Infection Prevention and Control for COVID 19 Module







 of COVID‐ 19 compared to other outbreak‐prone diseases How does virus")






 for COVID‐ 19 Level 1 Level 2 Find “Donning and")
 for COVID‐ 19 Level 1 (no interaction with patients) Level")



 Yes Disposable Aprons Yes Only when anticipating")



 • Patients should be placed in adequately")
 • If transport is required: • use")


 • Provide adequate training in IPC,")


 measures will protect health care workers,")
")







 • Doffing")
- Slides: 41
Infection Prevention and Control for COVID‐ 19 Module 2
Goals of Infection, Prevention, and Control Protect yourself Protect your community Protect your patients
Principles of IPC strategies associated with health care of suspected and confirmed COVID‐ 19 patients 1. Screening, early recognition, and source control (isolating patients with suspected COVID‐ 19) 2. Application of standard precautions for all patients 3. Implementation of empiric additional precautions: • Droplet and contact precautions for all suspected cases • Consider airborne precautions for aerosol‐generating procedures 4. Administrative controls 5. Environmental and engineering controls
1. Screening, early recognition, and source control • Encourage HCWs to have a high level of clinical suspicion and use updated case definitions. • Establish a well‐equipped screening station at the entrance of health facilities. • Reinforce adherence to standard precautions especially respiratory hygiene and hygiene. • Ensure that patients with symptoms of suspected COVID‐ 19 or other respiratory infection (e. g. , fever, cough) are not allowed to wait among other patients seeking care. Provide a medical mask to symptomatic patients. Find “Screening and triage” video link in slide appendix
2. Apply standard precautions for all patients • Hand hygiene • Respiratory hygiene • Appropriate Personal Protective Equipment (PPE) according to risk assessment • Injection safety practices/ sharps safety • Safe waste management • Proper linens, environmental cleaning and sterilization of patient‐care equipment
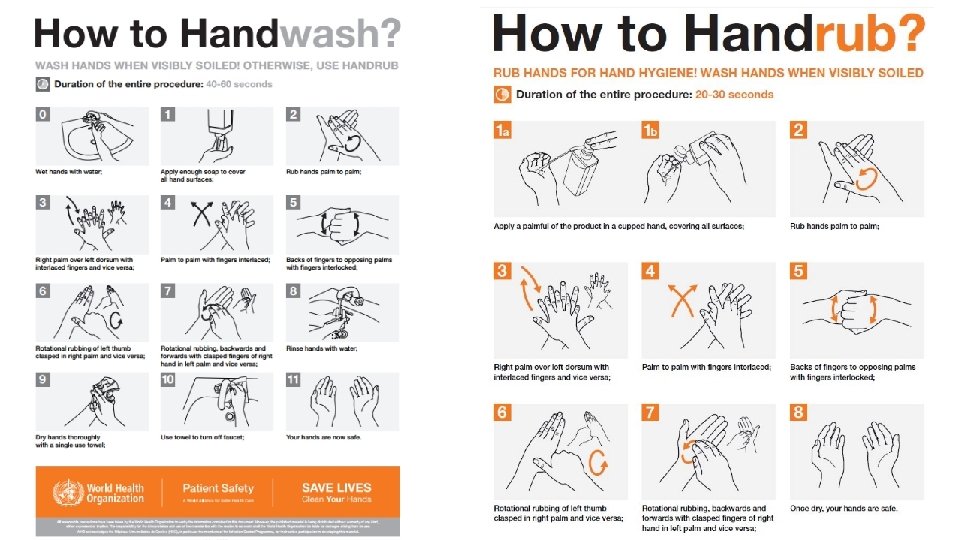
Hand hygiene is the most important measure to prevent infection Find “Hand hygiene” video link in slide appendix
Respiratory or cough etiquette Cover mouth and nose when coughing and sneezing Maintain social distance (2 m) from others Cover mouth/nose with tissue dispose of tissues in nearest waste bin perform hand hygiene Offer medical mask to suspected COVID‐ 19 patients while in waiting/ public areas or in isolation rooms
Contagiousness (R 0) of COVID‐ 19 compared to other outbreak‐prone diseases How does virus spread? R 0 (expected number of susceptible individuals who can be infected by a single case) Ebola Virus Disease (EVD) COVID‐ 19 Direct contact with blood or non‐respiratory body fluids (e. g. , vomit, stool, saliva, urine, breast milk, semen, etc) Direct contact Inhalation of with respiratory small droplets respiratory droplets Contaminated (aerosols) hands after poor respiratory etiquette play a key role in transmission. ~2 ~2. 5 Measles ~16 https: //www. weforum. org/agenda/2020/03/a‐visual‐history‐of‐pandemics
Primary modes of transmission for: COVID‐ 19 vs measles vs Ebola COVID‐ 19 1 meter Source: www. npr. org 2 meters
3. Implementation of empiric additional precautions: applying droplet precautions • Droplet precautions prevent large droplet transmission of respiratory viruses. • Use a medical mask if working within 2 m of the patient. • For suspect cases, place patients in single rooms if available or separate patients by 2 m spatial separation. • When providing care in close contact with a patient with respiratory symptoms (e. g. , coughing or sneezing), use eye protection (face shield or goggles). • Limit patient movement within the institution and ensure that patients wear medical masks when outside their rooms.
