SOFT TISSUE RHEUMATISM Dr A noori Rheumatologist www


,")
 Ø Glenohumeral joint (1%) Ø Refferal pain")














")


















 Ø Diagnosis: underlying disease (FBS), X-Ray MRI, arthrography")







 Lateral epicondylitis, or tennis elbow, : painful condition involving the")




, F=M ØEtiology: inflammation of common")

")






 Ø Epidemiology: F/M=5/1, symptomatic CTS (3% F,")

 Ø weakness and atrophy in chronic cases,")



")






 Ø Etiology: inflammation of tendon sheaths")












 Ø Etiology: any knee disease with synovial")
,")













- Slides: 119
SOFT TISSUE RHEUMATISM Dr. A. noori Rheumatologist www. arrh. ir
A number of periarticular disorders have become increasingly common over the past two to three decades, . Periarticular disorders most commonly affect the knee or shoulder.
Excessive frictional forces from overuse, trauma, systemic disease (e. g. , rheumatoid arthritis, gout), infection may cause bursitis and tendinitis.
Soft Tissue Rheumatism Shoulder Ø Periarthritis (80%) Ø Glenohumeral joint (1%) Ø Refferal pain (15%)
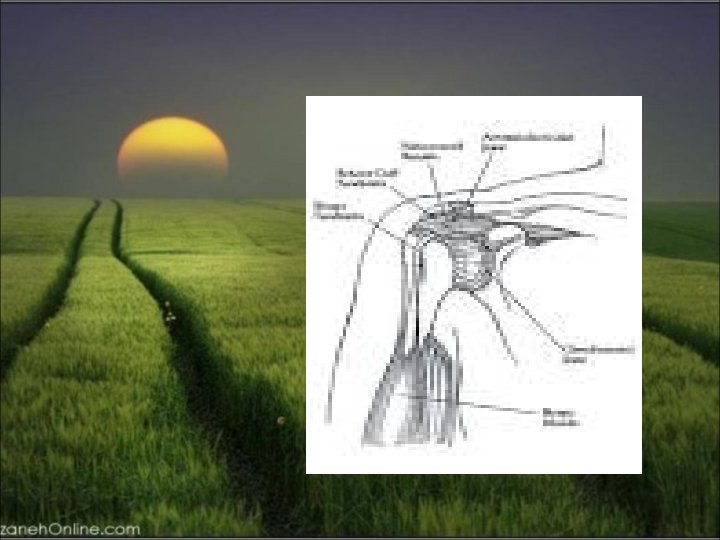
Soft Tissue Rheumatism shoulder Region ØRotator Cuff Tear ØBicipital tendinitis ØRotator Cuff tendinitis ØAdhesive capsulitis ØCalcific tendinitis
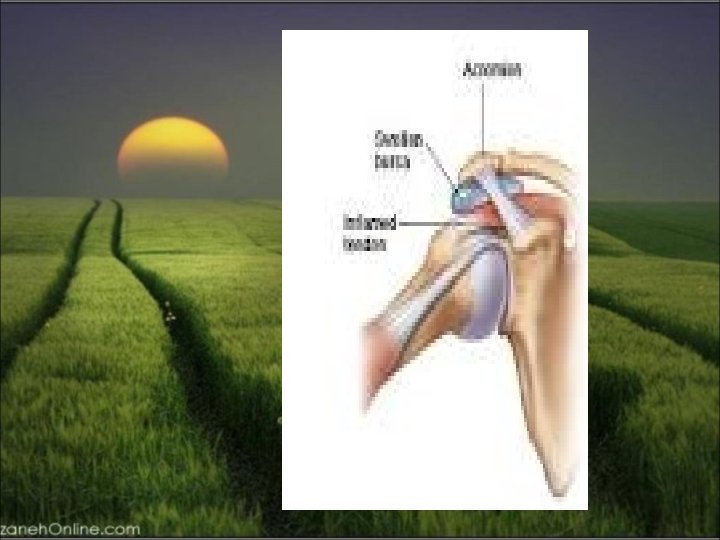
ØRotator Cuff tendinitis
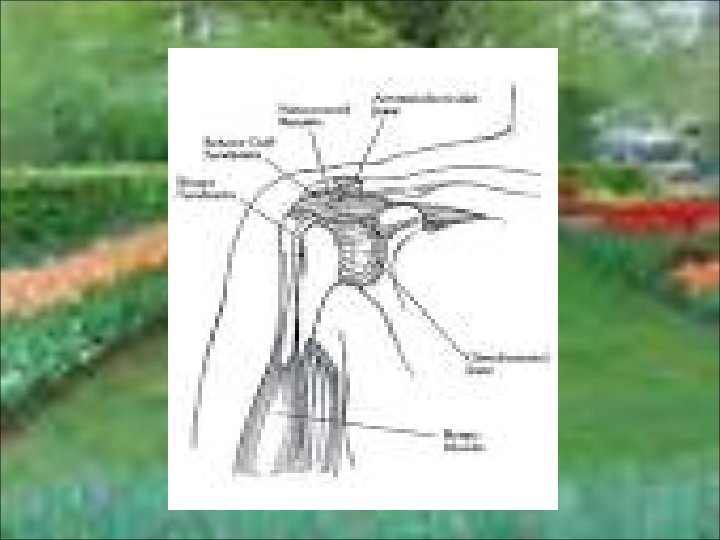
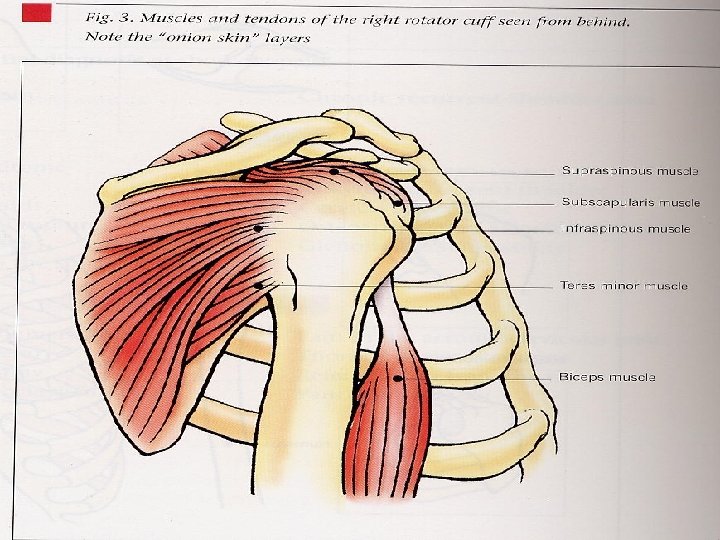
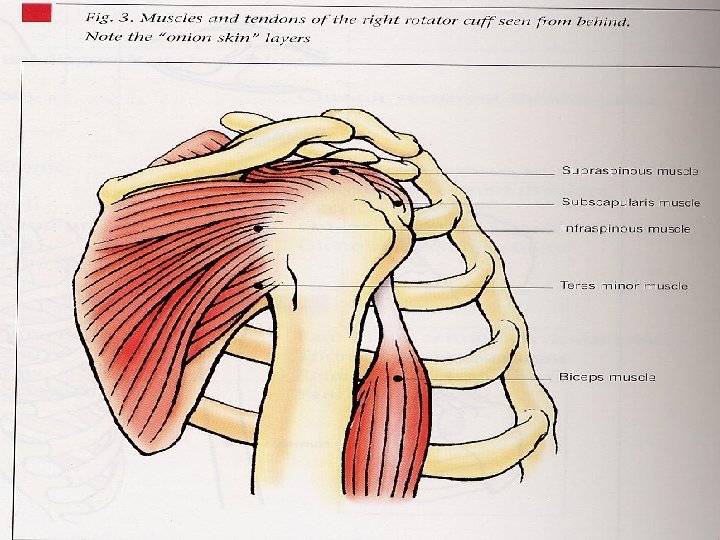
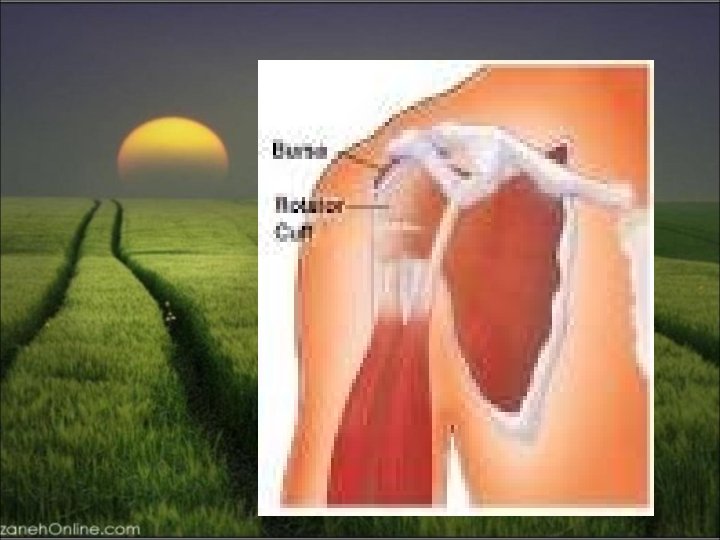
Tendinitis of the rotator cuff is the major cause of a painful shoulder and is currently thought to be caused by inflammation of the tendon(s). The rotator cuff consists of the tendons of the supraspinatus, infraspinatus, subscapularis, and teres minor muscles, and inserts on the humeral tuberosities.
