Inflammatory Myopathies Susan Wallis MD Idiopathic inflammatory myopathies








 triad of")






















 • • Present in 30 -60% of patients")
: 161– 170")





: 233 -241")
: 233 -241")
: 233 -241")




: 161– 170")






 223– 236")

















 revealed a 50% mortality from")


- Slides: 76
Inflammatory Myopathies Susan Wallis, MD
Idiopathic inflammatory myopathies • Polymyositis • Dermatomyositis • Juvenile dermatomyositis • Inclusion body myositis • Myositis associated with collagen vascular disease • Myositis associated with malignancy
Idiopathic inflammatory myopathies • Polymyositis • Dermatomyositis • Juvenile dermatomyositis • Inclusion body myositis • Myositis associated with collagen vascular disease • Myositis associated with malignancy
Inflammatory myopathies • Rare heterogeneous group of acquired diseases characterized by inflammatory infiltrate of skeletal muscle. • Incidence of about 2 -10 per 1 million people per year in the United States. • Potentially treatable.
Polymyositis/Dermatomyositis • Heliotrope rash was first described in 1875 in France. • In 1888 the first American biopsy documented polymyositis in ruling out Trichinella. • 1930 Gottron reported skin lesions • 1967 the pathology of inclusion body myositis was described. Hochberg et al. Rheumatology 3 rd ed. 2003
Epidemiology • Bimodal age distribution in PM/DM – Between 10 -15 years in children – Between 45 -60 in adults • Inclusion body – More common after age 50 years • Female predominance
Differential diagnosis • Drugs and toxins: – – – – Chloroquine Colchicine Corticosteroids Heroin Alcohol Fibrates/statins AZT • Metabolic • Malignancy • Genetic – HLA-DRB 1 – HLA-DQA 1 – TNF 2(-308) • Infectious agents: – Bacteria • • Staphylococci Clostridia Rickettsias Mycobacteria – Parasites • • • Toxoplasma Trichnella Schistosoma Cysticerca Borrelia – Viruses • • Coxsackie Echo Influenze Adeno
Criteria to define polymyositis and dermatomyositis proposed by Bohan and Peter 1. Symmetric weakness of limb girdle muscles and anterior neck flexors. 2. Skeletal muscle histologic examination showing evidence of necrosis of types I and II muscle fibers, phagocytosis, regeneration with basophilia, large sarcolemmal nuclei and prominent nucleoli, atrophy in a perifascicular distribution, variation in fiber size, and an inflammatory exudate. N Engl J Med 292: 344, 1975
3. Elevation of levels of serum skeletal muscle enzymes 4. Electromyographic (EMG) triad of short, small polyphasic motor units; fibrillations, positive waves, and insertional irritability; and bizarre high-frequency discharges. 5. Dermatologic features including a heliotrope rash with periorbital edema; a scaly, erythematous dermatitis over the dorsa of the hands, especially over the MCP and PIP joints (Gottron's sign); and involvement of the knees, elbows, medial malleoli, face, neck, and upper torso.
Diagnostic criteria for IBM • Pathologic criteria – Electron microscopy: Microtubular filaments in the inclusions. – Light microscopy: • Lined vacuoles • Intranuclear or intracytoplasmic inclusions or both • Clinical criteria – Proximal muscle weakness – Distal weakness – EMG evidence of generalized myopathy – Increase in serum muscle enzymes – Failure of muscle weakness to improve on high-dose steroids
Polymyositis/Dermatomyositis • Occur sporadically or in association with other systemic autoimmune disease • More common in women than men. • DM common than PM. • DM can clinically manifest with heliotrope rash, Grotton’s papules, shawl rash, erythematous nailfolds, dermatomyositis sine myositis.
Clinical features • Progressive painless weakness – Difficulty lifting above head/combing hair – Difficulty arising from a low chair or toilet – Nasal regurgitation or choking when eating – Hoarseness, change in voice – *Ocular/facial muscle involvement is very uncommon • Fatigue • Fever
Other clinical features • Weight loss • Nonerosive inflammatory polyarthritis in rheumatoid-like distribution – Except in Jo-1 positive, can be erosive and deforming. • • Raynaud’s phenomenon Interstitial lung disease Cardiac abnormalities Amyopathic dermatomyositis
Deforming arthritis of anti-Jo 1 antibody patient
Inclusion body myositis • Can present with features identical to PM. • Onset is typically insidious and progression is slow. • May differ from PM in that it may include focal, distal or asymmetric weakness. • Dyspagia is a late occurrence. • CK only slightly increased and can be normal in up to 25% of patients.
