TREATMENT OF VTE Dr MOHSEN SHAFIEPOUR PULMONOLOGIST TREATMENT



.")
, one")
anticoagulates by binding to and accelerating the activity of antithrombin, thus")







")


 are administered in a fixed dose, establish")


 to neutralize 100 units of heparin <1/2 hr: 1 -1.")

;")

. With less serious")














- Slides: 56
TREATMENT OF VTE Dr. MOHSEN SHAFIEPOUR /PULMONOLOGIST
TREATMENT OF DVT: Primary therapy: consists of clot dissolution with pharmacomechanical therapy that usually includes low-dose catheter-directed thrombolysis. This approach is reserved for patients with extensive femoral, iliofemoral, or upper extremity DVT SECONDARY PREVENTION: Anticoagulation or placement of an inferior vena caval (IVC) filter , below-knee graduated compression stockings may be prescribed, (usually 30– 40 mm. Hg)
TREATMENT OF Pulmonary RISK STRATIFICATION Embolism Hemodynamic instability, RV dysfunction on echocardiography, RV enlargement on chest CT, or elevation of the troponin level due to RV microinfarction portend a high risk of an adverse clinical outcome despite anticoagulation
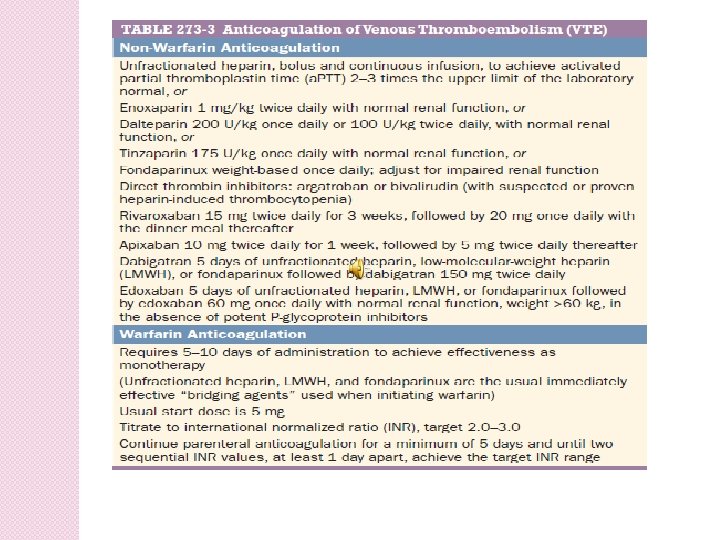
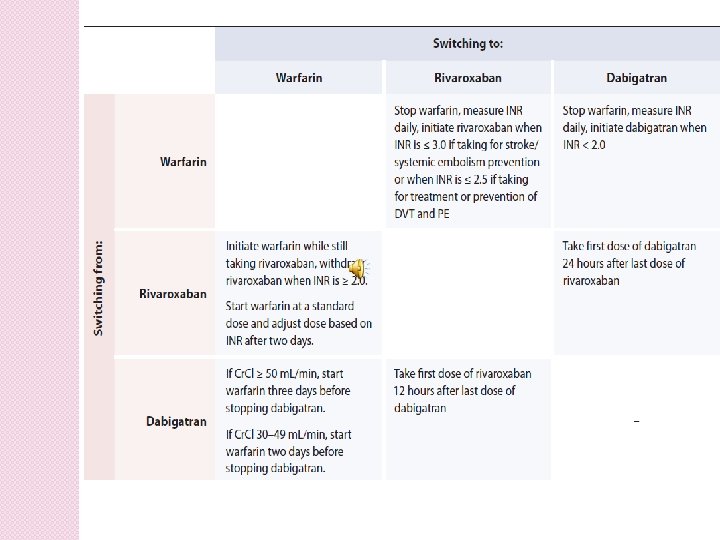
