VTE COMPLICATIONS OF COVID 19 Dr Chris Owoo









 describes two important conditions associated with venous")





















, Algeria")























- Slides: 58
VTE COMPLICATIONS OF COVID -19 Dr. Chris Owoo Anaesthesia & Critical Care University of Ghana Med School/ Korle Bu Teaching Hospital Accra, Ghana
Disclosures • NIL
Outline • VTE before COVID-19 • VTE Safe Zone Hospital Project – The Ghanaian Experience • COVID-19 arrives • Statistics and Burden of COVID-19 • VTE complications and pathophysiology in COVID-19 • Strategies and Recommendation • Conclusions • Acknowledgements
Ga East Municipal Hospital ICU
UGMC ICU
UGMC ICU
UGMC ICU MONITORING ROOM
BEFORE THE ARRIVAL OF COVID-19……………. .
VTE is a Major Public Health Problem!!! • VTE: Widespread and associated with significant mortality • Annually, 1. 5 million VTE events occur in the European Union¹ and 900 000 in the United States² • Globally, more than 500000 deaths per year are due to complications related to VTE 3; more than the number of deaths associated with AIDS, breast cancer and road traffic accidents combined 2 -3 • Responsible for 5 -10% of mortality among hospitalized adults • Many of these are sudden and from undetected disease 3 9
Background on VTE • Venous thromboembolism (VTE) describes two important conditions associated with venous thrombosis: Deep vein thrombosis (DVT) and Pulmonary embolism (PE) With permission of Pr Kakkar Pulmonary embolism is a potentially life-threatening complication of DVT but could also occur spontaneously 10
Aetiopathogenesis of HA-VTE • Hospitalized patients are exposed to multiple risks factors to increase the risk of HA-VTE • These risk factors fall into 3 major categories that positively predicts increase profile of risk and have been used by many RAMs to predict risk of VTE • The Virchow’s Triad • Hypercoagulability • Circulatory Stasis • Vascular Endothelial Injury
Assess Risk: VTE Prevention is a Strategy to Address a Challenging Silent Disease • VTE is often undiagnosed because of its silent nature • The first manifestation of VTE may be fatal PE 1 • An estimated 10% of hospital deaths may be due to PE 2, 3 With the permission of Dr MA Sevestre, Amiens University Hospital, France. • More than 90% of patients dying from fatal VTE events were never diagnosed or treated 2, 3 • Expert guidelines recommend VTE Prevention • PE is the leading cause of preventable death in hospitalized patients and prophylaxis is the number 1 strategy for improving patient safety in hospitals 1 1. Geerts WH. Chest. 2004; 126(suppl): 338 S-400 S. 2. Cohen AT. Haemostasis 1996; 26: 65 -71. 3. Sandler DA, et al. J R Soc Med 1989; 82(4): 203 -5. 12
VTE Safety Zone Hospital Project 13
Why Implement a VTE Safety Zone Program? • Together we can improve patients’ VTE safety in our hospital • The VTE Safety ZONE program is designed to: • Help hospitals and physicians improve quality of patient care through measurable reductions in DVT and PE. • Provides a comprehensive set of information and tools to assess and improve the prophylaxis of patients at risk of DVT in the hospital setting • Audit performance for VTE prevention and facilitate hospital accreditation 14
A Comprehensive approach to optimize VTE management 15
Expected outcomes of the VTE SZ program ● Improve the quality of care in your hospital through measurable reductions in DVT and PE. ● Improve the quality of life (QOL) of patients. ● Reduce the overall costs of care. ● Data generation for wider Healthcare community (Best practice sharing) 16
HOW? Evaluate Prophylaxis Practice BE AWARE Optimize Prophylaxis Practice BE PROACTIVE Optimize Prophylaxis Practice MEASURE IMPACT 17
18
Introducing and Implementing a VTE Safety ZONE Program • Introducing the VTE Safety ZONE Program • Identify an interdisciplinary team (physicians, nurses, administrators) to present the initiative and define implementation strategy • Incorporate routine risk assessment into forms and protocols • Establish program metrics 19
Introducing and Implementing a VTE Safety ZONE Program • Implementing the program • Provide training for key staff members • Use adapted materials from the VTE Safety ZONE package to drive change • Provide VTE Risk Assessment Sheets to HCP’s to easily identify patients at Risk for VTE. • Provide VTE Stickers to HCP’s to identify Patients who have been assessed or not and to know their risk status • For Patients at Risk, give Risk Assessment to treating Physicians and VTE Prophylaxis order for selection of appropriate VTE Prophylaxis modality 20
21
22
A Comprehensive approach to optimize VTE management 23
VTE SAFETY ZONE HOSPITAL PROJECT AN EFFECTIVE PATHWAY FOR THE MANAGEMENT OF THE RISK OF HA-VTE
THEN ON DECEMBER 31, 2019 ARRIVES ……. SARS-Co. V-2 VIRUS!!!
