COMPLICATIONS OF FRACTURES Local complications can be divided

COMPLICATIONS OF FRACTURES Local complications can be divided into early (those that arise during the first few weeksfollowing injury) and late. Done by ala’a khresat& Marah Saeed

• Either Generalize or local complications. • Early or late complications. • Early and generalized complications >> shock (inadequate tissue perfusion)>> multi organ failure • ( hypovolemic shock > pelvic fracture which is single bone fracture that lead to bleed to death, bleeding from fracture site and plexus in pelvic , could die at site of accident, m. c (open book >> open of symphysis , or vertical shear ) >> treated by stabilize the pelvic and try to close the pelvic by c-Clamp >> decrease bleeding and decrease space of bleeding by increase pressure inside. • neuorogenic shock • Management of shock >> blood [ fresh frozen plasma, whole blood] , fluid ( normal saline)
 embolization >> fat , , from 1) medullary canal of bone")
• 2) embolization >> fat , , from 1) medullary canal of bone 2)from soft tissue 3) circulating fat >> trauma > inflammatory reaction >> globalization of fat >> block blood vessels. • Unique about fat embolism not close large blood vessels > to peripheral circulation >> no exchanges (there is oxygen but no blood circulation) • To develop need 24 -48 h , takes time • To prevent it by early fixation • Symptoms >> tachycardia , tachypneic , SOB , petechial rash in SVC distribution unconscious, sudden death , cor pulmonale , Rt. side HF • Clinical diagnosis , no specific diagnosis • First filter of fat embolism >> pulmonary tree , if it less than 100 microns >> might go to left side of heart and go any where of the body >> brain , kidney. • Treatment >> supportive( no specific treatment) >> , , oxygen, fluid management , pain management , , stabilization of fracture as much as possible. • Do chest X-ray >> ARDS like snow storm appearance
 DVT /PE and thromboembolism • Virchow triad >1) endothelial injury(Fracture and")
• 3) DVT /PE and thromboembolism • Virchow triad >1) endothelial injury(Fracture and trauma) 2) hypercoagulable state (tissue factor and thromboplastin and endothelial injury increased hypercoagulable state. • 3)stasis (immobilization) • >> hip surgery and hip fracture is one of the highest in thromboembolic diseases because of major vein around >> caused endothelial injury, hypercoagulable state and stasis. • So in hip surgery or fracture >> anti coagulant state for Long time (35 days) • Symptoms >> pain , swelling and fever • Diagnosis of DVT>> clinical, Doppler ultra sound • Treatment >> anti coagulation (therapeutic dose not prophylactic dose) and supportive treatment.

Early complications may present as part of the primary injury or may appear only after a few days or weeks. 1. visceral injury Fractures around the trunk are often complicated by injuries to underlying viscera, the most important being penetration of the lung with life-threatening pneumothorax following rib fractures and rupture of the bladder or urethra in pelvic fractures. These injuries require emergency treatment, before the fracture is dealt with. 2. vascular injury Fractures most often associated with damage to a major artery are those around the knee and elbow and those of the humeral and femoral shafts. The artery may be cut, torn, compressed or contused, either by the initial injury or subsequently by jagged bone fragments. Even if its outward appearance is normal, the intima may be detached and the vessel blocked by thrombus, or a segment of artery may be in spasm. The effects vary from transient diminution of blood flow to profound ischaemia, tissue death and peripheral gangrene.

Clinical features • The injured limb is cold and pale, or slightly cyanosed, and the pulse is weak or absent. • X-rays will probably show that the fracture is at one of the ‘high-risk’ sites mentioned above. If a vascular injury is suspected, urgent exploration to establish the diagnosis and restore circulation is mandatory. An angiogram is performed on the operating table if needed, but the damage is usually at the level of the fracture or joint dislocation anyway. Warm ischaemia times greater than 4– 6 hours can lead to limb loss.
 X-ray of a patient with a fractured femur and early signs")
Vascular injury (a) X-ray of a patient with a fractured femur and early signs of vascular insufficiency. The point of the proximal fragment seems to be dangerously close to the popliteal vessels. Angiography (b) shows that the artery is interrupted at precisely that point. (c) Despite vein grafting, the patient ended (a) (b) (c) up with peripheral gangrene.