ANTICOAGULATION Effective anticoagulation is the foundation for successful treatment of DVT and PTE. (1). the classical (parenteral anticoagulation with warfarin) (2). parenteral therapy switched after 5 days to a novel oral anticoagulant (3). oral anticoagulation monotherapy
For patients with VTE in the setting of suspected or proven heparin-induced thrombocytopenia(HIT), one can choose between two parenteral direct thrombin inhibitors: argatroban and bivalirudin
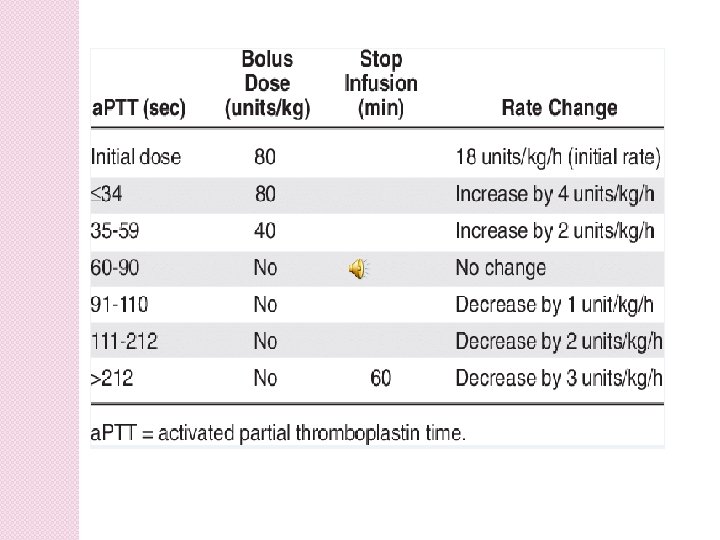
Unfractionated Heparin (UFH )anticoagulates by binding to and accelerating the activity of antithrombin, thus preventing additional thrombus formation. UFH is dosed to achieve a target activated partial thromboplastin time (a. PTT) of 60– 80 s. The most popular nomogram uses an initial bolus of 80 U/kg, followed by an initial infusion rate of 18 U/kg per h in patients with normal liver function. Heparin also has pleiotropic effects that may decrease systemic and local inflammation.
Low-Molecular-Weight Heparins No monitoring or dose adjustment is needed unless the patient is markedly obese or has chronic kidney disease.
