The leukaemias are a group of disorders characterized







 is caused by an accumulation of lymphoblasts in the bone")


 according to WHO (modified from WHO 2008")
 primarily affects older adults; the median age is 50 years, it")


 according to the WHO classification 2016")









 : Immunophenotyping is very useful in distinguishing ALL from AML,")
 e. g. Myeloperoxidase and")
")
 positivity for acid phosphatase in lymphoblasts.")
 translocation. The green probe hybridizes")

- Slides: 34
The leukaemias are a group of disorders characterized by the accumulation of malignant white cells in the bone marrow and blood. Classification of leukaemia The main classification is into: acute and chronic leukaemias, which are further subdivided into lymphoid or myeloid.
�Acute leukaemias are usually aggressive diseases in which malignant transformation occurs in the haemopoietic stem cell or early progenitors. -Acute leukaemia is either acute myeloid leukaemia (AML) or acute lymphoblastic leukaemia (ALL).
PATHOGENESIS The principal pathogenic defect in acute leukemia is a block in differentiation. This block in differentiation “maturation arrest” stems from acquired maturation arrest mutations in specific transcription factors that regulate the differentiation of immature lymphoid or myeloid progenitors.
-Approximately 90% of ALL have chromosomal changes. Many of the chromosomal aberrations dysregulate the expression or function of transcription factors that control normal B- and T-cell development and lead to maturation arrest e. g. Hyperdiploidy , hypodiploidy.
-Most genetic aberrations in AML interfere with transcription factor activities required for normal myeloid cell differentiation. For example t (15; 17). Many AML ‘driver mutations’ have been identified, e. g. FLT 3 , NPM 1
These events cause accumulation in the bone marrow of early haemopoietic cells known as blast cells. -
These abnormal cells cause symptoms of leukaemia because of: 1. Bone marrow failure: blasts accumulating in the failure: marrow suppress the growth of normal hematopoietic cells (e. g. anaemia , neutropenia , thrombocytopenia). 2. Infiltration of organs (e. g. liver, spleen, lymph 2. Infiltration of organs nodes, meninges, brain, skin or testes).
-Acute lymphoblastic leukaemia (ALL) is caused by an accumulation of lymphoblasts in the bone marrow. It is the most common malignant disease of childhood ( 75% of cases occur before the age of 6 years). Eighty five per cent of cases are of B‐cell lineage with the rest being of T‐cell lineage. -
Lymphoblasts
ALL
Classification of acute lymphoblastic leukaemia (ALL) according to WHO (modified from WHO 2008
�Acute myeloid leukaemia(AML) primarily affects older adults; the median age is 50 years, it is caused by an accumulation of myeloid blasts( Myeloblasts). . .
�Auer rods, distinctive red-staining rodlike structures, may be present in myeloblasts. �Auer rods are specific for neoplastic myeloblasts and thus a helpful diagnostic clue when present.