Injuries associated with vascular trauma Injury Vessel First rib fracture. . . . . Subclavian artery Shoulder dislocation. . . . Axillary artery Humeral supracondylar fracture. . . Brachial artery Elbow dislocation. . . . . Brachial artery Pelvic fracture. . . . . Presacral and internal iliac vessels Femoral supracondylar fracture. . . Femoral artery Knee dislocation. . . . . Popliteal artery Proximal tibial fracture. . . . Popliteal artery or its branches

Treatment • All bandages and splints should be removed. • The fracture is re-x-rayed and, if the position of the bones suggests that the artery is being compressed or kinked, prompt reduction is necessary. • The circulation is then reassessed repeatedly over the next 30 minutes. If there is no improvement, the vessels must be explored by operation – preferably with the benefit of perioperative angiography. • An early temporary shunt across the damaged zone will restore the circulation promptly. If vessel repair is undertaken, stable fixation is imperative; where it is practicable, the fracture should be fixed internally.

• Early complications >> due to injury it’s self , injury of vessels and nerve • >> common site of vessels injury , around the knee and around the elbow • >> supracondylar Fracture of the elbow>> injury of brachial artery. • >> injury of artery >> compressed by bone it’s self, compressed by swelling of soft tissue , tear , vasospasm , intimal injury becomes like valve and close.

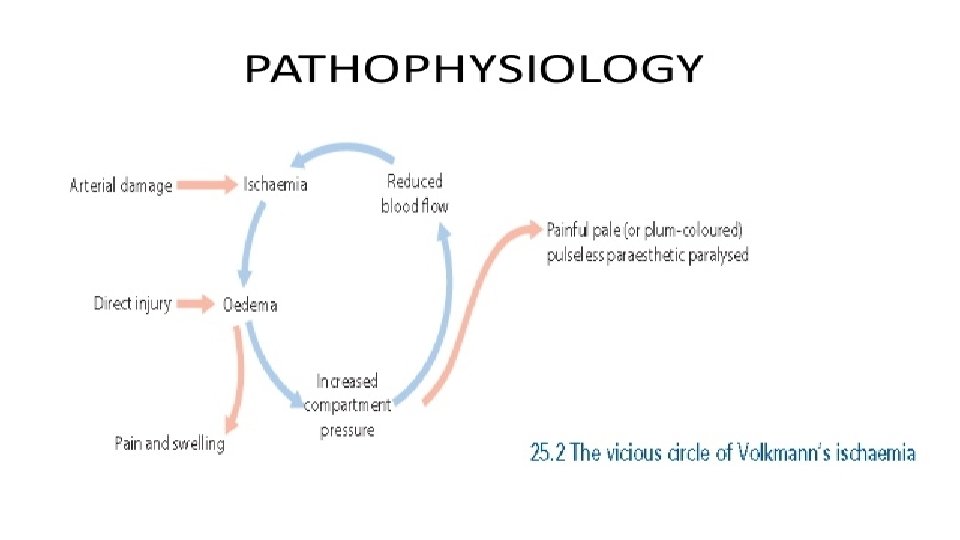
3. Compartment syndrome • Severe ischaemia even if there is no damage to a major vessel. • Bleeding, oedema or inflammation (infection) may increase the pressure within one of the osteofascial compartments; there is reduced capillary flow which results in muscle ischaemia, further oedema, still greater pressure and yet more profound ischaemia – a vicious circle that ends, after 12 hours or less, in necrosis of nerve and muscle within the compartment. • Nerve is capable of regeneration but muscle, once infarcted, can never recover and is replaced by inelastic fibrous tissue (Volkmann’s ischaemic contracture). • A similar cascade of events may be caused by swelling of a limb inside a tight plaster cast.

Clinical features High-risk injuries are fractures of the elbow, the forearm bones, the proximal one-third of the tibia and multiple fractures of the hand or foot. Other precipitating factors are operation (usually for internal fixation) or infection. Be aware that a compartment syndrome may also arise in a crush injury, a circumferential burn or even in a tight plaster cast. The classic features of ischaemia are the five Ps: Pain, Paraesthesia, Pallor, Paralysis and Pulselessness However, in a compartment syndrome the ischaemia occurs at the capillary level, so pulses may still be felt and the skin may not be pale! The earliest of the ‘classic’ features are pain (or a ‘bursting’ sensation), altered sensibility and paresis (or, more usually, weakness in active muscle contraction). Skin sensation should be carefully and repeatedly checked.

