Dysnatremic Disorders Hyponatremia and Hypernatremia Mohamed Osama Ezwaie

; key facts/ concepts Regulation of water balance Renal")


 Sensor Stimulus Effector Osmoreceptors; hypothalamus Plasma hypo/ hyperosmolality")




![Key calculations in electrolytes disorders Serum OSM ( cal) = [ Na] × 2+](https://slidetodoc.com/presentation_image/298ef9956fba24f45c156d2135564376/image-14.jpg "Key calculations in electrolytes disorders Serum OSM ( cal) = [ Na] × 2+")
 Hyponatremia; defined as a serum sodium conc.")






![Hyponatremia [ Na] <130 m. Eq/L p. Osm >295 m. Osm/kg Translocational Defect in](https://slidetodoc.com/presentation_image/298ef9956fba24f45c156d2135564376/image-24.jpg "Hyponatremia [ Na] <130 m. Eq/L p. Osm >295 m. Osm/kg Translocational Defect in")





 Viral pneumonia Duodenum")



, proved for therapy of")





 Moderate: 150")

 Water deficit ( Liters) Estimate TBW: 50 -60% of body")






- Slides: 52
Dysnatremic Disorders; Hyponatremia and Hypernatremia Mohamed Osama Ezwaie, MD Associate professor of medicine and nephrology
Learning objectives Water homeostasis ( balance); key facts/ concepts Regulation of water balance Renal water handling Hyponatremia: Types Etiology & SIADH Diagnostic approach Management; general & directed therapy Hypernatremia: Etiology & diagnosis Therapy / correction
Water balance
Basic principles Facts/ concepts in nephrology to realize; Control of ECF volume is dependent on regulation of sodium balance (intake and excretion), clinically manifested as: Hypovolemia/ hypotension Hypervolemia-edema/ hypertension ECF volume disorder Control of sodium concentration is dependent on regulation of water balance, clinically manifest as: Hyopnatremia Hypernatremia ECF / ICF osmolality disorder
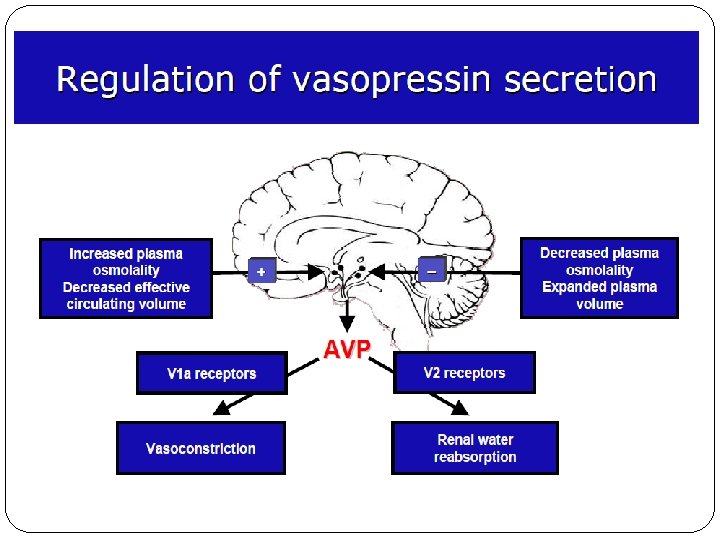
Regulators of water balance (sodium concentration) Sensor Stimulus Effector Osmoreceptors; hypothalamus Plasma hypo/ hyperosmolality Osmotic release of ADH; increase expression and affinity of aquaporin receptors at collecting ducts Baroreceptors (intravascular arterial receptors) - Low pressure; atria - High pressure; carotids and aortic arch Hypovolemia Non-osmotic release of ADH Balance effect Water retention or excretion
Discovery of Aquaporins-AQP 1 Peter Agre & Roderick Mac. Kinnon Nobel Prize---10 December 2003
Renal regulation of sodium and water balance Kidneys regulate sodium balance differently from regulation of water balance: JGA (RAAS), and tubular handling for sodium balance Aquaporins of CD and medullary tonicity for water balance Daily intake of sodium varies from 100 -150 m. Eq ( 4 -6 g of Na. Cl) Kidneys capacity for sodium handling is quite flexible. In normal person, they maintain sodium balance without edema, hypertension, or hypotension across a broad range of sodium intake ( 10 -1000 m. Eq per day)
sodium
Basic principles Serum osmolality: determined by total solutes concentration in fluid, and is equal in all fluid compartments Vs. specific gravity a measure of molecular weight of solutes Serum tonicity: ability of combined effect of all solutes to generate an osmotic driving force that causes water movement from one compartment to another
Key calculations in electrolytes disorders Serum OSM ( cal) = [ Na] × 2+ [glucose] /18+ [BUN] /2. 8 (OSM = 280 -295 m. Osm/ kg H 2 O) Osmolal gap = measured OSM – calculated OSM (Osmolal gap < 10 m. Osm)
