synovial fluid or tophaceous material and demonstrating MSU crystals Polarized microscopy, the crystals appear as bright birefringent crystals that are yellow (negatively birefringent)
Serum uric acid levels can be normal or low at the time of an acute attack, as inflammatory cytokines can be uricosuric and effective initiation of hypouricemic therapy can precipitate attacks. This limits the value of serum uric acid determinations for the diagnosis of gout. Nevertheless, serum urate levels are almost always elevated at some time and are important to use to follow the course of hypouricemic therapy.
Acute Gouty Arthritis: Precipitating Factors Surgery Alcohol Fluctuation of uric acid level initiation of therapy to lower uric acid level diuretics (esp. hydrochlorothiazide) aspirin low doses raise uric acid levels high doses lower uric acid levels
Differential Diagnosis Trauma Infections septic arthritis, gonococcal arthritis, cellulitis Inflammatory Rheumatic arthritis, Reiter’s syndrome, Psoriatic arthritis Metabolic pseudogout Miscellaneous Osteoarthrtis
Predisposing Factors Heredity Drug usage Renal failure Hematologic Disease Trauma Alcohol use Psoriasis Poisoning Obesity Hypertension Organ transplantation Surgery
Less commonly, chronic gouty arthritis will be the only manifestation, and, more rarely, the disease will manifest only as periarticular tophaceous deposits in the absence of synovitis
Prevalence increasing May be signal for unrecognized comorbidities : ( Not to point of searching) Obesity (Duh!) Metabolic syndrome DM HTN CV disease Renal disease
INTERCRITICAL More concentration of uric acid crystals Typically no need for drug intervention at the time.
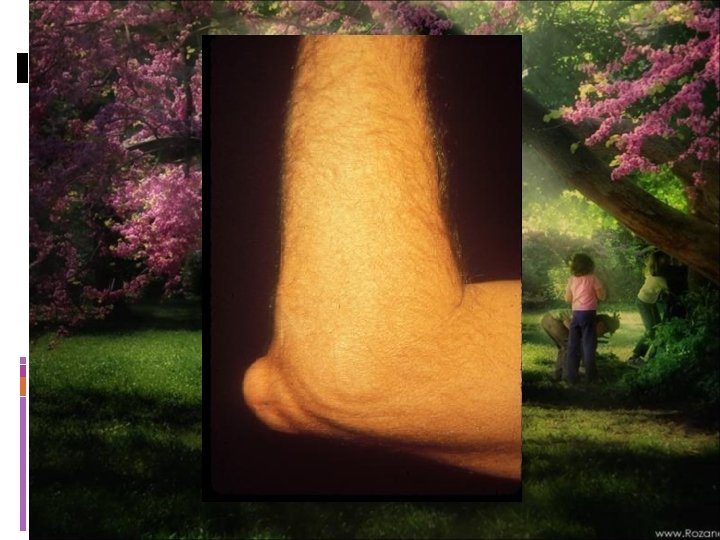
CHRONIC GOUT
Chronic Gout-Radiographic Features
Chronic Tophaceous Gout
CHRONIC GOUT
Chronic Tophaceous Gout
Questions?
Chronic Tophaceous Gout
CHRONIC Continuous or persistent over a long period of time Treatment required Not easily or quickly resolved
Diagnostic Studies Uric Acid Limited value as majority of hyperuricemic patients will never develop gout Levels may be normal during acute attack CBC Mild leukocytosis in acute attacks, but may be higher than 25, 000/mm ESR mild elevation or may be 2 -3 x normal 24 hr urine uric acid Only useful in patients being considered for uricosuric therapy or if cause of marked hyperuricemia needs investigation Trial of colchicine Positive response may occur in other types of arthritis to include pseudogout.
A 24 -h urine collection for uric acid can, in some cases, be useful in assessing the risk of stones, elucidating overproduction or underexcretion of uric acid, and deciding whether it may be appropriate to use a uricosuric therapy (. Excretion of >800 mg of uric acid per 24 h on a regular diet suggests that causes of overproduction of purine should be considered. Urinalysis, serum creatinine, hemoglobin, white blood cell (WBC) count, liver function tests, and serum lipids should be obtained because of possible pathologic sequelae of gout and other associated diseases requiring treatment and as baselines because of possible adverse effects of gout treatment.