THE NEW VIRULENT KID ON THE BLOCK WITH THE “CROWN” OF DEATH
EPIDEMIOLOGY & BURDEN
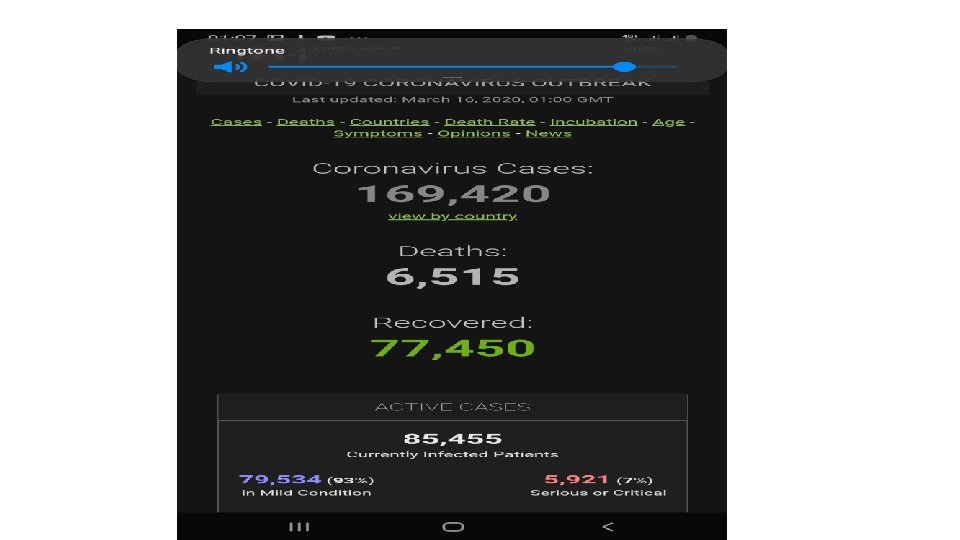
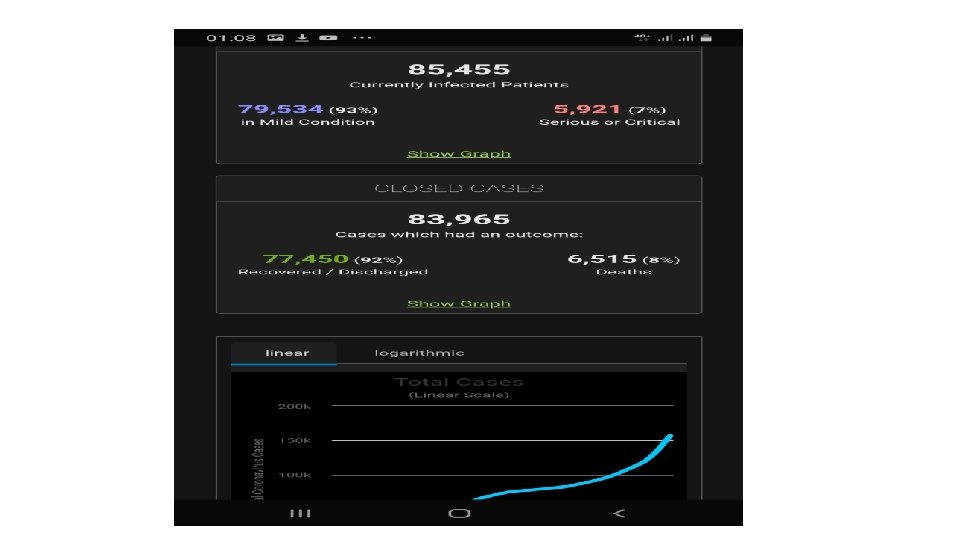
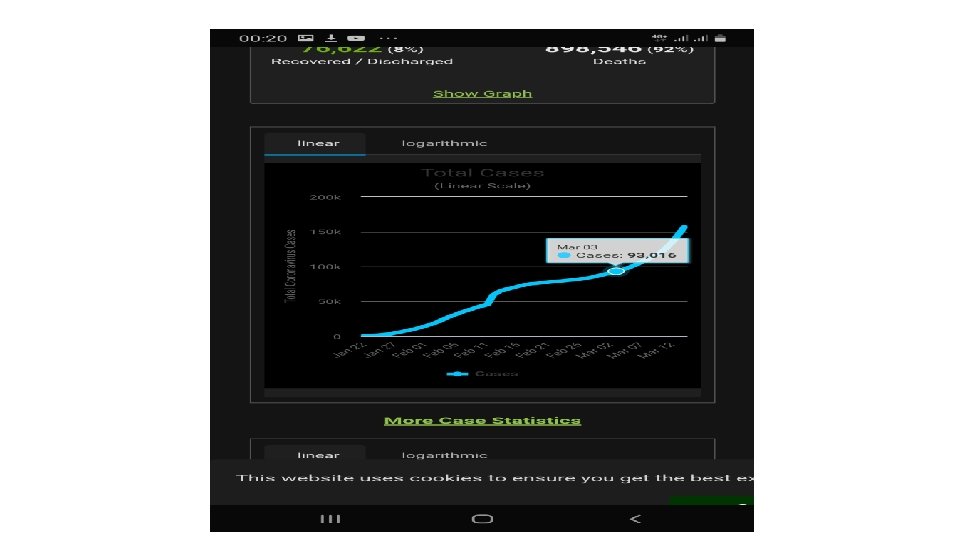
Global Statistics for COVID-19 As at 15/03/2020 As at 08/06/2020 • Coronavirus Cases: • 162, 651 • Deaths: • 6, 069 • Recovered: • 76, 219 • Coronavirus Cases: • 7, 188, 208 • Deaths: • 408, 229 • Recovered: • 3, 506, 728
Africa Update as at 15/03/2020 • Africa – 24 Countries • Egypt (110), Algeria (48), South Africa (51), Morocco (28), Senegal (24), Tunisia (18), Ghana (6), Cote D’ivoire (4), Burkina Faso (3), Cameroon (3), • DRC (2), Namibia (2), Nigeria (2), Seychelles (2), Equatorial Guinea (1), Ethiopia (1), Gabon (1), Guinea (1), Kenya (1), Mauritania (1) • Rwanda (1), Sudan (1), Swaziland (1) and Togo (1)
Africa Update as at 08/06/2020 • Africa – 57 Countries • South Africa (50, 879), Egypt (35, 444), Nigeria (12, 801), Algeria (10, 265), Ghana (9, 910), Morocco (8, 302), Cameroon (8, 060), Sudan (6, 242), Senegal (4, 427), Djibouti (4, 278) • Guinea (4, 216), DRC (4, 106), Cote D’ivoire (3, 881), Gabon(3, 101), Kenya (2, 872), Somalia (2, 368), Ethiopia (2, 156), Mayotte (2, 151), CAR (1, 850), South Sudan (1, 604) • Mali (1, 547), Guinea Bissau (1, 368), Equatorial Guinea (1, 306), Zambia (1, 200), Mauritania (1, 104), Madagascar (1, 094), Tunisia (1, 087), Sierra Leone (1, 001), Niger (973), Burkina Faso (890)
Disease Severity……………. In Africa: • The majority of people have uncomplicated or mild illness (90 - 95%) – requiring isolation at home, isolation centre or hospital • Approximately 5 -10% develop severe disease that requires hospitalization and oxygen support, and • 2 -5% require admission to an intensive care unit or high dependency/ care unit for treatment • Of those critically ill, many will require mechanical ventilation or NIV modalities. • The most common diagnosis in severe covid-19 patients is severe pneumonia. • Older age and co-morbid disease have been reported as risk factors for death