• Ischaemic muscle is highly sensitive to stretch, so when the toes or fingers are passively hyperextended, there is increased pain in the calf or forearm. • Confirmation of the diagnosis can be made by measuring the intracompartmental pressures; indeed, so important is the need for early diagnosis that some surgeons advocate the use of continuous compartment pressure monitoring for high-risk injuries and especially forearm or leg fractures in patients who are unconscious. • A differential pressure (ΔP) – the difference between the general diastolic pressure and the compartment pressure – of less than 30 mm. Hg is an indication for immediate compartment decompression.
 must be promptly decompressed. Casts, bandages and dressings")
Treatment The threatened compartment (or compartments) must be promptly decompressed. Casts, bandages and dressings must be completely removed limb should be nursed flat (elevating the limb causes a further decrease in end-capillary pressure and aggravates the muscle ischaemia). The ΔP should be carefully monitored; if it falls below 30 mm. Hg, immediate open fasciotomy is performed. ## In the case of the leg, ‘fasciotomy’ means opening all four compartments through medial and lateral incisions. The wounds should be left open and inspected 2 days later: if there is muscle necrosis, debridement can be done; if the tissues are healthy, the wound can be sutured (without tension), or skin grafted

If facilities for measuring compartmental pressures are not available, the decision to operate will have to be made on clinical grounds. If three or more of the ‘classical’ signs are present, the diagnosis is almost certain. If the signs are equivocal, the limb should be examined at 15 minute intervals and if there is no improvement within 2 hours of splitting the dressings, fasciotomy should be performed. Muscle will be dead after 4– 6 hours of total ischaemia there is no time to lose!
 A fracture at this level is always dangerous. This man")
Compartment syndrome (a, b) A fracture at this level is always dangerous. This man was treated in plaster; pain became intense and when the plaster was split (which should have been done immediately after its application), the leg was swollen and blistered. (c) Tibial compartment decompression is best done through two separate incisions and requires fasciotomies of all compartments (d). (A: anterior, P: peroneal, S: superficial posterior, D: deep posterior. )

• Local complications >> compartment syndrome • >> increase pressure within fascia beyond tissue perfusion. • Common site>> in leg • How many compartment in leg > 4 compartments(anterior compartment( extensor compartment) , lateral (peroneal compartment) , posterior deep and posterior superficial compartment>> gastrocnemius ) • >> due to trauma >> bleeding ( hematoma) or muscle contusion (swelling) or due to cast >> increase pressure in venous return >> increased pressure beyond tissue perfusion >> compartment • Symptoms >> severe pain beyond expected, unresponce to analgesic • In examination >> tense , swelling , shiny , v. pain in stretched ( early sign) ex. Very pain in dorseflexion of ankle , in unconscious pt / alcohol can’t examine them • There is device for measurement of compartment pressure • 2 measurements >>1)absolute pressure more than 30 or different between diastolic and compartment pressure less than 30. • Presence of pulse doesn’t role out compartment. • Compound fracture not against compartment, not role out compartment syndrome. • Treatment >> immediate fasciotomy • Not treatment >> ischemia, volksmann’s contracture >> ischemic muscle will convert to fibrous tissue.

4. Nerve injury is particularly common with fractures of the humerus or injuries around the elbo or knee. Look for tell tal signs: In closed injuries the nerve is seldom severed, and spontaneous recovery should be awaited – it occurs in 90% of cases within 4 months. If recovery has not occurred by the expected time, and if nerve conduction studies fail to show evidence of recovery, the nerve should be explored Early exploration should also be considered if signs of a nerve injury appear after manipulation of the fracture. In open fractures any nerve lesion is more likely to be complete; the nerve should be explored during wound debridement and repaired at the time of wound closure.

Nerve compression, as distinct from a direct injury, sometimes occurs with fractures or dislocations around the wrist. Complaints of numbness or paraesthesia in the distribution of the median or ulnar nerves should be taken seriously and the patient monitored closely; if there is no improvement within 48 hours of fracture reduction or splitting of bandages around the splint, the nerve should be explored and decompressed.

Common nerve injuries Injury Shoulder dislocation Humeral shaft fracture Humeral supracondylar Elbow medial condyle Elbow dislocation Montegia fracture Hip dislocation Knee dislocation Nerve Axillary Radial or median Ulnar Posterior interosseous Sciatic Peroneal

• Nerve injury >> common site >> shoulder dislocation > axillary nerve. • Fracture of humorous >> radial nerve • Around elbow >> ulnar nerve(although this nerve proximal to elbow but have less chance to be injured) , median n and radial. • Wrist >> median and ulnar nerve. • Around knee>> peroneal n. • Hip dislocation >> sciatic n.

5. Haemarthrosis Fractures involving a joint may cause acute haemarthrosis. The joint is swollen and tense and the patient resists any attempt at moving it. The blood should be aspirated before dealing with the fracture.