Myeloblasts
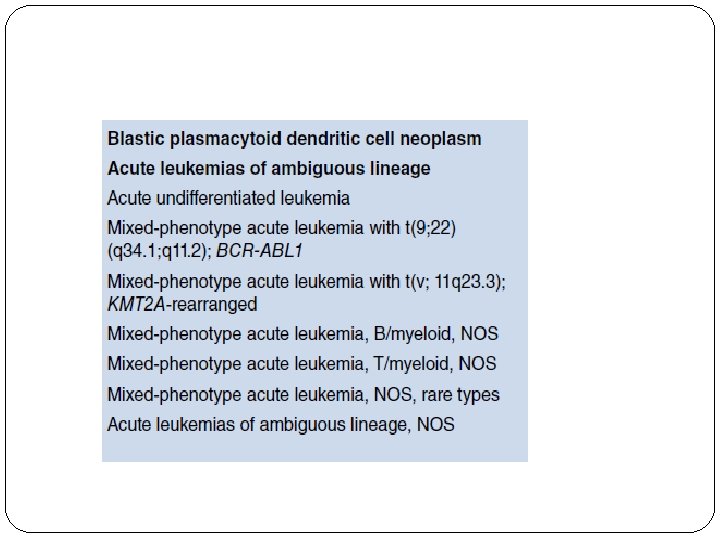
Classification of acute myeloid leukaemia (AML) according to the WHO classification 2016
Clinical Features of Acute Leukemias: • Abrupt, stormy onset. Most patients present for medical attention within 3 months of the onset of symptoms. •
• -Clinical signs and symptoms related to suppressed marrow function, function including fatigue (due to anemia), fever (reflecting infections resulting from neutropenia), and bleeding (petechiae, ecchymoses, epistaxis, gum bleeding) secondary to thrombocytopenia
Infection
Bone pain and tenderness, resulting from marrow expansion and infiltration of the subperiosteum - --Generalized lymphadenopathy, splenomegaly, and hepatomegaly due to dissemination of the leukemic cells. These are more pronounced in ALL than in AML.
Lymphadenopathy in ALL
• Central nervous system manifestations, including headache, vomiting, and nerve palsies resulting from meningeal spread. These are more common in children than in adults and in ALL than in AML. ALL - Granulocytic sarcoma as a discrete tissue mass can be seen in AML.
Nerve palsy
Diagnosis of Acute Leukemias: • The diagnosis is started by first by clinical suspension then diagnosis is made by : 1 -Complete blood count: WBCs count: usually high , neutropenia RBCs : anemia Platelet : low or normal. 2. Morphology (Microscopic examination) of 2. Morphology peripheral blood film and bone marrow aspirate and biopsy.
�The diagnosis of acute leukemia rests on the presence of over 20% of blast cells in the bone marrow at clinical presentation. However, it can be diagnosed with less than 20% blasts if specific leukaemia‐associated cytogenetic or molecular genetic abnormalities are present. �
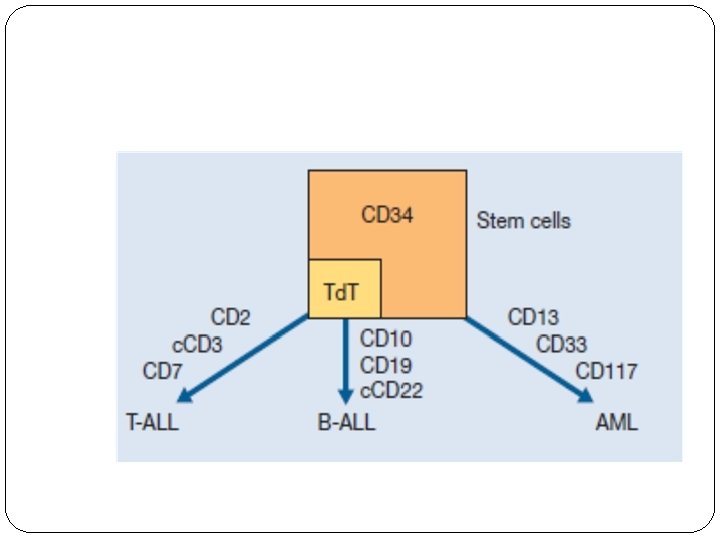
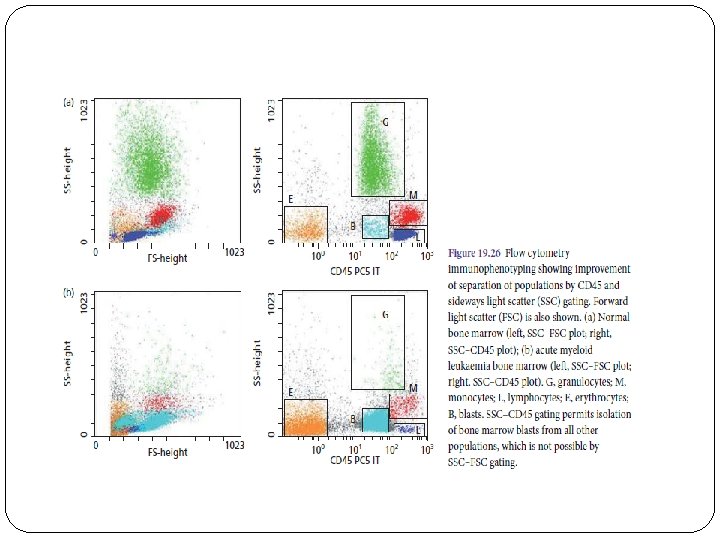
3. Immunophenotyping (flow cytometry) : Immunophenotyping is very useful in distinguishing ALL from AML, subtyping of them. The typical ‘myeloid immunophenotype’ is CD 13, CD 33+ CD 117, and Td. T−. The lymphoid phenotype is : CD 10+ , CD 19+, c. CD 22+ for B-ALL, CD 2+ , c. CD 3+, CD 7+ for T-ALL
4. Cytochemical analysis: (performed in some countries instead of immunophenotyping) e. g. Myeloperoxidase and Sudan black are positive in AML cases. 5. Cytogenetic and molecular studies: to identify leukaemia specific mutations , translocations, chromosomal abnormalities
SBB localised positive reaction in the blast cells(AML)
T-lineage acute lymphoblastic leukaemia showing focal (Golgi zone) positivity for acid phosphatase in lymphoblasts. Cytospin preparation, acid phosphatase reaction .
An example of FISH analysis showing the t(12; 21) translocation. The green probe hybridizes to the region of the ETV 6 gene on chromosome 12 and the red probe hybridizes to the region of the RUNX 1 gene on chromosome 21. The arrows point to the two derived chromosomes resulting from the reciprocal translocation.