3. Implementation of empiric additional precautions: applying contact precautions SARS‐Co. V‐ 2 can remain on surfaces for ~2 days. • Droplet and contact precautions prevent direct or indirect transmission from contact with contaminated surfaces or equipment. • Use PPE (medical mask, eye protection, gloves and gown) when entering room and appropriately remove PPE when leaving. • If possible, use either disposable or dedicated equipment (e. g. , stethoscopes, blood pressure cuffs and thermometers). • If equipment needs to be shared among patients, clean and disinfect between each patient use. • Refrain from touching your eyes, nose, and mouth with potentially contaminated gloved or ungloved hands.
3. Implementation of empiric additional precautions: applying airborne precautions Use when performing Aerosol‐Generating Procedures (AGP) • Use Level 4 PPE, including gloves, long‐sleeved gowns, eye protection and fit‐tested particulate respirators (N 95 or equivalent or higher level of protection). • Whenever possible, use adequately ventilated single rooms. • Avoid the presence of unnecessary individuals in the room. • Due to risk for AGPs during intubation procedures and potentially while a patient is mechanically ventilated, maintain care for the patient in the same type of room where the patient was intubated to avoid risk of aerosol spread to other parts of the health facility.
PPE covers the most important places where germs can enter your body EYES NOSE LIPS You must ALWAYS protect these areas of the body when interacting with suspect and confirmed patients! HANDS
PPE Components for COVID‐ 19 Face Mask N 95 Mask Faceshield Goggles Hair cover* Surgical cap/bonnet Nose + mouth Eyes +nose + mouth Eyes Hair Head Gown Apron Gloves Body Hands *if applicable (e. g. , long hair or large hairdo) Gumboots Feet Shoe covers Feet/shoes
Personal protective equipment (PPE) for COVID‐ 19 Level 1 Level 2 Find “Donning and doffing” video link in slide appendix WHO: The COVID-19 Risk Communication Package For Healthcare Facilities Level 3 Level 4 Consider addition of gumboots/shoe covers if entering COVID‐ 19
Personal protective equipment (PPE) for COVID‐ 19 Level 1 (no interaction with patients) Level 2 (patient interaction without contact) Level 3 (patient contact, no risk of aerosols) Level 4 (risk of aerosols with or without patient contact) Setting In the community or in the hospital where there is no interaction with patients (e. g. , administrative areas; cafeterias) • Screening at entry points • Ambulance drivers • Patient care for non‐suspect patients with no respiratory symptoms • Caring for suspected or confirmed COVID‐ 19 patients with no aerosol risk • Transfer of suspect/confirmed patients • Collection of respiratory samples • Cleaners • Preparing a deceased body • Aerosol generating procedures (AGPs) involving a suspect or confirmed COVID‐ 19 patient [e. g. , bronchoscopy, tracheal • • • intubation, CPR, airway suctioning, sputum induction, NG tube placement, non‐invasive ventilation (CPAP; BIPAP), high‐flow nasal cannula oxygenation] PPE No PPE. Home clothes/scrubs with closed shoes. Medical mask * Facial protection (face shield or goggles) should be used when unable to maintain 2 m social distance Facial protection (face shield or goggles), surgical gown, gloves (x 2), medical mask, shoe covers/gum boots, hair cover (for long hair or large hairdos) * Add a plastic apron if gown is not water resistant Level 3 PPE with the following modifications: • N 95 mask instead of a medical mask • Addition of a head covering (e. g. surgical bonnet) Caring for suspected or confirmed COVID‐ 19 patients in an * Coveralls (with N‐ 95 mask) may be used as an alternative ICU or HDU (where AGPs are common) Laboratory personnel Autopsy