Fondaparinux, : an anti-Xa pentasaccharide, is administered as a weight-based oncedaily subcutaneous injection No laboratory monitoring is required. Fondaparinux is synthesized in a laboratory and, unlike LMWH or UFH, is not derived from animal products. It does not cause heparin-induced thrombocytopenia. dose must be adjusted downward for patients with renal dysfunction.
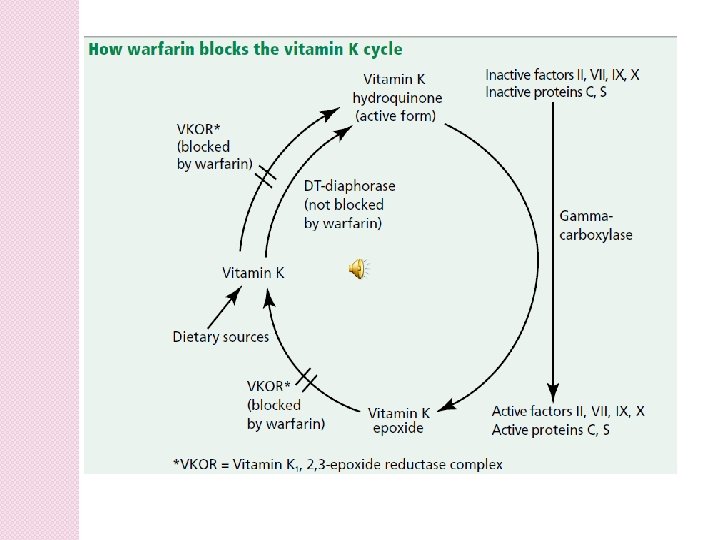
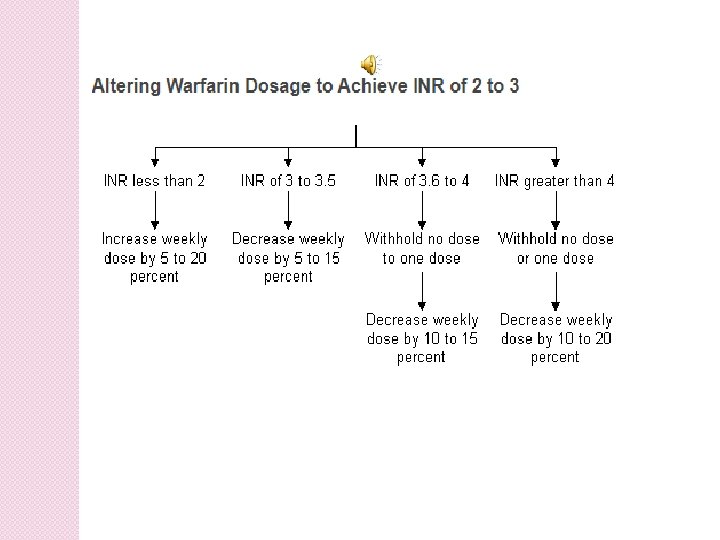
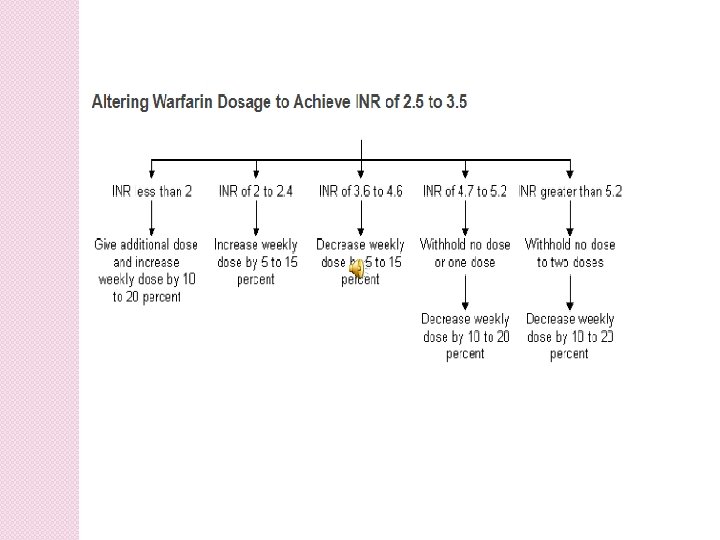
Warfarin This vitamin K antagonist prevents carboxylation activation of coagulation factors II, VII, IX, and X. Warfarin dosing In an average-size adult, warfarin is often initiated in a dose of 5 mg. The target INR is usually 2. 5, with a range of 2. 0– 3. 0.
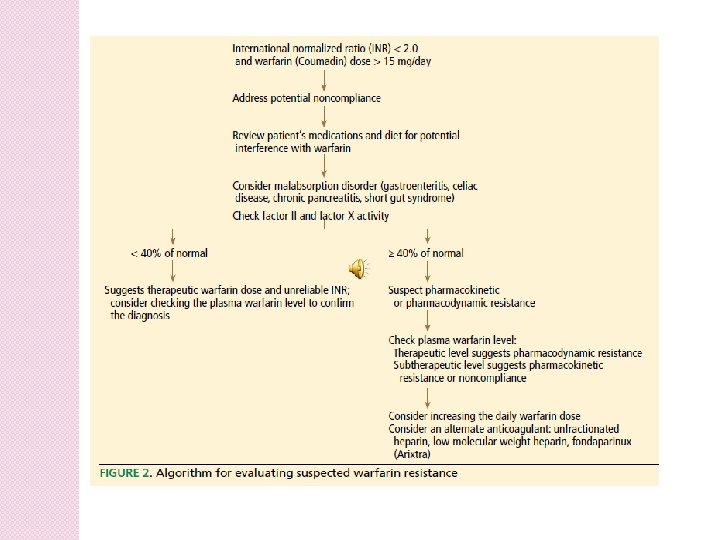
Resistance to warfarin has been described as the inability to prolong the prothrombin time or raise the international normalized ratio (INR) into therapeutic range when the drug is given at normally prescribed doses. However, a higher warfarin requirement does not itself establish the diagnosis of warfarin resistance. Patients who need more than 105 mg per week (15 mg/day) should be considered warfarin- resistant.