Soft Tissue Rheumatism Rotator Cuff Tendinitis Ø Epidemiology: F>M, age>40 Ø Most common cause of shoulder pain Ø Etiology: overuse, especially with activities involving elevation of the arm with some degree of forward flexion. Impingement syndrome occurs in persons participating in baseball, tennis, swimming, or occupations that require repeated elevation of the arm
Soft Tissue rheumatism Impingement Of Rotator Cuff
Soft Tissue Rheumatism Rotator Cuff Tendinitis Ø Clinical manifestation: Patients complain of a dull aching in the shoulder, which may interfere with sleep. Severe pain is experienced when the arm is actively abducted into an overhead position. The arc between 60° and 120° is especially painful. Tenderness is present over the lateral aspect of the humeral head just below the acromion
Soft Tissue Rheumatism Painful Arc
ØTreatment NSAIDs, local glucocorticoid : injection, and physical therapy may relieve symptoms. Surgical decompression of the subacromial space may be necessary in patients refractory to conservative treatment.
Soft Tissue Rheumatism Injection of Subacromion Bursa
Soft Tissue Rheumatism Rotator Cuff Tear Ø Epidemiology: F>M, middle and old ages Ø Etiology: trauma, fracture or dislocation of shoulder joint, degeneration, rotator cuff tendinitis Ø Clinical manifestation: pain and weakness on abduction, drop arm sign Ø Diagnosis: X-Ray, ultrasound, arthrography; MRI Ø Treatment: acute tearing in young patients (surgery), steroid injection (after 6 weeks in acute form), physical therapy
Soft Tissue Rheumatism Rotator Cuff Tear Ø Epidemiology: F>M, middle and old ages Ø Etiology: trauma, fracture or dislocation of shoulder joint, degeneration, rotator cuff tendinitis Ø Clinical manifestation: pain and weakness on abduction, drop arm sign Ø Diagnosis: X-Ray, ultrasound, arthrography; MRI
Patients may tear the supraspinatus tendon acutely by falling on an outstretched arm or lifting a heavy object. Symptoms : pain along with weakness of abduction and external rotation of the shoulder. Atrophy of the supraspinatus muscles develops.
The diagnosis : arthrogram, ultrasound, or MRI. Surgical repair may be necessary in patients who fail to respond to conservative measures. In patients with moderate-to-severe tears and functional loss, surgery is indicated.
Soft Tissue Rheumatism Shoulder Arthrogram (Rotator Cuff)
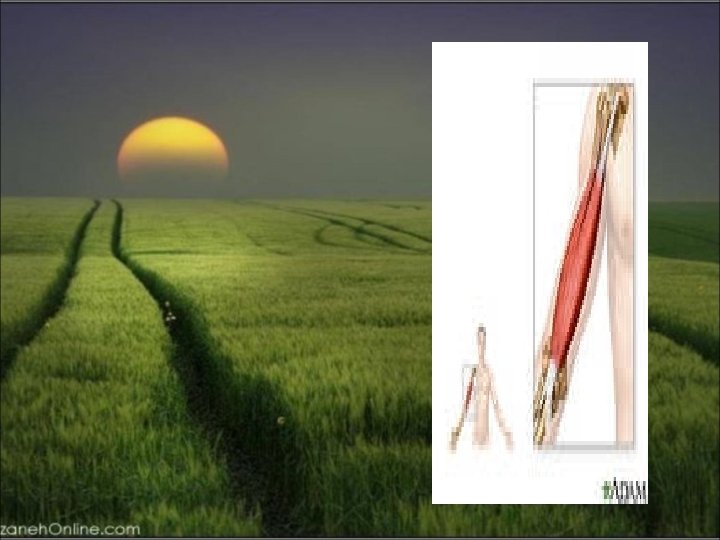
Soft Tissue Rheumatism Bicipital Tendon
Bicipital Tendinitis and Rupture § Bicipital tendinitis, or tenosynovitis, is produced by friction on the tendon of the long head of the biceps as it passes through the bicipital groove. When the inflammation is acute, patients experience anterior shoulder pain that radiates down the biceps into the forearm
Soft Tissue Rheumatism Bicipital Tendinitis ØEtiology: sport injury, special activity ØClinical manifestation: acute or chronic pain on anterior of shoulder, tenderness on palpation of bicipital groove, associated with Rotator cuff tendinitis
Soft Tissue Rheumatism Bicipital Tendinitis ØDiagnosis: yergason’s sign, speed test, pope eye sign (tendon rupture) ØTreatment: rest, physical therapy, NSAIDs, steroid injection, surgery
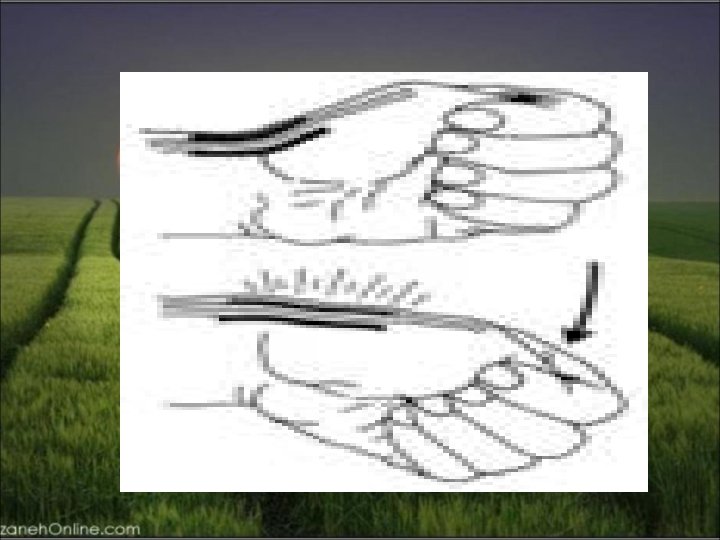
. Abduction and external rotation of the arm are painful and limited. Pain may be elicited along the course of the tendon by resisting supination of the forearm with the elbow at 90° (Yergason's supination sign).