Dermatologic manifestations www. jfponline. com/Pages. asp? AID=2763&UID=
Nailfold capillaries www. hakeem-sy. com/main/files/images/20_2. jpg
Cardiac • Myocarditis – With secondary arrhythmias and CHF – Myocardial fibrosis • Cor pulmonale – Secondary to ILD • Accelerated atherosclerosis associated with prolonged steroid use
Dyspnea • Non-pulmonary: respiratory muscle weakness, cardiac involvement • Pulmonary: – ILD: NSIP, UIP, diffuse alveolar damage, cryptogenic organizing pneumonia – Pulmonary hypertension – Alveolar hemorrhage – Infection: with or without aspiration – Drug induced
Pulmonary evaluation • CT scan – Increased interstitial markings • PFTs – Decreased TLV and DLCO • BAL – Abnormal number of leukocytes • Biopsy – Mononuclear cell infiltration, destruction of alveolar spaces and fibrosis
GI Tract • Pharyngeal muscle involvement – Dyphonia – Dysphagia • Postprandial symptoms of bloating, pain and distension • Pneumatosis cystoides intestinalis
Malignancy risk • Strong association between malignancy and dermatomyositis, but less clearly with polymyositis. – Ovarian, lung, pancreatic, stomach and colorectal and non-Hodgkin lymphoma • The overall risk is greatest in the first 3 years after diagnosis but is still increased through all years of follow-up.
Pathology
Inflammation • Dermatomyositis – B cells and CD 4 are abundant in the pervascular region. – MAC found in the perivascular areas and within intrafascicular capillaries – Damage to intrafascicular capillaries • Polymyositis and inclusion body myositis – Normal appearing muscle cells are invaded by T cells • PM/DM – Increased expression of costimulatory molecules
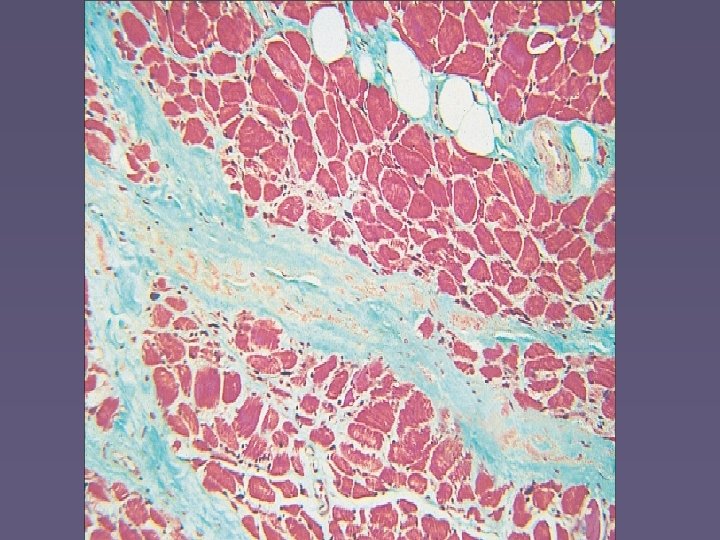
Polymyositis pleiad. umdnj. edu/. . . /muschtml/musc 008. htm Endomysial inflammatory infiltrate surrounding and invading non-necrotic muscle fibers www. neuropathologyweb. org/chapter 13
Dermatomyositis Necrotic and regenerating muscle fibers in perifascicular regions www. neuro. wustl. edu/. . . /pathol/dermmyo. htm www. phoenixneurology. com
Chronic dermatomyositis
Inclusion body myositis
Pathogenesis • Humoral – Autoantibodies • Directed against cell components • Directed at intracellular, ususally intracytoplasmic molecules • Usually part of the protein synthesis machinery • Cellular • Genetic
Autoantibodies • Autoantibodies have been identified in patients with myositis. – Not seen in inclusion body myositis • Can help predict specific syndromes. • Differentiate between types of idiopathic myositis versus myositis associated with other conditions.