Disorders of osmolality/ tonicity ( hypo/ hypernatremia) Hyponatremia; defined as a serum sodium conc. < 135 m. Eq/L Hospital incidence variable 15 -20% of patients Hypernatremia; defined as a serum sodium conc. > 145 m. Eq/L [serum Na] = ECF Na / ECF H 2 O
Hyponatremia
Sodium balance Chief extracellular cation Normal range: 135 -145 m. Eq/L Total body volume Na conc. estimated at 40 m. Eq/L 1/3 fixed to bone, remaining 2/3 predominantly in ECF ready for transmembrane exchange with ICF For every 3. 5 m. Eq the Na is over 140, there is an estimated free water deficit of 1 L. Na+
Hyponatremia; severity Mild 130 -135 m. Eq/l Moderate 125 -130 m. Eq/l ( may not symptomatic if chronic) Sever < 125 m. Eq/l (usually symptomatic) High mortality; may reach 50%
Hyponatremia; types Pseudo-hyponatremia; Normal serum osmolality Lab. artifact: reduced aqueous fraction < 93% Hyperlipidemia, hyperparaproteinemia, Immunoglobulin infusion Translocational ( dilutional) hyponatremia; High serum osmolality Shift of water out of cells to ECF, due non-sodium stimuli Hyperglycemia*, mannitol, sorbitol, glycerol, glycine infusions, radiocontrast agents For each 100 mg% of glucose above its normal range, serum sodium must be increased by 1. 6 m. Eq/L
Hyponatremia; types Pseudo-hyponatremia; Normal serum osmolality Lab. artifact: reduced aqueous fraction < 93% Hyperlipidemia, hyperparaproteinemia, Immunoglobulin infusion Translocational ( dilutional) hyponatremia; High serum osmolality Shift of water out of cells to ECF, due non-sodium stimuli Hyperglycemia*, mannitol, sorbitol, glycerol, glycine infusions, radiocontrast agents For each 100 mg% of glucose above its normal range, serum sodium must be increased by 1. 6 m. Eq/L
True hyponatremia Low serum osmolality Viewed as defect in water balance; Excess water intake or Defect in renal handling/regulation; which includes defect s in Glomerular filtration, or in diluting segment of renal tubules or Defect in ADH (AVP) release or response ( reduced free water excretion)
Hyponatremia [ Na] <130 m. Eq/L p. Osm >295 m. Osm/kg Translocational Defect in urinary diluting mechanisms , relatively concentrating urine or ( ADH PROBLEM) p. Osm< 280 m. Osm/kg (True hyponatremia) Uosm >100 m. Osm/kg Uosm <100 m. Osm/kg Patients with normal renal function, but exceeding max. Urinary Na ? Psychogenic polydipsia, water intoxication, hypotonic fluid infusion, beer botmania ( low salt content), defect in thirst center (rare), or Hyponatremia in process of correction urine diluting capacity ( 50 m. Osm/kg)
Defect in urinary dilution or ADH secretion Hyponatremia [Na} <130 m. Eq/L p. Osm< 280 m. Osm/kg Uosm >100 m. Osm/kg Coupled with Reduced / Blocked Na excretion Urinary Na < 30 m. Eq/L Urinary Na >30 m. Eq/L Edema or ascites Signs of ECF volume contraction No signs of ECF volume contraction Hypervolemic hyponatremia Extra-renal hypovolemic hyponatremia Renal hypovolemic hyponatremia Euvolemic hyponatremia Coupled with normal or increased urinary Na excretion
Hyponatremia [Na} <130 m. Eq/L p. Osm< 280 m. Osm/kg Uosm >100 m. Osm/kg Urinary Na Blocked Na excretion Urinary Na >30 m. Eq/L < 30 m. Eq/L Edema or ascites Signs of ECF volume contraction Hypervolemic hyponatremia Extra-renal hypovolemic hyponatremia Liver cirrhosis No signs of ECF volume contraction Renal hypovolemic hyponatremia Euvolemic hyponatremia Salt wasting nephropathy CCF Advanced renal disease Nephrotic syndrome Signs of ECF volume contraction Diarrhea Vomiting Mineralocorticoid def. Diuretics ACE inhibitors SIADH Hypothyroidism Coupled with normal or increased urinary Na excretion