6. Infection • Open fractures may become infected; closed fractures hardly ever do unless they are opened by operation. • Post-traumatic wound infection is now the most common cause of chronic osteomyelitis. This does not necessarily prevent the fracture from uniting, but union will be slow and the chance of re-fracturing is increased. Osteomyelitis is an infection of the bone, a rare but serious condition. By. Staphylococcus aureus • ways: Infection in one part of the body may spread through the bloodstream into the bone, or an open fracture or surgery •

Clinical features Following an open fracture or operation, the wound becomes inflamed and starts draining seropurulent fluid. A sample should be submitted immediately for microbiological investigation; while awaiting the result, intravenous antibiotic administration can be started. Infection Wound sinuses and exposed metalwork are sorry sights. X-rays often show that the fracture is ununited

Treatment • All open fractures should be regarded as potentially infected and treated by giving prophylactic antibiotics and meticulously excising all devitalized tissue. • If there are signs of acute infection and pus formation, the tissues around the fracture should be opened and drained; the choice of antibiotic is dictated by tests for bacterial sensitivity. • If internal fixation has been used, this does not necessarily have to be removed. However, if the infection does not respond to antibiotic treatment, it may be necessary to remove the implants and replace them with an external fixation device.

• Late signs of infection may appear in the form of a sinus and/or x-ray evidence of a sequestrum. • The implants and all avascular pieces of bone should be removed; • X-rays often show that the fracture is ununited (ideally a flap) will be needed. An external fixator can be used to bridge the fracture. If the resulting defect is too large for bone grafting at a later stage, the patient should be referred to a centre with the necessary experience and facilities for limb reconstruction. Sequestrum: a piece of dead bone tissue formed within a diseased or injured bone, typically in chronic osteomyelitis.

7. Gas gangrene • This terrifying condition is produced by clostridial infection (especially C. welchii). • These are anaerobic organisms that can survive and multiply only in tissues with low oxygen tension; the prime site for infection, therefore, is a dirty wound with dead muscle that has been closed without adequate debridement. • Toxins produced by the organisms destroy the cell wall and rapidly lead to tissue necrosis, thus promoting the spread of the disease.

Clinical features Appear within 24 hours of the injury: the patient complains of intense pain and swelling around the wound a brownish discharge may be seen; gas formation is usually not very marked. There is little or no pyrexia but the pulse rate is increased and a characteristic smell (once experienced this is never forgotten). Rapidly the patient becomes toxaemic and may lapse into coma and death. It is essential to distinguish gas gangrene, gangrene which is characterized by myonecrosis, myonecrosis from anaerobic cellulitis, in which superficial gas formation is abundant but toxaemia usually slight. Failure to recognize the difference may lead to unnecessary amputation for the non-lethal cellulitis.
 Clinical picture of gas gangrene. (b) X-rays show diffuse gas in")
Gas gangrene (a) Clinical picture of gas gangrene. (b) X-rays show diffuse gas in the muscles of the calf.

Prevention Deep, penetrating wounds in muscular tissue are dangerous; they should be explored, all dead tissue should be completely excised and, if there is the slightest doubt about tissue viability, the wound should be left open. there is no effective antitoxin against C. welchii. Treatment • The key to life-saving treatment is early diagnosis. • General measures, such as fluid replacement and intravenous antibiotics, are started immediately. • Hyperbaric oxygen has been used as a means of limiting the spread of gangrene. • However, the mainstay of treatment is prompt decompression of the wound and removal of all dead tissue • In advanced cases, amputation may be essential

8. Fracture blisters Two distinct types of blistering are sometimes seen after fractures: clear fluid-filled vesicles and bloodstained ones. Both occur during limb swelling and are due to elevation of the epidermal layer of skin from the dermis. There is no advantage in puncturing the blisters (it may even lead to increased local infection) infection and surgical incisions through blisters, whilst generally safe, should be undertaken only when limb swelling has decreased.

9. Plaster sores and pressure sores • Plaster sores occur where skin is pressed directly onto bone. • They should be prevented by padding the bony points and by moulding the wet plaster so that pressure is distributed to the soft tissues around the bony points. • While a plaster sore is developing the patient feels localized burning pain. • A window must immediately be cut in the plaster, as warning pain quickly abates and skin necrosis proceeds unnoticed. • Pressure sores may be produced by splints and other appliances. • These should be checked at frequent intervals to ensure that they fit correctly and comfortably.

• Bed sores are liable to occur in elderly or paralysed patients. • The skin over the sacrum and heels is especially vulnerable. • They can usually be prevented by careful nursing and early activity; once they have developed, • treatment is difficult and it may be necessary to excise the necrotic tissue and cover the defect by plastic surgery. Pressure sores are a sign of carelessness. (a, b) Sores from poorly supervised treatment in a Thomas’ splint. (c) Bed sores in an elderly patient, which kept her in hospital for months.