Soft Tissue Rheumatism Yergason’s Sign And Speed Test
Acute rupture of the tendon may occur with vigorous exercise of the arm and is often painful. In a young patient, it should be repaired surgically.
Rupture of the tendon in an older person : little or no pain and is recognized by the presence of persistent swelling of the biceps ("Popeye" muscle) produced by the retraction of the long head of the biceps. Surgery is usually not necessary in this setting
Calcific Tendinitis deposition of calcium salts, primarily hydroxyapatite, within a tendon. The exact mechanism of calcification is not known but may be initiated by ischemia or degeneration of the tendon. The supraspinatus tendon is most often affected because it is frequently impinged on and has a reduced blood supply when the arm is abducted.
Calcific Tendinitis The condition usually develops after age. 40. Calcification within the tendon may evoke acute inflammation, producing sudden and severe pain in the shoulder. However, it may be asymptomatic or not related to the patient's symptoms
Soft Tissue Rheumatism Calcific Tendinitis
Adhesive Capsulitis Often referred to as "frozen shoulder, " adhesive capsulitis : pain and restricted movement of the shoulder, usually in the absence of intrinsic shoulder disease. Adhesive capsulitis may follow bursitis or tendinitis of the shoulder.
Adhesive Capsulitis associated with systemic disorders such as chronic pulmonary disease, myocardial infarction, and diabetes mellitus. Prolonged immobility of the arm contributes to the development of adhesive capsulitis. Pathologically, the capsule of the
Adhesive capsulitis : commonly in women after age 50. Pain and stiffness usually develop gradually but progress rapidly in some patients. Night pain is often present in the affected shoulder and pain may interfere with sleep. The shoulder is tender to palpation, and both active and passive movement are restricted. Radiographs of the shoulder show osteopenia. .
The diagnosis is typically made by physical examination but can be confirmed if necessary by arthrography, in that only a limited amount of contrast material, usually <15 m. L, can be injected under pressure into the shoulder joint.
In most patients, the condition improves spontaneously 1– 3 years after onset. While pain usually improves, many patients are left with some limitation of shoulder motion. Early mobilization of the arm following an injury to the shoulder may prevent the development of this disease. Physical therapy: the foundation of treatment for adhesive capsulitis.
Local injections of glucocorticoids and NSAIDs may also provide relief of symptoms. Slow but forceful injection of contrast material into the joint may lyse adhesions and stretch the capsule, resulting in improvement of shoulder motion. Manipulation under anesthesia may be helpful in some patients. , . ; /
Soft Tissue Rheumatism Adhesive Capsulitis (2) Ø Diagnosis: underlying disease (FBS), X-Ray MRI, arthrography (loss of joint cavity space) Ø Treatment: NSAIDs, steroid (local injection or systemic), physical therapy (pendulum exercise, wall climbing), manipulation under anesthesia in refractory cases