Hyponatremia; diagnostic approach What is apparent ECF volume status ? ; Hypovolemia, euvolemia, hypervolemia Monitor patient, B. P& urine output ( determine fluid balance) Body weight ( to calculate TBW) What is serum osmolality ? ; Pseudohyponatremia Translocational hyponatremia True Hyponatremia What is urine osmolality and sodium ? Severity of and chronicity hyponatremia Workup of underlying cause SIADH Psychogenic polydipsia Hypothyroidism drugs
SIADH pathophysiological definition Hyponatremic disorder characterized by reduced ability of the kidneys to dilute urine despite serum hypotonicity Implies; ADH release in absence of two major stimuli: Increased serum osmolality Decreased EABV
SIADH State of mild volume expansion results; Urinary sodium wasting Clinically undetectable decrease in total body sodium Overall disturbances; Hyponatremia Low serum osmolality < 280 m. Osm/kg Inappropriately concentrated urine Increased urinary sodium > 30 m. Eq/L Patient must be clinically euvolemic, no evidence of thyroid, adrenal or renal disease, and taking diuretics or drugs that stimulate AVP release or action.
Conditions associated with SIADH Carcinomas Pulmonary diseases Lung ( small cell) Viral pneumonia Duodenum Pulmonary abscess pancreas Tubeculosis aspergillosis CNS disorders Encephalitis Meningitis Stroke Tumor Head trauma
Drugs result in SIADH Stimulate release of AVP Nicotine Clofibrate Vincristine Antidepressants antipsychotics Other mechanism Chloropropamide Tolbutamide Cyclophosphamide Barbiturates Carbamazipine NSAID
Correction of Sodium Deficit Example: A 60 kg woman with a plasma sodium concentration of 120 m. Eq/L: Sodium deficit = TBW x (130 – [Na+]p) Sodium deficit = 0. 5 x 60 x (130 -120) = 300 m. Eq 3% Na. Cl contains 513 m. Eq sodium/L Volume of 3% Na. Cl needed = 300/513 = 585 m. L Infusion rate: Should be at 0. 5 m. Eq/L/hr A correction of 10 m. Eq should be done over 20 hours So, 585 m. L/20 hours = 29 m. L/hour of 3% Na. Cl
Treatment of euvolemic hyponatremia In SIADH; Giving loop diuretics ( 1 mg/ Kg I. V 6 -12 hourly) will result in excretion of at least isotonic urine ( isothenuria 290 mosm/ L), because it enhances free water excretion This method achieve maximal net free water loss of about 0. 5 liter/ hour with concomitant rise in plasma sodium conc. of 1. 5 m. Eq/ L If cause not reversible; Na Cl salt tablet, demeclocycline 600 mg/ day, or lithium can be used Currently introduced the V 2 receptor antagonists; Vaptans
Treatment of euvolemic hyponatremia Vaptans: V 2 receptor antagonists (acquaretics), proved for therapy of euvolemic and hypervolumic hyponatremia Enhance water reabsorption in the collecting ducts, antagonizing effect of ADH Increasing free water excretion without causing electrolyte disturbance ( Vs. diuretics)
Treatment of euvolemic hyponatremia Vaptans: Tolvaptan; 15 -30 mg tablets O. D, Conivaptan parentral They reverse hyponatremia, increasing P. Na by 6 -7 m. Eq/L Dose not require water restriction unless patient is hypervolemic Caution for use in patients with chronic liver disease
Treatment of hypovolemic hyponatremia; Discontinue diuretics Replace volume deficit or on going fluid loss, usually as isotonic saline treat cause for volume deficit
Treatment of hypervolemic hyponatremia; water restriction and loop diuretics mainstay of therapy Isotonic saline used if sever hyponatremia
Hypernatremia