Late complications , doctor’s note • **Related to treatment > open reduction with internal fixation >> early or late infection >> m. c organism > staphylococcus aureus > treatment by Debridement with cleaning and antibiotics • In early infection >> no need for remove the metal • In late infection >> must remove it , Bacteria will growth on this foreign body(biofilm) and separated it from blood circulation so antibiotic won’t reach bacteria. • **Related to pt personality >> reflex sympathetic dystrophy or regional pain syndrome or Shoulder Hand Syndrome due to sympathetic over activity >> stiffness/swelling/ shiny skin/ hot/ painful peripheral limb. • Treatment: Better to treat it preventive more than treat itself >> by early mobilization of pt, once it’s happened treated by sympathetic block like gabapentin, sympathetic ganglion blockage others > vitamin c , NSAIDs and physiotherapy.

• **Related to union > • Most important factors of union are age and blood supply • 1) delayed union >> bone not union within expected period of time for that fracture. • 2) non union > bone not union within expected period of time with no sign of healing. • Healing process it’s self > it’s inflammatory reaction(pain , swelling , tenderness, hotness) >> so sign of healing (inflammation) present in delay union not in non –union. • >> we wait for 6 months after that we called it non union.
 hypertrophic non union >> bone and")
• Types of non union • 1) hypertrophic non union >> bone and vascularity are good but there is problems in immobilization(stability of fracture)>> there is callus formation but can’t make cross bridges of fracture ends by lamellar bone because of movement. • Treatment >> just provide some stablility. • If not treatment > psudue arthosis >> becomes like a joint with no capsule. • 2) atrophic non- union >> bone failed to form callus, bone ends are atrophic. problem here is vascular • Treatment >> good stabilization , good bone graft , , difficult to heal
Necrotic – non union >> necrotic segments. • Treatment >> remove necrotic")
• 3)Necrotic – non union >> necrotic segments. • Treatment >> remove necrotic segments and put bone graft • 4) gap non union or defect non union. >> bone loss • 2 bones like fibula and tibia >> fibula intact and making traction to tibia (broken) and prevents its from healing so I broke fibula • 1. 5 cm of shortening can be accepted • 5) cross union

Malunion • • • Healing with deviation in normal alignment> vagus , varus , rotation, shortening. Causes>> failure of reduction >> failure of maintain reduction > patient’s or surgeon’s problem. 30 degree malunioun could accept in children , will be normal after 6 months. in adult > 5 degree deformity could affect pronation , supination. Treatment >> depend on age , gender , site of malunion, effect functiona? Indication for surgery >either cosmetic or prevention of future complications (proximal to joint to prevent osteoarthritis) Note>> elbow normally 10 -15 degree in valgus Cubits varus Gun stoke deformity

Late complications 1. Delayed union Causes Factors causing delayed union are either biological, biomechanical or patient related. A. Poor blood supply A badly displaced fracture will cause tearing of the periosteum and interruption of the intramedullary blood supply. The fracture surface may become necrotic and the normal healing process will take longer than usual.

b. Severe soft-tissue damage is the most important cause of delayed union and non-union. It disrupts the blood supply, reduces osteogenesis from mesenchymal stem cells and impairs the effectiveness of muscle splintage. c. Periosteal stripping Over-enthusiastic periosteal stripping during internal fixation is an avoidable cause of non-union.
 or excessive movement at the")
d. Imperfect splintage Excessive traction (creating a fracture gap) or excessive movement at the fracture site will delay ossification in the callus. In forearm or leg fractures, an intact fellow bone may also serve to splint a fracture apart. e. Over-rigid fixation Delays rather than promotes fracture union. It is only because the fixation device holds the fragments securely that the fracture seems to ‘unite’. Union by primary bone healing is slow, but provided stability is maintained throughout, the fracture does eventually unite.

f. Infection Tissue healing is severely hampered by bone lysis, necrosis and pus formation In addition, fixation implants tend to loosen and fracture stability is lost. h. Implant failure Implants may loosen or break apart. g. Patient related Patients come in all shapes and forms. They are sometimes immense, immoderate, immovable or impossible. Proper care can overcome most of these problems.