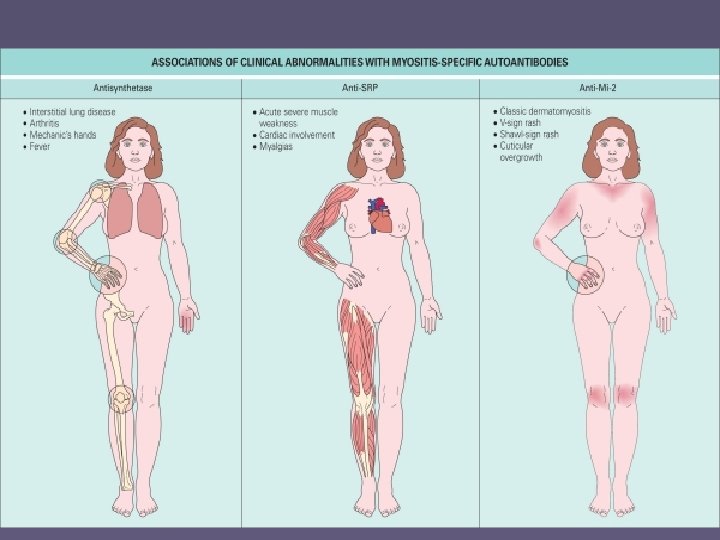
Autoantibodies • Myositis specific antibodies (MSA) • • Present in 30 -60% of patients with PM/DM Anti-aminoacyl-t. RNA synthetases (ARS). Anti-SRP Anti-Mi-2 Autoimmunity, 2006; 39(3): 161 -170
Autoimmunity, May 2006; 39(3): 161– 170
Clinical syndromes associated with specific antibodies
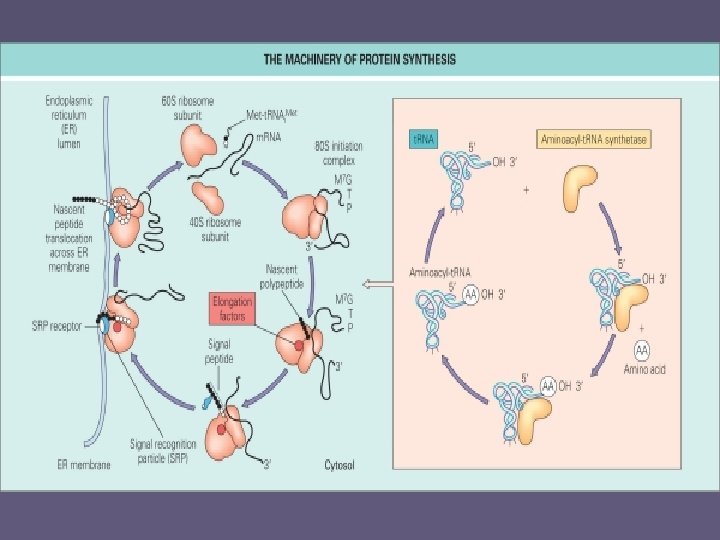
Antisynthetase syndrome • Aminoacyl-t. RNA-synthetase is a cytoplasmic enzyme involved in aminoacylation. • The most common ARS is histidyl-RNAsynthetase, also called Jo-1. www. arodia. com/. . . /order. By. Attribute__caption
Common characteristics • • • Myopathy Interstitial lung disease Raynaud’s phenomenon Polyarthritis Fever Mechanic’s hands
Anti-aminoacyl-t. RNA synthetase antibodies in clinical course prediction of interstitial lung disease complicated with idiopathic inflammatory myopathies • Aim of the study to determine if these antibodies were predictive of clinical course of ILD in idiopathic inflammatory myositis patients. • Retrospective study of 74 patients who met Peter-Bohan criteria. • The patients with ILD have a worse prognosis than those without. • Anti-ARS are strongly associated with ILD Autoimmunity 2006; 39(3): 233 -241
Prevalence of symptoms of patients with antisynthetase syndrome Autoimmunity 2006; 39(3): 233 -241
Interstitial lung disease Autoimmunity 2006; 39(3): 233 -241
Autoimmunity 2006; 39(3): 233 -241
Anti-SRP Antibodies • Cytoplasmic antibody • SRP is an RNA-protein complex that binds newly synthesized proteins and guides them to the endoplasmic reticulum for translocation.