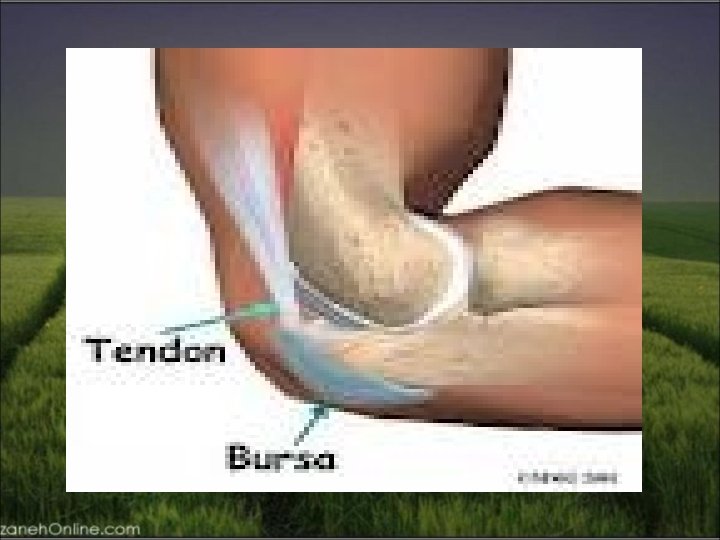
Soft Tissue Rheumatism Elbow Region ØLateral epicondylitis ØMedial Epicondylitis ØOlecranon bursitis ØUlnar nerve entrapment
Soft Tissue Rheumatism Olecranon Bursitis Ø Etiology: low grade chronic trauma _inflammatory arthritis, septic Ø Clinical manifestation: pain and tenderness is minimal , clear or blood tinged fluid in aspiration Ø Treatment: avoid special habit, fluid aspiration and steroid injection, antibiotic in septic bursitis, surgery in refractory cases
Soft Tissue Rheumatism Muscle Insertions Around The Elbow Joint
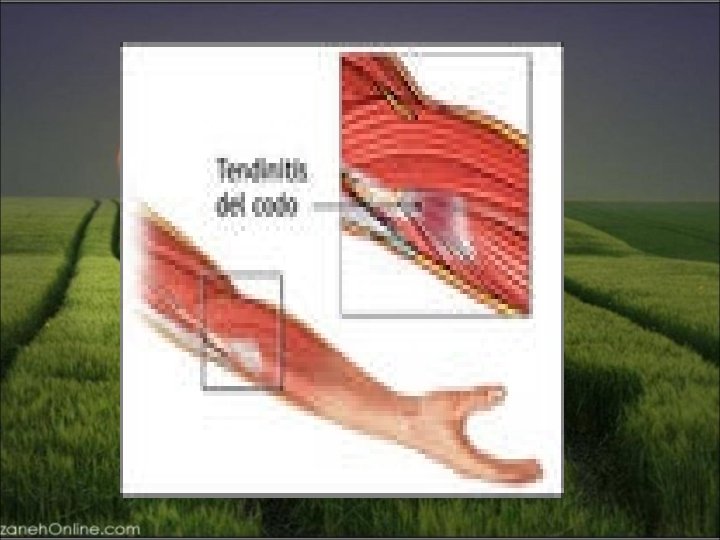
Lateral Epicondylitis (Tennis Elbow) Lateral epicondylitis, or tennis elbow, : painful condition involving the soft tissue over the lateral aspect of the elbow. The pain originates at or near the site of attachment of the common extensors to the lateral epicondyle and may radiate into the forearm and dorsum of the wrist. The pain usually appears after work or recreational activities involving repeated motions of wrist extension and supination against resistance.
Soft Tissue Rheumatism Resisted Wrist Extension Test
Soft Tissue Rheumatism Muscle Insertions Around The Elbow Joint
Soft Tissue Rheumatism Lateral Epicondylitis ØEpidemiology: ages (35 -50), F=M ØEtiology: inflammation of common extensor tendon, tennis player, gardening, ØClinical manifestation: pain in lateral epicondyle, radiation to forearm, weakness on grasping, differentiation with radial nerve entrapment
Treatment usually rest along with administration of an NSAID. Ultrasound, icing, and friction massage may also help relieve pain. When pain is severe, the elbow is placed in a sling or splinted at 90° of flexion.
Soft Tissue Rheumatism Lateral Epicondylitis ØDiagnosis: pain on resisted wrist extension, X-Ray (calcification, exostosis) ØTreatment: NSAIDs, physical therapy, steroid injection, surgery (>6 months),
Medial Epicondylitis Medial epicondylitis is an overuse syndrome resulting in pain over the medial side of the elbow with radiation into the forearm. The cause of this syndrome is considered to be repetitive resisted motions of wrist flexion and pronation, .
. patients >35 years and is much less common than lateral epicondylitis. It occurs most often in work-related : : swinging a golf club (golfer's elbow) or throwing a baseball. On physical examination, there is tenderness just distal to the medial epicondyle over the origin of the forearm flexors. Pain can be reproduced by resisting wrist flexion and pronation with the elbow extended.
Soft Tissue Rheumatism Resisted Wrist Flexion Test
Treatment s conservative, involving rest, NSAIDs, friction massage, ultrasound, and icing splinting. Injections of glucocorticoids at the painful site may also be effective. Patients should be instructed to rest for at least one month. Also, patients should start physical therapy once the pain has subsided. In patients with chronic debilitating medial epicondylitis that remains unresponsive after at least a year of treatment, surgical release of the flexor muscle at its origin may be necessary and is often successful.