Clinical features Fracture tenderness persists and if the bone is subjected to stress, pain may be acute. On x-ray the fracture line remains visible and there is very little callus formation or periosteal reaction. However, the bone ends are not sclerosed or atrophic. The appearances suggest that, although the fracture has not united, it eventually will.
 to eliminate any possible cause of")
Treatment Conservative The two important principles are: (1) to eliminate any possible cause of delayed union and (2) to promote healing by providing the most appropriate biological environment. Immobilization (whether by cast or by internal fixation) but fracture loading is an important stimulus to union and this can be enhanced by encouraging muscular exercise and weight bearing in the cast or brace. The watchword is patience; however, there comes a point with every fracture where the ill-effects of prolonged immobilization outweigh the advantages of nonoperative treatment, or where the risk of implant breakage begins to loom.

Operative Each case should be treated on its merits; however, if union is delayed for more than 6 months and there is no sign of callus formation , internal fixation and bone grafting are indicated. The operation should be planned in such a way as to cause the least possible damage to the soft tissues.

2. Non-union In a minority of cases delayed union gradually turns into non-union. Movement can be elicited at the fracture site and pain diminishes; the fracture gap turns into a pseudarthrosis. On x-ray the fracture is clearly visible and the bone on either side of it may be either exuberant or rounded off. • Non-unions being divided into hypertrophic and atrophic types. In hypertrophic non-union the bone ends are enlarged, suggesting that osteogenesis is still active but not quite capable of bridging the gap. In atrophic non-union osteogenesis seems to have eased; the bone ends are tapered or rounded with no suggestion of new bone formation.
 This patient has an obvious pseudarthrosis of the humerus. The x-ray")
Non-union (a, b) This patient has an obvious pseudarthrosis of the humerus. The x-ray shows a typical hypertrophic nonunion. (c) Non-union associated with (a) (b) (c) implant fatigue failure.

Treatment Conservative Non-union is occasionally symptomless, needing no treatment or, at most, a removable splint. Even if symptoms are present, operation is not the only answer; with hypertrophic non-union, functional bracing may be sufficient to induce union, but treatment often needs to be prolonged. Operative With hypertrophic non-union and in the absence of deformity, rigid fixation alone (internal or external) may lead to union. With atrophic nonunion, fixation alone is not enough. Fibrous tissue in the fracture gap, as well as the hard, sclerotic bone ends, should be excised and bone grafts graft packed around the fracture. If there is significant ‘die-back’, this will require more extensive excision and the gap is then dealt with by bone advancement using the Ilizarov technique
 This patient with fractures of the tibia and fibula was")
Non-union – treatment (a) This patient with fractures of the tibia and fibula was initially treated by internal fixation with a plate and screws. The fracture failed to heal and developed the typical features of hypertrophic nonunion. (b) After a further operation, using more rigid fixation (and no bone grafts), the fractures healed solidly. (c, d) This patient with atrophic non-union needed both internal fixation and bone grafts to stimulate bone formation and union (e).

3. Malunion • When the fragments join in an unsatisfactory position (unacceptable angulation, rotation or shortening) = malunited. • Causes : • failure to reduce a fracture adequately, • failure to hold reduction while healing proceeds or gradual collapse of comminuted or osteoporotic bone.

Clinical features The deformity is usually obvious, but sometimes the true extent of malunion is apparent only on x-ray. Rotational deformity of the femur, tibia, humerus or forearm may be missed unless the limb is compared with its opposite fellow. X-rays are essential to check the position of the fracture while it is uniting. This is particularly important during the first 3 weeks when the situation may change without warning (and when deformity can still be easily corrected). At this stage it is sometimes difficult to decide what constitutes ‘malunion’; acceptable norms differ from one site to another and these are discussed under the individual fractures.

Treatment A few guidelines are offered: ■ In adults, fractures should be reduced as near to the anatomical position as possible; appositionis important for healing whereas alignment and rotation are important for function. Angulation of more than 10– 15 degrees in a long bone, or a noticeable rotational deformity, may need correction by re-manipulation, or by osteotomy - is any surgery that cuts and reshapes your bones- and internal fixation. ■ In young children, angular deformities near the bone ends will often remodel with time; rotational deformities will not. ■ In the lower limb, shortening of more than 2 cm is seldom acceptable to the patient and a shoe raise may be indicated; in cases of severe discrepancy, limb lengthening should be considered.
 may be quite different from the")
■ The patient’s expectations (often prompted by cosmesis) may be quite different from the surgeon’s; they should not be ignored. Early discussion with the patient, and a guided view of the x-rays, will help in deciding on the need for treatment and may prevent later misunderstanding. ■ Little is known of the long-term effects of small angular deformities on joint function. However, it seems likely that malalignment of more than 15 degrees in any plane may cause asymmetrical loading of the joint above or below and the lat development of secondary osteoarthritis; this applies particularly to the large weight bearing joints.
 This malunited fracture was treated by corrective osteotomy and internal fixation (b).")
Malunion (a) This malunited fracture was treated by corrective osteotomy and internal fixation (b).