Level Setting Level 1 In the community or in the hospital where No PPE. Home clothes/scrubs with closed there is no interaction with patients (e. g. , shoes. administrative areas; cafeterias) (no interaction with patients) Level 2 (patient interaction without contact) • Screening at entry points • Ambulance drivers • Patient care for non‐suspect patients with no respiratory symptoms PPE Medical mask *Facial protection (face shield or goggles) should be used when unable to maintain 2 m social distance.
Level Setting PPE Level 3 • Caring for suspected or confirmed COVID‐ 19 patients with no aerosol risk • Transfer of suspect/confirmed patients • Collection of respiratory samples • Cleaners • Preparing a deceased body Medical mask, facial protection (face shield or goggles), surgical gown, gloves (x 2), shoe covers/gum boots, hair cover (for long hair or large hairdos) (patient contact, no risk of aerosols) Level 4 (risk of aerosols with or without patient contact) *Add a plastic apron if gown is not water resistant • Aerosol generating procedures (AGPs) Level 3 PPE with the following involving a suspect or confirmed modifications: COVID‐ 19 patient [e. g. , bronchoscopy, • N 95 mask instead of a medical mask tracheal intubation, CPR, airway • Addition of a head covering (e. g. , suctioning, sputum induction, NG tube surgical bonnet) placement, non‐invasive ventilation (CPAP; BIPAP), high‐flow nasal cannula oxygenation] • Caring for suspected or confirmed COVID‐ 19 patients in an ICU or HDU (where AGPs are common) • Laboratory personnel • Autopsy *Coveralls (with N‐ 95 mask) may be used as an alternative.
Differences in PPE recommended for COVID‐ 19 vs EVD PPE for direct patient care for COVID‐ 19 PPE for direct patient care for Ebola Virus Disease Head cover if Level 4 risk ………. . . N 95 (or equivalent) if Level 4 risk Double gloves ………… Shoe covers or gumboots Adopted from: https: //www. cdc. gov/coronavirus/2019‐ncov/downloads/COVID‐ 19_PPE_illustrations‐p. pdf
PPE Component EVD COVID‐ 19 Gloves (double) Yes Disposable Aprons Yes Only when anticipating body fluid exposure (e. g. , non‐fluid resistant gown) N 95 Respirators Only for aerosol risk (*N 95 respirators are often used, however, because of the recommendation for water-resistant, structured masks) Only for Level 4 risk Yes Goggles/face shield Yes Shoe covers/gumboots Yes Surgical Masks (*need to be water-resistant and structured so that they do not collapse against a HCWs mouth) (gumboots preferred) (shoe covers preferred) Coveralls Yes Alternative to gowns if Level 4 risk Gowns No Yes Separate hood/head covering Yes Head covers (e. g. , surgical bonnet) if Level 4 risk When applicable (e. g. , long hair or large hairdo) Hair cover
Rationale for COVID‐ 19 PPE: N 95 respirators do not provide added benefit over medical masks for HCW during non‐aerosolizing procedures STUDY TITLE Long Y, Hu T, Liu L, et al (2020). STUDY DESIGN, SETTING AND PARTICIPANTS A systematic review and meta‐analysis to assess the effectiveness of N 95 respirators versus surgical masks for prevention of influenza. A total of six RCTs involving 9, 171 participants were included. Bartoszko, J. J. , Farooqi, M. A. M. , Alhazzani, W. , & Loeb, M. (2020). Systematic review to compare medical masks to N 95 respirators in preventing laboratory‐confirmed viral infection and respiratory illness including coronavirus specifically in healthcare workers. Four RCTs were meta‐analyzed adjusting for clustering. CONCLUSION The use of N 95 respirators compared with surgical masks is not associated with a lower risk of laboratory‐confirmed influenza. It suggests that N 95 respirators should not be recommended for general public and non‐high‐risk medical staff who are not in close contact with influenza patients or suspected patients. 1‐ Low certainty evidence suggests that medical masks and N 95 respirators offer similar protection against viral respiratory infection including coronavirus in healthcare workers during non– aerosol‐generating care. 2‐ Preservation of N 95 respirators for high‐risk, aerosol‐generating procedures in this pandemic should be considered when in short supply.