VTE Complications of COVID-19 • Coagulopathy in COVID-19 has a prothrombotic character, which may explain reports of thromboembolic complications. • Predisposition to venous VTE due to the direct effects of COVID-19, or the indirect effects of isolation or illness severity (e. g. , severe inflammatory response, critical illness, traditional risk factors). • Incidence of VTE of 20% to 86% of patients with severe COVID-19 (including some patients who were on thromboprophylaxis), and may be associated with poor prognosis. • Patients with very high D-dimer levels have the greatest risk of thrombosis as well as poor disease prognosis from COVID-19
VTE-Related Pathophysiology • It has been hypothesised that the pathophysiology of PE in COVID-19 is different. • It is thought that local thrombi are formed in the lung vessels due to a local inflammatory process rather than the classical emboli coming from elsewhere in the body. • It has been suggested that a new term (e. g. , COVID-19 -associated pulmonary thrombosis, diffuse pulmonary intravascular coagulopathy, or microvascular COVID-19 lung vessels obstructive thrombo-inflammatory syndrome [Micro. CLOTS]) be used rather than the term pulmonary embolism. • Cases of arterial thrombosis, cerebral venous thrombosis, and acute limb ischaemia secondary to thrombosis have been reported.
VENOUS THROMBOEMBOLISM + COVID-19 ILLNESS = EXAGGERATED VIRCHOW’S TRIAD = EXAGGERATED MORBIDITY & MORTALITY
So Do We Need A Different Strategy or Pathway For Management of VTE or VTE Risk?
NO! We Probably Need A Widening Of The Pathway That Works…………. . Probably An Exaggeration Of The VTE Safety Zone Hospital Project
Strategies for Management of HA-VTE or More Importantly – Risk of HA-VTE in COVID 19 & Recommendations