Soft Tissue Rheumatism wrist And Hand Region ØCarpal tunnel syndrome ØDe quervain’s tenosynovitis ØTrigger finger ØGanglion ØDupuytren’s contracture
Soft Tissue Rheumatism Anatomy Of Carpal Tunnel
Soft Tissue Rheumatism Carpal Tunnel Syndrome (1) Ø Epidemiology: F/M=5/1, symptomatic CTS (3% F, 2% M), peak age (30 -60) Ø Etiology: Inflammatory disease (RA, SLE, PSS), crystal arthropathy, job trauma, local (osteophyte, tumors), metabolic (DM 6%, myxedema, acromegaly), infection (tuberculosis, fungal, rubella), pregnancy, idiopathic Ø Clinical manifestation: nocturnal symptom (
Soft Tissue Rheumatism Sensory Supply To The Hand
Soft Tissue Rheumatism Carpal Tunnel Syndrome (2) Ø weakness and atrophy in chronic cases, Phalen’s maneuver (40 -80% sensitivity and specificity), Tinel’s sign (sensitivity 25 -60%, specificity 68 -87%), tourniquet test Ø Diagnosis: physical examination, EMG-NCV Treatment: treating : Ø splinting, NSAID’s, steroid (local injection or systemic), , surgery (sever symptom>1 year, atrophy
Soft Tissue Rheumatism Tinel’s Sign And Phalen’s Test
Soft Tissue Rheumatism Thenar Muscle Atrophy
Soft Tissue Rheumatism Carpal Tunnel Syndrome (Local Injection)
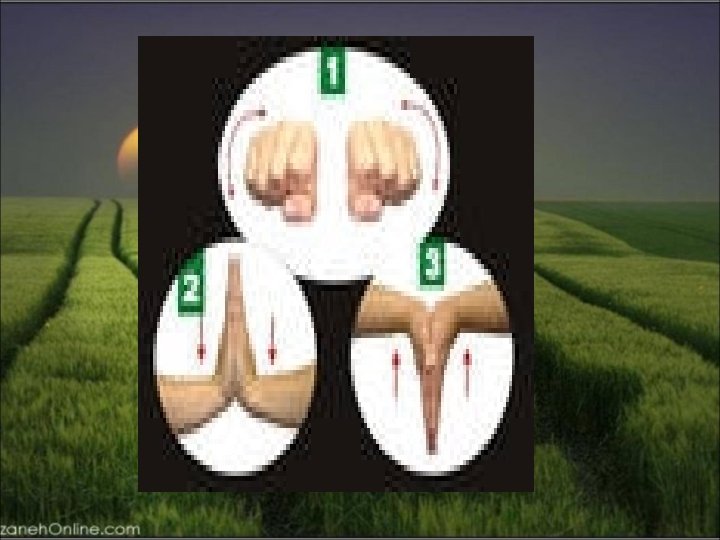
Soft Tissue Rheumatism De Quervain’s Tenosynovitis Ø Epidemiology: age>40, F>M Ø Etiology: repetitive activity with thumb pinching and moving wrist, inflammation of tendon sheath (abductor pollicis longus and extensor pollicis brevis) Ø Clinical manifestation: pain and tenderness, swelling over the radial styloid, Finkelstein test Ø Treatment: rest, NSAID’s, local steroid injection, surgery in refractory cases
Soft Tissue Rheumatism De Quervain’s Tenosynovitis
Soft Tissue Rheumatism Finkelstein Test
Soft Tissue Rheumatism Dupuytren’s Contracture
Soft Tissue Rheumatism Flexor Tendon Sheaths Of The Hand
Soft Tissue Rheumatism Dupuytren’s Contracture Ø Epidemiology: F/M 1/5, white man Ø Etiology: shortening and thickening of palmar fascia, hereditary, alcoholism, epilepsy, DM, any chronic disease Ø Clinical manifestation: 4 th, flexion contracture of one or more digits, in decreasing order (5 th 3 th, 2 th fingers) Ø Treatment: physical therapy, steroid injection, colchicin, vitamin E, surgery
Soft Tissue Rheumatism Volar Flexor Tenosynovitis (Trigger Fingers) Ø Etiology: inflammation of tendon sheaths of flexor digitorum, trauma, inflammatory disease (RA, psoriatic arthritis, crystal arthropathy, overused, osteoarthritis Ø Clinical manifestation: painful finger flexion (middle and index fingers), swelling, tenderness and nodule proximal to MCP joint in the volar side, Ø treatment: rest, physical therapy, NSAID’s, steroid injection, surgery
Soft Tissue Rheumatism Ganglion Ø Epidemiology: ages 20 -40, F=M Ø Etiology: cystic swelling arising from a joint or tendon sheath, trauma, prolonged wrist extension Ø Clinical manifestation: swelling and discomfort on wrist extension Ø Treatment: splint, rest, physical therapy, NSAID’s, steroid injection, surgery