Hypernatremia Almost always result of combined water and volume deficit, with losses of water in excess of salt Associated with cellular dehydration ( Vs. hyponatremia) It is advisable to correct water deficit slowly to avoid neurological complications, especially if chronic one
Hyponatremia; clinical evaluation Severity: Mild: 145 -149 m. Eq/L (usually asymptomatic ) Moderate: 150 -169 m. Eq/L Sever ( profound ): > 170 m. Eq/L Clinical features; signs of intracellular dehydration and neurological dysfunction: Lethargy Irritability Skin feels "doughy" Ataxia, tremor Hyperreflexia, Seizures, reduced GCS
Hypernatremia; diagnosis Plasma osmolality Urine osmolality TBW estimation Screening for osmotic solutes in blood ( glucose) Water challenge test ( D. I); with monitering of response of P. osmolality and urine osmolality Pituitary hypothalamic axis evaluation and imaging ( MRI)
Hypernatremia; Treatment ( correction) Water deficit ( Liters) Estimate TBW: 50 -60% of body weight 2. Calculate free-water deficit: [(Na- 140)/ 140] x TBW 3. Adminster over 48 hours 1. On going water losses (liters) Calculate free-water clearance from urinary flow rate ( V) and urine ( U) Na and K concentrations: V- V x ( UNa +Uk)/ 140 Insensible losses ( liters) 10 ml/kg per day: less if ventilated, more if febrile Total: As free water replacement ( D/W 5%), adminstration rate 50 -250 ml/ hour
Hypernatremia; Treatment Aim to lower the serum sodium slowly at a rate of no more than 12 mmol/L in 24 hours, (0. 5 m. Eq/L/hour) An even slower rate will be required for patients with chronic hypernatremia Carefully regulate fluid intake - do not allow excessive intake in a thirsty patient If the serum sodium falls too rapidly (>0. 5 mmol/L/hr) slow the rate of rehydration (for example, by 20%) Check U&E's and glucose hourly intially, then 2 -4 hours
Hypernatremia; Treatment Patients with central diabetes insipidus may respond well to intranasal adminstration of desmopressin. Patients with nephrogenic diabetes insipidus, may reduce their polyuria by drugs that decrease free water excretion ( i. e, urine dilution) as hydrochlorthiazide or amiloride
q Simon Steddon, Neil Ashman. Handbook of nephrology and hypertension, 2 nd edition, 2014, oxford university press. q Maxime papadakis, Stephen Mcphee. Current medical diagnosis and treatment. 55 th edition, 2016, Mc. Graw Hill. q Brian Walker, Nicki Colledge, et al. Davidson’s principles and practice of medicine. , . 22 nd edition, 2014. Churchill Livingstone Elsevier q Parveen Kumar, Michael Clark. Kumar and Clark’s clinical medicine, 8 th edition, 2012. Saunders Elsevier press.
Exercises A patient with renal failure has the following chemistries: Sodium 130 m. Eq/ L Glucose 100 mg% BUN 120 mg% Calculate the serum osmolality? Would you expect this osmolality to be associated with increased thirst? Answer is: 308 m. Osm/L This patient ECF is not hypertonic, thirst is not stimulated
Exercises A 53 non-diabetic patient presents with confusion, pedal edema, rales, and third heart sound ( S 3), his serum [ Na ] is 122 m. Eq/ L confirmed in two lab. assays , dose he has problem with sodium regulation, water regulation, or both? Answer is: Expanded ECF volume; increased sodium content True symptomatic hyponatremia This patient has combined sodium and water disturbances; CCF with salt and water retention, and impaired ability of the his kidneys to excrete dilute urine ( free water) Ideally treatment; salt restriction and loop diuretic to reduce ECF volume expansion, Water restriction to prevent further hyponatremia