4. Avascular necrosis Certain regions are notorious for their propensity to develop ischaemia and bone necrosis after injury. They are: (1) the head of the femur (after fracture of the femoral neck or dislocation of the hip). (2) the proximal part of the scaphoid (afterfracture through its waist). (3) the lunate (following dislocation). (4) the body of the talus (after fracture of its neck). Avascular necrosis (AVN) is really an early complication of bone injury, because ischaemia occurs during the first few hours following fracture or dislocation. However, the clinical and radiological effects are not seen until weeks or even months later.
 Displaced fractures of the femoral neck are at considerable risk of")
Avascular necrosis (a) Displaced fractures of the femoral neck are at considerable risk of developing avascular necrosis. Despite internal fixation within a few hours of the injury (b), the headfragment developed avascular necrosis. (c) X-ray after removal of the fixation screws.

Clinical features There are no symptoms associated with AVN, but if the fracture fails to unite or if the bone collapses the patient may complain of pain. X-ray shows the characteristic increase in bone density (the consequence of new bone ingrowth in the necrotic segment and disuse osteoporosis in the surrounding parts).

Treatment usually becomes necessary when joint function is threatened. In elderly people with necrosis of the femoral head, an arthroplasty-surgical replacement of a joint- is the obvious choice; in younger people, re-alignment osteotomy (or even arthrodesis-An arthrodesis is a surgical procedure, also called a joint fusion. In performing an arthrodesis, the goal is to permanently hold a joint in a fixed position, and allow the bone to grow across that joint-) may be wiser. AVN in the scaphoid or talus may need no more than symptomatic treatment, but arthrodesis of the wrist or ankle is sometimes needed.

arthroplasty osteotomy arthrodesis

5. Growth disturbance In children, damage to the physis may lead to abnormal or arrested growth of the bone. 6. Joint instability Bone loss or malunion close to a joint may lead to instability or recurrent dislocation. The commonest sites are the shoulder, the elbow and the patella. A more subtle form of instability is seen after fractures around the wrist. Patients complaining of persistent discomfort or weakness after wrist injury should be fully investigated for chronic carpal instability

7. Osteoarthritis A fracture involving a joint may damage the articular cartilage and give rise to post-traumatic osteoarthritis within a period of months. Even if the cartilage heals, irregularity or incongruity of the joint surfaces may cause localized stress and so predispose to secondary osteoarthritis years later. Little can be done to prevent this once the fracture has united.

Late soft-tissue complications 1. Joint stiffness After a fracture commonly occurs in the knee, the elbow, the shoulder and (worst of all) the small joints of the hand Sometimes the joint itself has been injured; a haemarthrosis forms and leads to synovial adhesions. More often the stiffness is due to oedema and fibrosis of the capsule, capsule the ligaments and the muscles muscle around the joint, or adhesions of the soft tissues to each other or to the underlying bone. All these conditions are made worse by prolonged immobilization; immobilization moreover, if the joint has been held in a position where the ligaments are at their shortest, shortest no amount of exercise will afterwards succeed in stretching these tissues and restoring the lost movement completely

Treatment The best treatment is prevention: • Elevation to minimize oedema • Functional bracing rather than full cast immobilization • Exercises that keep the joints mobile from the outset. If a joint has to be splinted, make sure that it is held in the ‘position of safe immobilization’ Joints that are already stiff take time to mobilize, but prolonged and patient physiotherapy can work wonders. However, surgical release of tight structures is sometimes necessary.

2. Heterotopic ossification • Heterotopic ossification in the muscles sometimes occurs after an injury, particularly around the elbow. OR sometimes occurs spontaneously in unconscious patients. • The patient (usually a fit young man) man complain of pain and local swelling. • X-ray is normal at first but a bone scan may show increased activity. Over the next 2– 3 weeks the pain gradually subsides, but joint movement is limited and x-ray may show fluffy calcification in the soft tissues. By 8 weeks bony mass is easily palpable and is clearly defined in the x-ray.

Myositis ossificans: is a condition where bone tissue forms inside muscle or other soft tissue after an injury. It tends to develop in young adults and athletes who are more likely to experience traumatic injuries. Most of the time, myositis ossificans occurs in the large muscles of the arms or the legs Heterotopic Ossification (HO): is the abnormal growth of bone in the non-skeletal tissues including muscle, tendons, or other soft tissue. When HO develops, new bone grows at 3 times the normal rate resulting in jagged, painful joints. Myositis ossificans This followed a fractured head of radius.