MEDS- Decreased Urate Pool High dose Salicylate Losartan Fenofibrate Amlodipine Vitamin C Probenecid, sulfinpyrazone, benzbromarone Allopurinol, uricase, febuxostat
Diagnostic Studies Uric Acid Limited value as majority of hyperuricemic patients will never develop gout Levels may be normal during acute attack CBC Mild leukocytosis in acute attacks, but may be higher than 25, 000/mm ESR mild elevation or may be 2 -3 x normal 24 hr urine uric acid Only useful in patients being considered for uricosuric therapy or if cause of marked hyperuricemia needs investigation Trial of colchicine Positive response may occur in other types of arthritis to include pseudogout.
Diagnosing Gout X-rays Arthrocentesisextraction of joint fluid Examination of joint Patient medical history
Radiographic Features Early in the disease radiographic studies may only confirm clinically evident swelling. Cystic changes, well-defined erosions with sclerotic margins (often with overhanging bony edges), and soft tissue masses are characteristic features of advanced chronic tophaceous gout. Ultrasound, CT and MRI are being studied and are likely to become more sensitive for early changes
RADIOLOGIC SIGNS
X-RAYS
X-RAYS
Complications Renal Failure ARF can be caused by hyperuricemia, chronic urate nephropathy Nephrolithiasis Joint deformity Recurrent Gout
Questions?
Treatment Goals Gout can be treated without complications. Therapeutic goals include terminating attacks providing control of pain and inflammation preventing future attacks preventing complications such as renal stones, tophi, and destructive arthropathy
Treatment: Gout Acute Gouty Arthritis The mainstay of treatment during an acute attack is the administration of anti-inflammatory drugs such as nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, or glucocorticoids. NSAIDs are used most often in individuals without complicating comorbid conditions. Both colchicine and NSAIDs may be poorly tolerated and dangerous in the elderly and in the presence of renal insufficiency and gastrointestinal disorders. Ice pack applications and rest of the involved joints can be helpful.
The end
. Colchicine given orally is a traditional and effective treatment if used early in an attack. One useful regimen is one 0. 6 -mg tablet given every 8 h with subsequent tapering. This is generally better tolerated than the formerly advised hourly regimen. The drug must be stopped promptly at the first sign of loose stools, and symptomatic treatment must be given for the diarrhea. Intravenous colchicine has been taken off the market. NSAIDs given in full anti-inflammatory doses are effective in 90% of patients, and the resolution of signs and symptoms usually occurs in 5– 8 days. The most effective drugs are any of those with a short half-life and include indomethacin, 25– 50 mg tid; naproxen, 500 mg bid; ibuprofen, 800 mg tid; and diclofenac, 50 mg tid
Hypouricemic Therapy Ultimate control of gout requires correction of the basic underlying defect: the hyperuricemia. Attempts to normalize serum uric acid to <300– 360 mol/L (5. 0 – 6. 0 mg/d. L) to prevent recurrent gouty attacks and eliminate tophaceous deposits entail a commitment to long-term hypouricemic regimens and medications that generally are required for life
Colchicine given orally is a traditional and effective treatment if used early in an attack. One useful rm m m Hypouricemic Therapy 5 Ultimate control of gout requires correction of the basic G I underlying defect: the hyperuricemia. Attempts to e 3 normalize serum uric acid to <300– 360 mol/L (5. 0 i – 6. 0 mg/d. L) to prevent recurrent gouty attacks and g t eliminate tophaceous deposits entail a commitment to a long-term hypouricemic regimens and medications that i F generally are required for life f i t a o m 2 e t r e
SERUM URATE LEVELS Not reliable May be normal with flares May be high with joint Sx from other causes
Hypouricemic Therapy Ultimate control of gout requires correction of the basic underlying defect: the hyperuricemia. Attempts to normalize serum uric acid to <300 – 360 mol/L (5. 0– 6. 0 mg/d. L) to prevent recurrent gouty attacks and eliminate tophaceous deposits entail a commitment to long-term hypouricemic regimens and medications that generally are required for life.