Should hospitalized COVID-19 confirmed or highly suspected patients receive VTE prophylaxis? • Pharmacologic VTE prophylaxis for all hospitalized non-pregnant patients with confirmed or highly suspected COVID-19, regardless of VTE risk assessment score, unless a contraindication exists (e. g. active bleeding, profound thrombocytopenia). • Pharmacologic VTE prophylaxis for all hospitalized pregnant patients with confirmed or highly suspected COVID-19 following guidance recently published by the RCOG. Close collaboration with obstetric and anesthesiology colleagues is recommended in the event of delivery and/or need for epidural anesthesia during hospitalization. • In patients with a contraindication to pharmacologic VTE prophylaxis – consistent application of intermittent pneumatic compression devices with regular re-assessment for conversion to pharmacologic prophylaxis. • In critically ill patients, it is reasonable to employ both pharmacologic and mechanical VTE prophylaxis (intermittent pneumatic compression devices) as long as no contraindication to either modality exists.
What intensity of VTE prophylaxis should patients with COVID‑ 19 receive? • For non-critically ill hospitalized patients – Normal intensity (standard dose) VTE prophylaxis as per existing societal guidelines. • For critically ill patients – increased (Intermediate intensity) doses of VTE prophylaxis (e. g. , enoxaparin 40 mg (0. 5 mg/kg) subcutaneous twice daily, UFH 7500 units subcutaneous three times daily, or low-intensity heparin infusion. • For pregnant patients – consultation with obstetrician and anaesthetist. Intermediate intensity doses in 3 rd trimester may be reasonable • Recommend against using biomarker thresholds, such as elevated D-dimer, as the sole reason to trigger escalations in anticoagulant dosing outside the setting of a clinical trial. • For patients that are improving and transferring out of the ICU to the medical ward, it is reasonable to deescalate to standard VTE prophylaxis dosing.