Clinical • Very rare • Chiefly proximal muscle involvement with rhabdomyolysis • Usually poor response to steroids • ILD possible but uncommon • Skin and joints spared Joint, Bone, Spine. 2006; 73: 646 -654
Anti-Mi-2 • Antibodies directed to a nuclear macromolecular complex involved in transcription. • Strong specificity for dermatomyositis. • Usually good response to treatment.
Myositis Associated Antibodies • • • Anti-PM-Scl Anti-RNP Anti-Ro Anti-La Anti-Ku
Myositis-associated antigens Autoimmunity, May 2006; 39(3): 161– 170
Anti-PM-Scl antibodies • Directed against a nucleolar macromolecular complex • Primarily polymyositis or dermatomyositis/scleroderma overlap • Strongly associated with HLA-DR 3 • Seen in 5 -25% of patients with myositis.
Anti-U 1 -RNP • Sm-RNPs are ribonucleoproteins composed of 11 peptides and five small RNAs called U 1, U 2, U 4, U 5 and U 6. – Anti-U 1 -RNP is primary marker of an overlap syndrome. • Found in 5 -60% of patients with connective tissue disease and myositis.
Joint, Bone, Spine. 2006; 73: 646 -654.
Cellular Immunity • Lymphocyte accumulation • T cell receptor restriction in inflamed muscle • Cytokine activation • Increased expression of antigen presenting cells
• Factors that activate complement and the antigenic targets are unknown. • Lymphocytic infiltrates are B cells, CD 4+ cells and plasmacytoid/dendritic cells. • Complement activation upregulates cytokines, chemokines and adhesion molecules.
Dermatomyositis Complement activation C 5 b-C 9 deposition in endomysial capillares Capillary necrosis Perivascular inflammation Ischemia Muscle fiber destruction
Immunopathological changes in dermatomyositis Neuromuscular Disorders 16 (2006) 223– 236
Polymyositis • CD 8+ invade healthy non-necrotic muscle fibers. • MHC-class I antigen expressing muscle cells.
MHC-class I • MHC-class I expression is absent in normal muscle • Strongly up-regulated in pathologic conditions, especially in inflammatory myopathies. • A mouse model of overexpression of MHC class I molecules alone in skeletal muscle led to a self-sustaining inflammatory process. PNAS 2000; 97(16): 9209 -9214
Genetic Factors • HLA-DRB 1*0301, HLA-DQA 1 • Non-HLA class II genetic polymorphisms including IL-1 receptor antagonist and TNF -α. • Gene studies have been difficult to perform given rarity of disease. • Previous studies have combined DM and PM patients to increase power. Current Opinion in Rheumatology 2004; 16: 707 -713
T cell receptors • All the inflammatory myopathies are characterized by the presence of T cells and macrophages in muscle tissue. • Exogenous or endogenous antigen? • Previous studies looking at the TCR repertoire in myositis patients has been inconclusive.
Restricted T Cell Receptor BV Gene Usage in the Lungs and Muscles of Patients with Idiopathic Inflammatory Myopathies • Aim of study to compare TCR expression in 3 compartments that could be involved in patients with myositis: muscle, lung and peripheral blood. • Identify a common TCR Englund P et al. Arthritis and Rheumatism 2007; 56(1); 372 -383
• T cells recognize an antigen via complementary region of T cell receptors. • TCR is a heterodimer of two α and two β variable chain lesions. • TCR genes are restricted and amino acid sequences are conserved when T cells are selectively recruited by specific autoantigens.
Muscle biopsies showing localization of CD 4, CD 8 and BV 3 -expressing cells (brown cells). Arthritis and rheumatism 2007; 56(1)372 -383
Conclusion • Restricted accumulation of T lymphocytes expressing selected TCR V-gene segments. • Positive results from lung and muscle. • Suggests common target antigens. – Unidentified
Patient evaluation
Diagnosis • Biopsy is gold standard • EMG • MRI – STIR images for active myositis – Confirmation of amyopathic dermatomyositis – Documentation of flare
Disease activity assessment • Global activity- VAS • Muscle strength – Proximal and distal muscle evaluation • Physical function – HAQ • Laboratory assessment – >2 serum muscle enzymes • Extramuscular disease – Assess cutaneous, GI, articular, cardiac and pulmonary activity
If we do not know what causes it, how do we treat it? Immunotherapy
Anti-inflammatory and immunosuppressive • • • Steroids Azathioprine Cell. Cept Methotrexate Cytoxan Cyclosporin
Corticosteroids is mainstay of treatment in most cases • Start 1 -2 mg/kg/day • Continue until CPK returns to normal, then slow taper. • For severe acute disease, consider pulse dose steroids.