Soft Tissue Rheumatism Ganglion Ø Epidemiology: ages 20 -40, F=M Ø Etiology: cystic swelling arising from a joint or tendon sheath, trauma, prolonged wrist extension Ø Clinical manifestation: swelling and discomfort on wrist extension Ø Treatment: splint, rest, physical therapy, NSAID’s, steroid injection, surgery
SOFT TISSUE RHEUMATISM LOWER EXTREMITY
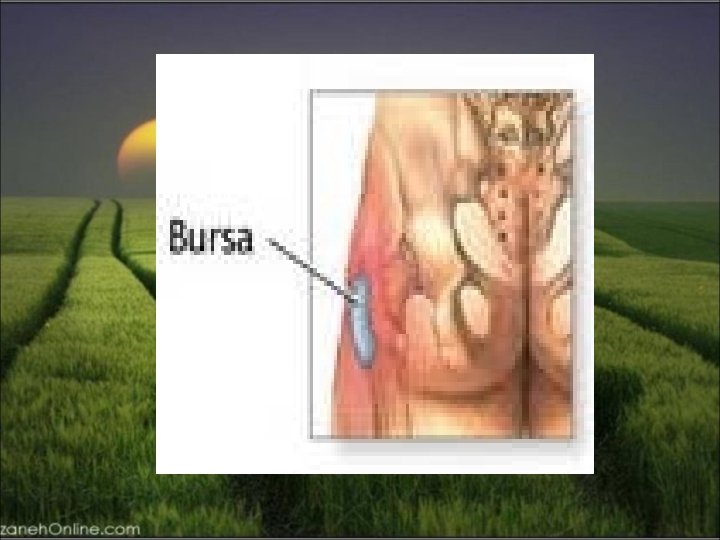
Soft Tissue Rheumatism Hip Region ØTrochantric bursitis ØIliopsoas bursitis ØIschial bursitis
Soft Tissue Rheumatism The Bursa Of The Hip Joint
Soft Tissue Rheumatism Trochantric Bursitis Ø Epidemiology: age 30 -70, F>M Ø Etiology: local trauma, osteoarthritis of hip and lumbar spine, scoliosis, leg-length discrepancy, inflammatory conditions Ø Clinical manifestation: pain on moving and lying on the involved side, pain in external rotation and abduction against resistance, calcification in X-Ray Ø Treatment: NSAID’s, steroid injection
Soft Tissue Rheumatism Iliopsoas Bursitis Ø Etiology: trauma, inflammatory conditions, septic, communication with hip joint (15%) Ø Clinical manifestation: groin and anterior thigh pain, exacerbation of pain with hyperextension of hip, cystic mass (30%), femoral venous obstruction Ø Diagnosis: X-Ray with contrast media, MRI Ø Treatment: NSAID’s, steroid injection, surgery
Soft Tissue Rheumatism CT Scan Of Iliopsoas Bursitis
Soft Tissue Rheumatism Ischial Bursitis Ø Etiology: trauma, prolonged sitting on hard surface, weaver’s bottom Ø Clinical Manifestation: radiation of pain to back of the thigh, local tenderness Ø Treatment: modified activity, cushion’s, NSAID’s, steroid injection with caution
Soft Tissue Rheumatism Meralgia Paresthetica Ø Etiology: obesity, pregnancy, diabetes, direct trauma, compression from corset, leg-length discrepancy Ø Clinical manifestation: hyperesthesia and numbness of anterolateral thigh, exacerbation of pain with , extension and abduction of thigh, prolonged standing and walking, Decreased touch and pinprik sensation Ø Diagnosis: NCV Ø Treatment: weight loss, steroid injection (medial to anterior superior iliac spine
Soft Tissue Rheumatism Meralgia Paresthetica
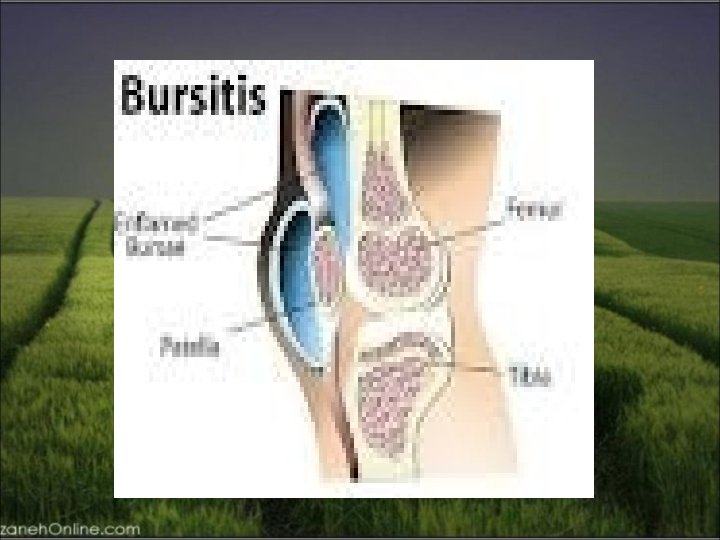
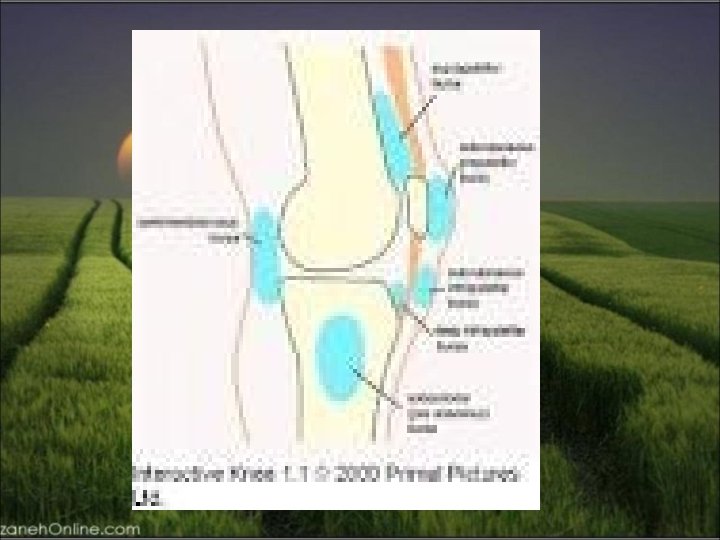
Soft Tissue Rheumatism knee Region ØPopliteal cyst ØPrepatellar and infrapatellar bursitis ØAnserine bursitis ØPatellar tendinitis
Soft Tissue Rheumatism Popliteal Cyst (Baker’s Cyst) Ø Etiology: any knee disease with synovial effusion (mechanical and inflammatory), naturally occurring communication between knee joint and semimembranosusgastrocnemius bursa (40%) Ø Clinical manifestation: diffuse swelling and pain of calf, erythema and edema of ankle (ceresent sign), mimiking thrombophlebitis Ø Diagnosis: ultrasound, arthrography, MRI Ø Treatment: rest, aspiration and steroid injection, surgery