Treatment This condition was much more common in by gone years when joints, after plaster immobilization, were treated by vigorous muscle-stretching exercises. This must be avoided; active movements should be introduced gently and gradually, alternating with rest periods in the position of function. If heterotopic bone has already appeared and is blocking movement, it may be helpful to excise the bony mass. Indomethacin or radiotherapy should be given to help prevent recurrence Indomethacin is used to relieve pain, swelling, and joint stiffness caused by arthritis, gout, bursitis, and tendonitis It is also used to relieve pain from various other conditions. This medication is (NSAID) It works by blocking your body's production of certain natural substances that cause inflammation. This effect helps to decrease swelling and pain.

3. Muscle contracture Following arterial injury or a compartment syndrome, syndrome the patient may develop ischaemic contractures of the affected muscles (Volkmann’s ischaemic contracture). Nerves injured by ischaemia sometimes recover, at least partially; thus the patient presents with deformity and stiffness, but numbness is inconstant. The sites most commonly affected are the forearm and hand, the leg and the foot In a severe case affecting the forearm, there will be muscle wasting and clawing of the fingers Volkmann contracture : is a permanent shortening of forearm muscles, usually resulting from injury, that gives rise to a clawlike deformity of the hand, fingers, and wrist. It is more common in children. Volkmann contracture. Supracondylar fracture
 Typical claw-finger deformity due to Volkmann’s ischaemic contracture of the forearm")
Muscle contracture (a) Typical claw-finger deformity due to Volkmann’s ischaemic contracture of the forearm muscles. With the wrist extended, the fingers are drawn into flexion; (b) when the wrist is allowed to flex, the fingers can be straightened, thus indicating that the deformity is due to muscle shortening.

Treatment Detachment of the flexor muscles at their origin and along the interosseous membrane in the forearm may improve the deformity, but function is no better if sensation and active movement are not restored. Nerve grafts may provide protective sensation in the hand, and tendon transfers (wrist extensors to finger and thumb flexors) will allow active grasp. In less severe cases, median nerve sensibility may be quite good and, with appropriate tendon releases and transfers, the patient regains a considerable degree of function. A tendon transfer is a surgery that moves a working muscle and tendon to replace a nonworking muscle and tendon.

4. Tendon rupture Rupture of the extensor pollicis longus tendon may occur after a fracture of the lower radius. Direct suture is seldom possible and the resulting disability is treated by transferring the extensor indicis proprius tendon to the distal stump of the ruptured thumb tendon. Late rupture of the long head of biceps after a fractured neck of humerus usually requires no treatment.

5. Nerve compression may damage the lateral popliteal nerve if an elderly or emaciated patient lies with the leg in full external rotation. Radial palsy may follow the faulty use of crutches. Both conditions are due to lack of supervision

6. Nerve entrapment Bone or joint deformity may result in local nerve entrapment with typical features such as numbness or paraesthesia, loss of power and muscle wasting in the distribution of the affected nerve. Common sites • ulnar nerve (due to a post-traumatic valgus deformity of the elbow) • median nerve (following injuries around the wrist) • posterior tibial nerve (following fractures around the ankle) Treatment is by early decompression of the nerve.

7. Complex regional pain syndrome characterized by pain, stiffness and osteoporosis of the hand The same condition sometimes occurs after fractures of the extremities and for many years it was called Sudeck’s atrophy. More recently it was held to be due to some type of neurovascular dysfunction and it came to be known variously as reflex sympathetic dystrophy or algodystrophy The condition is much more common than was previously recognized and it may occur even after relatively trivial injury. The patient complains of continuous pain, often described as ‘burning’ in character

At first there is local swelling, redness and warmth, as well as tenderness and moderate stiffness of the joints near the site of injury. As the weeks go by the skin becomes pale and atrophic, movements are increasingly restricted and the patient may develop fixed deformities X-rays characteristically show patchy rarefaction of the bone.
 Following a fracture of the tibia, this patient developed")
Complex regional pain syndrome (‘algodystrophy’) Following a fracture of the tibia, this patient developed the typical features of complex regional pain syndrome affecting the right ankle and foot. The skin is atrophic and shiny; the x-ray shows marked regional osteoporosis above and below the ankle.

Treatment The earlier the condition is recognized and treatment begun, the better the prognosis. • Elevation and active exercises are important after all injuries, but in this condition they are essential. • During the early stage anti-inflammatory drugs and amitriptyline are helpful. • Sympathetic block or sympatholytic drugs have been advocated for this condition. They do sometimes appear to help but their effect is unpredictable. • Prolonged and dedicated physiotherapy will usually be needed.
- Slides: 77