Rationale for COVID‐ 19 PPE: Gowns are as effective as coveralls and coveralls are more difficult to doff “Covering more parts of the body leads to better protection but usually comes at the cost of more difficult donning or doffing and user comfort, and may therefore even lead to more contamination. ” • A long gown may be the best compromise between protection and ease of doffing • In an RCT where 59 participants donned and doffed 3 different types of EVD PPE [PPE 1 and PPE 3 (gowns) vs PPE 2 (coverall)] in a random order, • Participants with a long gown (PPE 1) had less contamination than those with a coverall [median small patches of contamination: 5. 00 (PPE 1) vs 7. 00 (PPE 2), p < 0. 05] • Coveralls were more difficult to doff [i. e, . greater % of doffing protocol deviations: 9. 48% (PPE 2) vs 2. 95% (PPE 1)] • A more breathable fabric may still lead to similar levels of contamination protection to less breathable fabric and may be preferred by users Verbeek JH, et al. Cochrane Database of Systematic Reviews 2020, Issue 4. Art. No. : CD 011621. DOI: 10. 1002/14651858. CD 011621. pub 4 Suen LKP, et al. Antimicrobial Resistance & Infection Control 2018; 7(157).
Rationale for COVID‐ 19 PPE: Ugandan guidelines are consistent with recommendations from the region COUNTRY Face Mask N 95 / FFP 2 Gown Coverall Comments Kenya For droplet and contact precautions Only for aerosol generating procedures Recommended standard Not recommended Available from: South Africa For droplet and contact precautions Only for aerosol generating procedures Recommended standard Not recommended Available from: Nigeria For droplet and contact precautions Only for aerosol generating procedures Recommended standard Not recommended Available from: https: //kma. co. ke/Documen ts/Case%20 management%20 protocol. pdf http: //www. health. gov. za/in dex. php/component/phocad ownload/category/628 https: //ncdc. gov. ng/themes/ common/docs/protocols/18 9_1586635002. pdf
3. Implementing empiric additional precautions (cont. ) • Patients should be placed in adequately ventilated single rooms • When single rooms are not available, patients suspected of being infected with COVID‐ 19 should be grouped together (“cohorting”) • Suspect COVID‐ 19 patients should be separated from the confirmed cases • All patients’ beds should be placed at least 2 m apart, especially when COVID‐ 19 status is unknown (i. e. , area for suspected patients)
3. Implementing empiric additional precautions (cont. ) • If transport is required: • use pre‐determined transport routes to minimize exposure for staff, other patients and visitors • offer a medical mask for the patient to wear during transport • Routinely clean and disinfect surfaces with which the patient has contact • Maintain a record of all persons entering the patient’s room, including staff and visitors
3. Implementing empiric additional precautions— Isolation Rooms • Room doors should be kept closed except when entering or leaving the room • Personnel entry and exit should be minimized • Patient movement out of the room should also be minimized • Once transported to a designated isolation room for confirmed cases, a patient can remove her or his facemask • Outside the isolation room, patients should wear a facemask to contain secretions and droplets • Personnel entering the room should use appropriate PPE • Patient rooms should undergo appropriate cleaning and surface disinfection before it is returned to routine use