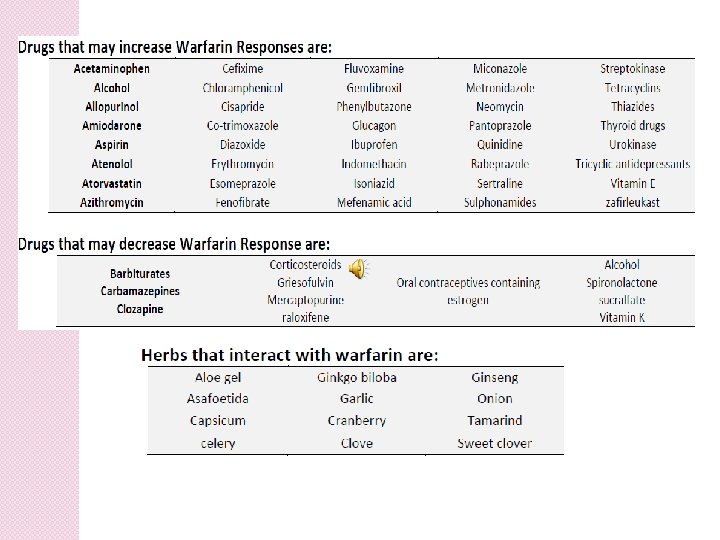
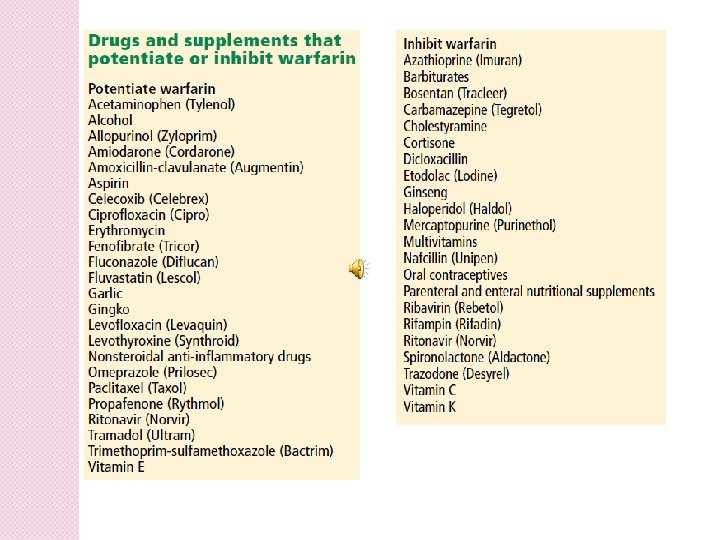
Causes of Warfarin Resistance: Acquired resistance 1. Poor patient compliance 2. High consumption of vitamin K 3. Decreased absorption of warfarin: 4. Increased clearance 5. Drug interactions
Hereditary resistance: has been postulated to be caused by genetic factors that result either in faster metabolism of the drug (a form of pharmacokinetic resistance) or in lower activity of the drug (pharmacodynamic resistance). Polymorphisms may play a role, as some VKORC 1 and CYP 2 C 9 variant alleles are known to be associated with increased sensitivity to warfarin.
Pharmacokinetic resistance: Genetic factors Hypoalbuminemia Hyperlipidemia. Diuretics
Pharmacodynamic resistance • Increased affinity of vitamin K, 2, 3 epoxide reductase complex (VKOR) for vitamin K • Prolongation of normal clotting factor activity • Production of clotting factors that is not dependent on vitamin K • Decreased VKOR sensitivity to warfarin.
Increasing age and systemic illness reduce the required warfarin dose. CYP 2 C 9 Variant alleles impair the hydroxylation of S-warfarin, thereby lowering the dose requirement. Variants in the gene encoding the vitamin K epoxide reductase complex 1 (VKORC 1) can predict whether patients require low, moderate, or high warfarin doses. However, genetic testing is not used clinically to dose patients with warfarin.
Warfarin cause major hemorrhage, including intracranial hemorrhage, even when the INR remains within the desired therapeutic range. Warfarin cause “off target” side effects such as alopecia or arterial vascular calcification. Some patients complain that warfarin makes them feel cold or fatigued.