Hypouricemic therapy should be considered when, as in most patients, the hyperuricemia cannot be corrected by simple means (control of body weight, low-purine diet, increase in liquid intake, limitation of ethanol use, decreased use of fructose -containing foods and beverages, and avoidance of diuretics
the decision to initiate hypouricemic therapy usually is made taking into consideration the number of acute attacks (urate lowering may be cost-effective after two attacks), serum uric acid levels [progression is more rapid in patients with serum uric acid >535 mol/L (>9. 0 mg/d. L)], the patient's willingness to commit to lifelong therapy, or the presence of uric acid stones. Urate-lowering therapy should be initiated in any patient who already has tophi or chronic gouty arthritis. Uricosuric agents such as probenecid can be used in patients with good renal function who underexcrete uric acid, with <600 mg in a 24 -h urine sample. Urine volume must be maintained by ingestion of 1500 m. L of water every day. Probenecid can be started at a dose of 250 mg twice daily and increased gradually as needed up to 3 g per day to maintain a serum uric acid level <360 mol/L (6 mg/d. L). Probenecid is generally not effective in patients with serum creatinine levels >177 mol/L (2 mg/d. L
Benzbromarone is another uricosuric drug that is more effective in patients with renal failure. Some agents used to treat common comorbidities, including losartan, fenofibrate, and amlodipine, have some mild uricosuric effects.
The xanthine oxidase inhibitor allopurinol is by far the most commonly used hypouricemic agent and is the best drug to lower serum urate in overproducers, urate stone formers, and patients with renal disease. It can be given in a single morning dose, 100– 300 mg initially and increasing up to 800 mg if needed. In patients with chronic renal disease, the initial allopurinol dose should be lower and adjusted depending on the serum creatinine concentration; for example, with a creatinine clearance of 10 m. L/min, one generally would use 100 mg every other day. Doses can be increased gradually to reach the target urate level of 6 mg/d. L; however, more studies are needed to provide exact guidance.
Toxicity of allopurinol has been recognized increasingly in patients who use thiazide diuretics and patients allergic to penicillin and ampicillin. The most serious side effects include life-threatening toxic epidermal necrolysis, systemic vasculitis, bone marrow suppression, granulomatous hepatitis, and renal failure. Patients with mild cutaneous reactions to allopurinol can reconsider the use of a uricosuric agent, undergo an attempt at desensitization to allopurinol, or take febuxostat, a new, chemically unrelated specific xanthine oxidase inhibitor
Febuxostat is approved at 40 or 80 mg once a day and does not require dose adjustment in mild to moderate renal disease. Patients can also pay increased attention to diet and should be aware of new alternative agents (see below). Urate-lowering drugs are generally not initiated during acute attacks but after the patient is stable and low-dose colchicine has been initiated to decrease the risk of the flares that often occur with urate lowering. Colchicine anti-inflammatory prophylaxis in doses of 0. 6 mg one to two times daily should be given along with the hypouricemic therapy until the patient is normouricemic and without gouty attacks for 6 months or as long as tophi are present.
Febuxostat is approved at 40 or 80 mg once a day and does not require dose adjustment in mild to moderate renal disease. Patients can also pay increased attention to diet and should be aware of new alternative agents (see below). Urate-lowering drugs are generally not initiated during acute attacks but after the patient is stable and low-dose colchicine has been initiated to decrease the risk of the flares that often occur with urate lowering. Colchicine anti-inflammatory prophylaxis in doses of 0. 6 mg one to two times daily should be given along with the hypouricemic therapy until the patient is normouricemic and without gouty attacks for 6 months or as long as tophi are present.
Colchicine should not be used in dialysis patients and is given in lower doses in patients with renal disease or with P gylcoprotein or CYP 3 A 4 inhibitors such as clarithromycin that can increase toxicity or colchicine. Pegloticase is a new uratelowering biologic agent that can be effective in patients allergic to or failing xanthine oxidase inhibitors. New uricosurics are undergoing investigation.
“Disease of Kings” Rich foods have a higher concentration of protein. This could cause major problems for a person afflicted with gout. ORGAN MEATS WILD GAME SEAFOOD LENTILS PEAS ASPARAGUS YEAST BEER
Newer Therapies Uricase Enzyme that oxidizes uric acid to a more soluble form Natural Uricase from Aspergillus flavus and Candida utilis under investigation Febuxostat New class of Xanthine Oxidase inhibitor More selective than allopurinol Little dependence on renal excretion Losartan ARB given as 50 mg/d. L can be urisuric. When given with HCTZ, it can blunt the effect of the diuretic and potentiate its antihypertensive action Fenofibrate Studies note when used in combo with Allopurinol produced additional lowering of the urate