Should patients with confirmed COVID‑ 19 receive VTE prophylaxis after hospital discharge? • Extended VTE prophylaxis is not necessary for all patients with COVID 19 who are being discharged from the hospital. • A multidisciplinary discussion should occur at or near the time of discharge to determine if a patient has ongoing VTE risk factors, may benefit from extended posthospital VTE prophylaxis, and has ensured access to VTE prophylactic medications. • If post-discharge prophylaxis is deemed reasonable, use an adequately studied and/or approved agent such as betrixaban, or rivaroxaban, or enoxaparin
Should biomarkers, such as D‑dimer, be serially measured to trigger changes in care? • While D-dimer elevation and other biomarkers have been associated with worse outcomes in patients with COVID-19, it is unknown if intensification of anticoagulant therapy based on biomarker thresholds alone improves patient outcomes. • Based on current available evidence, recommend against daily monitoring of d-dimer for the purpose of guiding anticoagulant therapy. D-dimer measurement may be used as a marker of illness severity and prognosis. • Recommend against intensification of anticoagulant dosing based only on biomarkers, such as d-dimer. However, acutely worsening clinical status in conjunction with laboratory value changes, such as rising D-dimer, may necessitate further thromboembolic workup or empiric treatment. • Recommend providers and clinicians stay apprised of emerging evidence regarding biomarkers of thromboembolic risk and adjust practices accordingly.
Should thrombolytic therapy be used in patients with COVID‑ 19? Recommend against use of thrombolytics in patients with COVID-19 outside of a clinical trial setting unless there is another clinical indication for thrombolysis, such as ST elevation myocardial infarction, acute ischemic stroke, or high-risk (massive) PE with hemodynamic compromise
How should VTE prophylaxis be administered in pediatric patients with COVID‑ 19? • Suggest that pediatric patients admitted for COVID-19 who are moderately or severely ill be given VTE risk prophylaxis in accordance with existing institutional guidelines.
When should patients on chronic warfarin therapy be transitioned to a DOAC in the setting of the COVID‑ 19 pandemic? • Anticoagulation clinics should use standardized educational materials for their warfarin-treated patients about safety precautions when obtaining INR blood draws to reduce the risk of COVID-19 infection • Patients who would not be eligible for DOAC therapy prior to the COVID-19 pandemic should not be switched to DOAC therapy during the COVID-19 pandemic. This includes (but is not limited to) patients with mechanical heart valves, severe liver dysfunction, or combined renal dysfunction and/or drug-drug interactions that preclude safe DOAC use. • Patients taking chronic oral anticoagulant in the outpatient setting should be switched to shorter acting agents (e. g. , LMWH or UFH) when initially hospitalized for COVID-19 in case of clinical deterioration, changes in renal function, or need for invasive procedures.
How should we manage COVID-19 patients who experience recurrent clotting of access devices (e. g. , central venous catheters, arterial lines) or extracorporeal circuits (e. g. ECMO) despite prophylactic anticoagulation? • Although of unproven benefit, it may be reasonable to increase the intensity of anticoagulation (i. e. , from standard-intensity prophylaxis to intermediate-intensity prophylaxis or from intermediate-intensity prophylaxis to therapeutic-intensity) or switch anticoagulants in these settings. • Any decision to increase the intensity of anticoagulation should take into account the individual patient’s bleeding risk.
Conclusions • Hospitalized COVID-19 patients are at greater risk of HA-VTE both from the pathophysiology of the disease and the clinical and IPC measures to manage these patients • The more severe the illness, the greater the risk • Hospital morbidity and mortality are greater than for their non-COVID -19 counterparts • Effective strategies for prevention and management of VTE risk and VTE are still very relevant but require the incorperation of other considerations • Awareness + Regular Risk Assessment + Appropriate Thromboprophylaxis are still the Key to prevention of HA-VTE in COVID-19 pandemic
A Comprehensive approach to optimize VTE management 53
Acknowledgement • Geoffrey D. , et al. Thromboembolism and anticoagulant therapy during the COVID‑ 19 pandemic: interim clinical guidance from the anticoagulation forum • COVID-19 and VTE/Anticoagulation: Frequently Asked Questions (Version 3. 0; last updated May 18, 2020) Input from Drs. Lisa Baumann Kreuziger, Agnes Lee, David Garcia, Adam Cuker, Mary Cushman, Maria De. Sancho
Ga East Municipal Hospital ICU
GEMH
UGMC ICU MONITORING ROOM
Thank You All