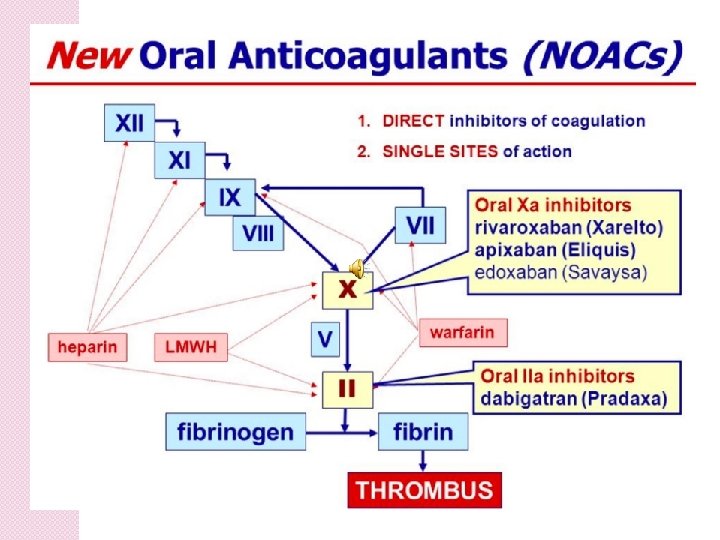
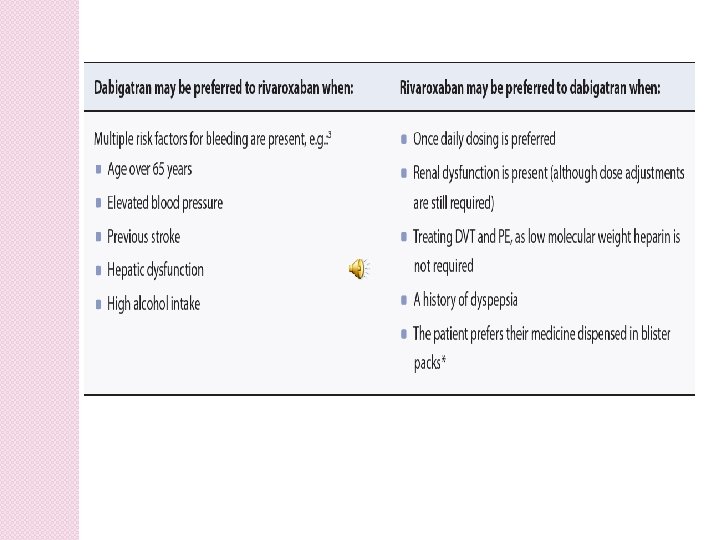
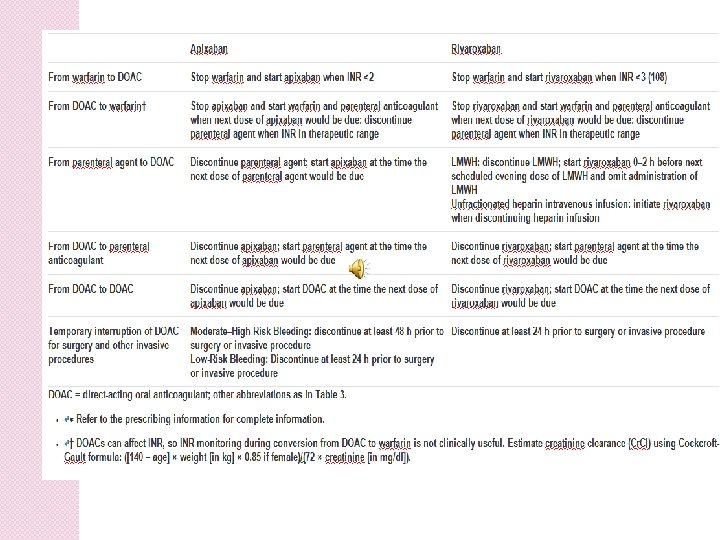
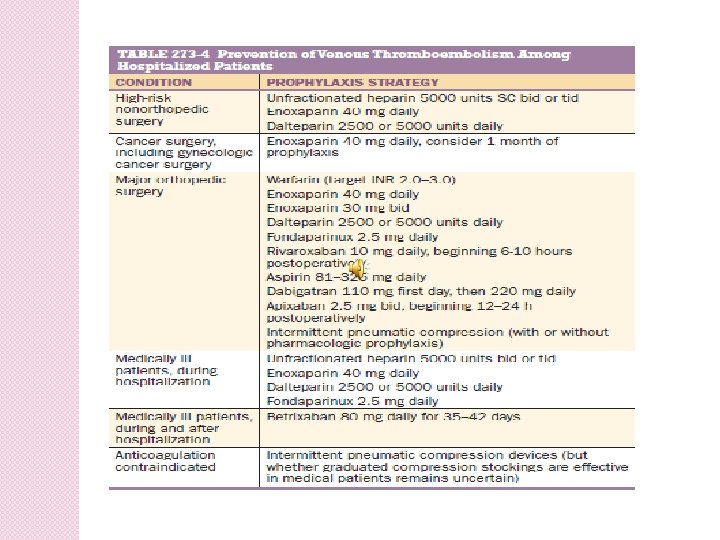
Novel Oral Anticoagulants: Novel oral anticoagulants (NOACs) are administered in a fixed dose, establish effective anticoagulation within hours of ingestion, require no laboratory coagulation monitoring, and have few of the drug-drug or drug-food interactions.