Other treatments • Steroid sparing – Methotrexate – Imuran • Non-responders – – – Rituxan IVIG Cyclosporin Cellcept Cyclophosphamide (also for ILD) – Plasmapheresis – ? TNF inhibitors
Additional follow-up • Cancer screening – Age appropriate – CAP CT scan – CA-125 and CA 19 -9 • Aggressive risk factor modification for atherosclerosis. • PT tailored to patient’s needs starting with passive ROM, stretching advancing to aerobic activity after recovery.
Prognosis • Older studies (before the availability of steroids) revealed a 50% mortality from complications. • Current estimates of mortality, excluding patients with malignancy, is less than 10% at 5 years after initial diagnosis.
Poor prognostic factors • • • Older age Malignancy Delayed steroid treatment Dysphagia with aspiration ILD
Bibliography Bradshaw EM, Orihuela A, Mc. Ardel S, Salajegheh M, Amato A, Hafler D, Greenberg S, O’Connor K. A local antigendriven humoral response is present in the inflammatory myopathies. J of Immun. 2007; 178: 547 -556. Ghirardello A, Zampieri S, Tarricone E, Iaccarino L, Bendo R, Briani c, rondinone R, Sarzi-Puttini P, Todesco S, Doria A. Clinical implications of autoantibody screening in patients with autoimmune myositis. Autoimmunity 2006; 39(3): 217 -221. Chinoy H, et al. In adult onset myositis, the presence of interstitial lung disease and myositis specific/associated antibodies are governed by HLA class II haplotype, rather than by myositis subtype. Arthritis Research and Therapy 2006; 8(1): R 13. Chinoy H, Ollier W, Cooper R. Have recent immunogenetic investigations increased our understanding of disease mechanisms in the idiopathic inflammatory myopathies? Curr Opin Rheumatol 2004; 16: 707 -713. Chong B, Wong H. Immunobiologics in the treatment of psoriasis. Cin. Immunol 2007. Dalakas MC. Therapeutic targets in patients with inflammatory myopathies: present approaches and a look to the future. Neuromuscular Disorders 2006; 16: 223 -236. Englund P, Wahlstrom J, Fathi M, Rasmussen E, Grunewald J, Tornling G, Lundberg I. Restricted T cell receptor BV gene usage in the lungs and muscles of patients with idiopathic inflammatory myopathies. Arthritis and Rheumatism 2007; 56(1): 372 -383. Hassan AB, Nikitina-Zake L, Sanjeevi CB, et al. Association of the proinflammatory haplotypes (MICA 5. 1/TNF 2/TNFa 2/DRB 103) with polymyositis and dermatomyositis. Arthritis Rheum 2004; 50: 1013 -1015. Hochberg et al, eds. Rheumatology 2003. Kanneboyina N, Raben N, Loeffler L, et al. Conditional up-regulation of MHC class I in skeletal muscle leads to selfsustaining autoimmune myositis and myositis-specific autoantibodies. Nagaraju K, Raben N, Loeffler L, et al. Conditional up-regulation of MHC class I in skeletal muscle leads to selfsustaining autoimmune myositis and myositis-specific autoantibodies. PNAS 2000; 97(16): 9209 -9214. Sordet C, Goetz J, Sibilia J. Contribution of autoantibodies to the diagnosis and nosology of inflammatory muscle disease. Joint Bone Spine 2006; 73: 646 -654 Wiendl H, Mitsdoerffer M, Hofmeister V, et al. The non-classical MHC molecule HLA-G protects human muscle cells from immune-mediated lysis; implications for myoblast transplantation and gene therapy. Brain 2003; 126: 176 -185. Van der Pas J, Hengstman GJ, Laak HJ, Borm GF, van Engelen BGM. Diagnositc value of MHC class I staining in idiopathic inflammatory myopathies. J Neurol. , Neursurg. , Psychiatry 2004; 75: 136 -139. Volkland J, et al. A humanized monoclonal antibody against interleukin-2 that can inactivate the cytokine/receptor complex. Molec Immunol. 2007; 44: 1743 -1753.