4. Implementing administrative controls • Establish sustainable IPC infrastructure and activities to prevent hospital‐acquired infections • Educate patients and patients’ caregivers on IPC measures • Develop SOPs on the early recognition of acute Respiratory Tract Infections, including COVID‐ 19 • Ensure access to prompt laboratory testing for diagnosis of illness • Provide dedicated waiting areas for symptomatic patients with COVID‐ 19 • Appropriately isolate hospitalized patients with COVID‐ 19 • Ensure adequate supplies of PPE for COVID‐ 19
4. Implementing administrative controls— Health Care Workers (HCWs) • Provide adequate training in IPC, PPE donning and doffing and clinical management to HCWs • Ensure an adequate patient‐to‐staff ratio • Establish a surveillance process for acute Respiratory Tract Infections potentially caused by COVID‐ 19 among HCWs • Monitor HCW compliance with standard precautions and provide mechanisms for improvement as needed
5. Using Environmental and Engineering Controls • Spatial separation of at least 2 m should be maintained between all suspected and confirmed COVID‐ 19 patients • Ensure that cleaning and disinfection procedures are followed consistently and correctly • Clean environmental surfaces with water and detergent or commonly used hospital disinfectants (such as sodium hypochlorite) • Manage laundry, food service utensils and medical waste in accordance with safe routine procedures
Recommendations for Outpatient Care Screening and triage for early recognition Emphasis on hand hygiene and respiratory hygiene Prioritization of care of symptomatic patients When symptomatic patients are required to wait, ensure they have a separate waiting area and have been offered facemasks • Educate patients and families about the early recognition of symptoms, basic precautions to be used and to which health care facility they should be referred • •
Summary • Strict infection, prevention, and control (IPC) measures will protect health care workers, patients, and the community • Effective IPC requires establishing screening at health facility entry, application of standard precautions, following appropriate PPE procedures, and instituting both administrative and environmental controls • Hand hygiene is the most important measure to prevent infection • Appropriate PPE for direct contact with patients having suspected or confirmed COVID-19 consists of: medical mask, facial protection (face shield or goggles), surgical gown, gloves (x 2), shoe covers/gum boots, and a hair cover (for long hair or large hairdos). o N‐ 95 respirators and surgical bonnets should be added if aerosol generating procedures are being conducted. • Coveralls are the most appropriate PPE for viral hemorrhagic fevers such as Ebola • Environmental and administrative controls should guide patient flow, isolation procedures, and disinfection routines.
References • Infection prevention and control during health care when novel coronavirus (COVID‐ 19) infection is suspected Interim guidance 25 January 2020. WHO • Interim Infection Prevention and Control Recommendations for Patients with Known or Patients Under Investigation for 2019 Novel Coronavirus in a Healthcare Setting. CDC • Uganda Ministry of Health National Guidelines for Management of COVID‐ 19, 2020 • Verbeek JH, et al. Cochrane Database of Systematic Reviews 2020, Issue 4. Art. No. : CD 011621. DOI: 10. 1002/14651858. CD 011621. pub 4 • Suen LKP, et al. Antimicrobial Resistance & Infection Control 2018; 7(157).