Complications of Anticoagulants: The most serious adverse effect of anticoagulation is hemorrhage. For life-threatening or intracranial hemorrhage due to heparin or LMWH, protamine sulfate can be administered.
Heparin Neutralization 1 -1. 5 mg per 100 USP units of heparin; not to exceed 50 mg Monitor APTT 5 -15 min after dose then in 2 -8 hr In setting without bleeding complications, consider observation
Dose of protamine (mg) to neutralize 100 units of heparin <1/2 hr: 1 -1. 5 mg/100 units of heparin 30 -120 min: 0. 5 -0. 75 mg/100 units of heparin >2 hr: 0. 25 -0. 375 mg/100 units of heparin
Dalteparin or Tinzaparin Overdose 1 mg protamine for 100 units dalteparin or tinzaparin; if PTT prolonged 4 hr after protamine overdose administer 0. 5 mg per 100 units of dalteparin or tinzaparin
Enoxaparin Overdose 1 mg per mg enoxaparin (if enoxaparin overdose given within 8 hr); if >8 hr of overdose or bleeding continues after 4 hr after first dose, give 0. 5 mg protamine per mg enoxaparin
There is no specific reversal agent for bleeding caused by fondaparinux or factor Xa inhibitors. However, the dabigatran antibody, idarucizumab, is an effective and rapidly acting antidote for dabigatran that is now licensed for use. Andexanet is a universal anti-Xa antidote for betrixaban, rivaroxaban, apixaban, and edoxaban that is undergoing review by the FDA.
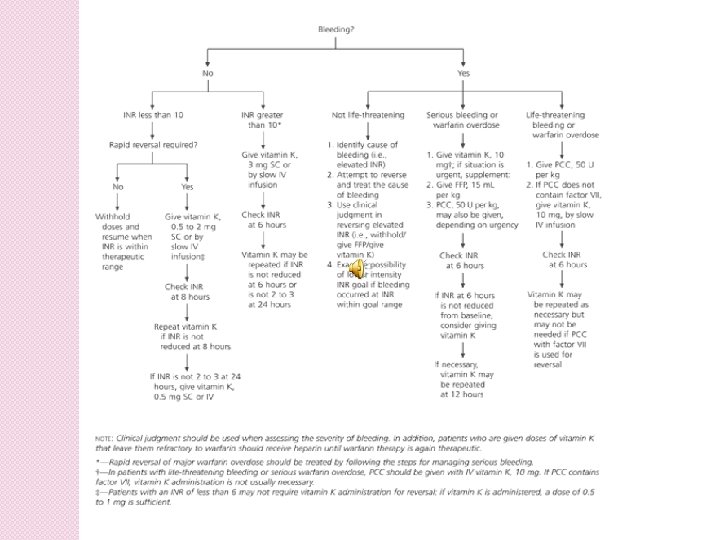
Major bleeding from warfarin is best managed with prothrombin complex concentrate(PCC). With less serious bleeding, fresh-frozen plasma or intravenous vitamin K can be used. Oral vitamin K is effective for managing minor bleeding or an excessively high INR in the absence of bleeding.