Soft Tissue Syndrome Prepatellar and Infrapatellar Bursitis Ø Etiology: trauma, frequent kneeling (housemaid’s knee), inflammatory (gout, septic) Ø Clinical manifestation: pain, tenderness, swelling, hotness and redness (septic) Ø Treatment: aspiration and culture, steroid injection, modified activity
Soft Tissue Rheumatism Anserine Bursitis Ø Epidemiology: age 30 -50, F>M Ø Etiology: inflammation ) include, tendons of gracilis, sartorius, semitendinosus, osteoarthritis of knee, obese Ø Clinical manifestation: pain and tenderness over the medial aspect of the knee (2 inch below the joint margin Ø Treatment: rest, stretching of adductor and quadriceps muscles, NSAID’s, steroid injection
The diagnosis of plantar fasciitis can usually be made on the basis of history and physical examination alone. Patients experience severe pain with the first steps on arising in the morning or following inactivity during the day. The pain usually lessens with weight-bearing activity during the day, only to worsen with continued activity. Pain is made worse on walking barefoot or up stairs. On examination, maximal tenderness is elicited on palpation over the inferior heel corresponding to the site of attachment of the plantar fascia
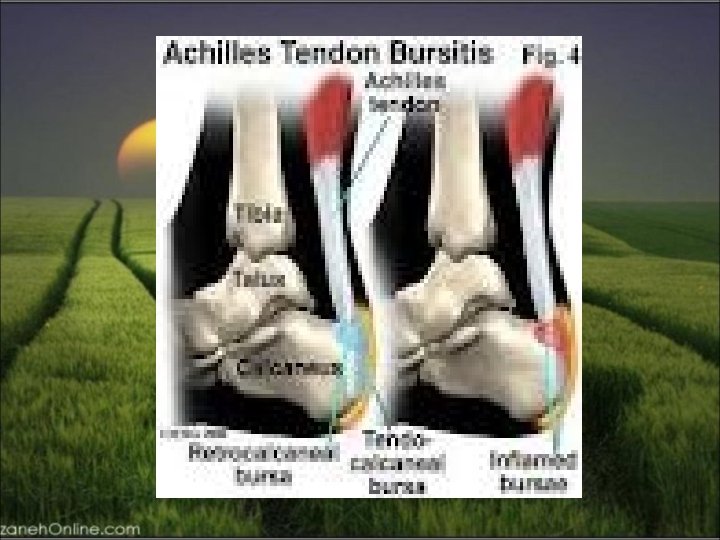
Soft Tissue Rheumatism Retrocalcaneal Bursitis Ø Etiology: inflammation of the bursa between the posterior surface of the achille tendon and the calcaneous, trauma, inflammatory arthritis (especially spondyloarthropathy) Ø Clinical manifestation: pain on dorsiflexion, tenderness, local swelling and bulging Ø Diagnosis: physical diagnosis, MRI, ultrasound Ø Treatment: rest, splint, NSAID’s,
Soft Tissue Rheumatism Subcutaneous Achilles Bursitis Ø Etiology: pressure of shoes, bony exostoses; sondyloarthropathy Ø Clinical manifestation: pain, swelling and redness Ø Treatment: relief from shoe pressure, treatment of underlying disease
Soft Tissue Rheumatism Achilles tendinitis Ø Etiology: trauma, athletic injury, fitting shoes, inflammatory conditions (especially spondyloarthropathy) Ø Clinical manifestation: pain on dorsiflexion, swelling, crepitus on motion Ø Diagnosis: MRI, ultrasound Ø Treatment: rest, splint (slight plantar flexion), NSAID’s
Soft Tissue Rheumatism Plantar Fascia
Soft Tissue Rheumatism Plantar Fasciitis Ø Etiology: athletic over activity, prolonged walking, improper shoes, spondyloarthropathy Ø Clinical manifestation: pain (morning upon arising, initial improvement, worsen later in the day), burning, aching, tenderness on palpation of medial calcaneal tubercle Ø Diagnosis: rest, heel pad, NSAID’s, orthoses, steroid injection
Soft Tissue Rheumatism Hallux Valgus-Bunion Ø Etiology: deviation of the large toe, genetic tendency, improper shoes, inflammatory arthritis, osteoarthritis Ø Clinical manifestation: deformity, local tenderness and redness (bunion), X-Ray (osteoarthritis of first MTP) Ø Treatment: orthoses and bunion pads, NSAID’s, surgery