IPC and PPE Donning/Doffing Appendix
COVID‐ 19 Screening and Triage Video • Video requires wifi to play it • Once connected to the internet, click movie icon above • Once page with videos appears, select video #1 (‘Setting up Screening and Triage Areas’)
Hand Hygiene Video • Video requires wifi to play it • Once connected to the internet, click movie icon above • Once page with videos appears, select video #2 (‘Hand Hygiene’)
COVID‐ 19 PPE Donning/Doffing Video • Video requires wifi to play it • Once connected to the internet, click movie icon above • Once page with videos appears, select video #4 (‘Appropriate Use of Personal Protective Equipment’)
Steps for Donning COVID‐ 19 PPE 1. Before starting the donning process, make sure you have hydrated, used the bathroom and change from your personal shoes into gumboots. For staff with long hair/large hairdos and not requiring a head cover (see step 9), put on a hair cover. 2. Identify and gather the correct size/fit of PPE to don. 3. Perform hand hygiene. 4. Put on first pair of gloves 5. Put on isolation gown. Tie all of the ties on the gown. Assistance may be needed by another HCW. If there is a thumb hook sewn into the wrists of the gown, secure the gown with your thumb to avoid slip ups that could expose arms. 6. Put on medical mask (or NIOSH‐approved N 95 respirator if managing a patient with aerosol‐generating procedures). Both your mouth and nose should be protected. [*Do not wear respirator/facemask under your chin or store in scrubs pocket between patients. ] v Medical mask: Mask ties should be secured on crown of head (top tie) and base of neck (bottom tie). If mask has loops, hook them appropriately around your ears. Facemask should be extended under chin. v Respirator: Respirator straps should be placed on crown of head (top strap) and base of neck (bottom strap). Respirator should be extended under chin. Perform a user seal check each time you put on the respirator. If the respirator has a nosepiece, it should be fitted to the nose with both hands, not bent or tented. Do not pinch the nosepiece with one hand. 7. Put on reusable face shield or goggles. 8. If you are using a gown that is not fluid‐resistant, don a disposable apron before proceeding to the next step. 9. If managing a patient with aerosol‐generating procedures, put on head cover (e. g. , surgical bonnet) over face shield/ goggles (see instructional slide) 10. Put on second pair of gloves. Gloves should ideally have a cuff long enough to cover the cuff (wrist) of gown. 11. Have a colleague check you to ensure that have donned correctly before entering the patient care area
Steps for Doffing COVID‐ 19 PPE 1. Perform hand hygiene. 2. Remove gown. v Untie all ties (or unsnap all buttons). Some gown ties can be broken rather than untied. Do so in gentle manner, avoiding a forceful movement. v Reach up to the shoulders and carefully pull gown down and away from the body. v Remove gown allowing the outer pair of gloves to be removed at the same time. Dispose in the waste bin 3. Perform hand hygiene. 4. Remove head cover if wearing Level 4 PPE (see instructional slide) 5. Remove face shield or goggles. Carefully remove face shield or goggles by grabbing the strap and pulling upwards and away from head. Do not touch the front of face shield or goggles. Place the goggles/face shield in a designated reusable PPE receptacle. 6. Perform hand hygiene 7. Remove and discard medical mask (or N 95 respirator). Do not touch the front of the mask. v v Medical mask: Carefully untie from back of head (or unhook from the ears) and pull away from face without touching the front. Respirator: Remove the bottom strap by touching only the strap and bring it carefully over the head. Grasp the top strap and bring it carefully over the head. Pull the respirator away from the face using the top strap (without touching the front of the respirator) and discard in the appropriate waste bin. 8. Perform hand hygiene on inner gloves. 9. Remove hair cover and shoe covers (where applicable). Perform hand hygiene after removing each element 10. Remove inner pair of gloves avoiding touching bare skin with potentially contaminated areas of the gloves (use the clean‐to‐clean and dirty‐to‐dirty technique). 11. If you are using gumboots, step into a footbath with 0. 5% chlorine solution for 15‐ 20 s. 12. Perform hand hygiene and proceed to low risk area
When donning a head covering, it should be placed over the face shield or goggles 1 2 4 3 5 6
Steps for doffing a PPE head covering (e. g. , surgical bonnet) • Doffing your PPE head covering (e. g. , surgical bonnet) should occur after the gown and outer gloves have been removed • Perform a glove washing step prior to doffing head cover • Untie or (rip if material allows) the head cover and remove from back to front • Dispose of head cover into the appropriate rubbish receptacle • Perform a glove washing step before proceeding with next doffing steps