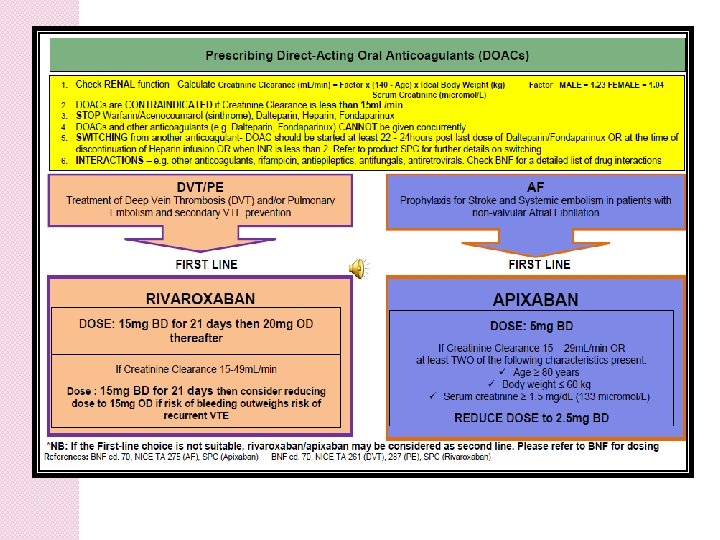
Rivaroxaban is contraindicated in patients who: Are actively bleeding or have a high risk of major bleeding Have a prosthetic heart valve Have moderate to severe hepatic dysfunction associated with coagulopathy Have renal dysfunction with a creatinine clearance (Cr. Cl) < 30 m. L/min
Rivaroxaban dosing as determined by renal function
Duration of Anticoagulation: For DVT isolated to an upper extremity or calf that has been provoked 3 months of anticoagulation usually suffice. For an initial episode of provoked proximal leg DVT or PTE, 3– 6 months of anticoagulation used to be the classic teaching.
For patients with cancer and VTE, prescribe LMWH as monotherapy VTE that occurs during long-haul air travel is considered unprovoked. Counterintuitively, the presence of genetic mutations such as heterozygous factor V Leiden and prothrombin gene mutation does not appear to increase the risk of recurrent VTE.
INFERIOR VENA CAVA FILTERS The two principal indications for insertion of an IVC filter are (1)active bleeding that precludes anticoagulation (2) recurrent venous thrombosis despite intensive anticoagulation.
MANAGEMENT OF MASSIVE PTE For patients with massive PE and hypotension, replete volume with 500 m. L of normal saline. Dopamine and dobutamine are first-line inotropic agents for treatment of PErelated shock. FIBRINOLYSIS
Successful fibrinolytic therapy rapidly reverses right heart failure and may result in a lower rate of death and recurrent PE by (1) dissolving much of the anatomically obstructing pulmonary arterial thrombus, (2) preventing the continued release of serotonin and other neurohumoral factors that exacerbate pulmonary hypertension, (3) lysing much of the source of the thrombus in the pelvicor deep leg veins, thereby decreasing the likelihood of recurrent PE.
The preferred systemically administered fibrinolytic regimen is 100 mg of recombinant tissue plasminogen activator (t. PA) prescribed as a continuous peripheral intravenous infusion over 2 h. The sooner thrombolysis is administered, the more effective it is. However, this approach can be used for at least 14 days after the PE has occurred.
Contraindications to fibrinolysis include intracranial disease, recent surgery, and trauma. The overall major bleeding rate is about 10%, including a 2– 3% risk of intracranial hemorrhage.
PHARMACOMECHANICAL CATHETERDIRECTED THERAPY The dose of alteplase can be markedly reduced, usually to a range of 20– 25 mg, instead of the peripheral intravenous systemic dose of 100 mg. PULMONARY EMBOLECTOMY PULMONARY THROMBOENDARTERECTOMY EMOTIONAL SUPPORT
Rivaroxaban: a fully-subsidised oral anticoagulant www. bpac. org. n z June 2018 1
Thanks for Your Attention E. Mail: Shafiepour. mohsen@yahoo. co m