Primary and Secondary Prevention of CVD Donald M



 Risk Prediction The CHD Prevention Iceberg")
























 LDL-C and Lipid Changes Simva 40 vs. Simva 40/Ezetimibe 10 7")
 Primary Endpoint Cardiovascular Death, MI, Stroke, documented Unstable Angina requiring rehospitalization,")

 - Pts with")
 Time to First Ischemic Event Angioplasty / UC Atorvastatin p")


 NEJM 2011")
 ER niacin/laropriprant-simvastatin vs. simvastatin: No ASCVD event reduction vs")
 ER niacin/laropriprant-simvastatin vs. simvastatin: No ASCVD event reduction vs")




 somewhat for weight loss • Focus on")















: 1281 -1357")
: 1281 -1357")




 Design • International multicenter trial • Ppts")
 -")













")






- Slides: 89
Primary and Secondary Prevention of CVD Donald M. Lloyd-Jones MD Sc. M FACC FAHA
Spectrum of Prevention for CVD • Secondary Prevention - MI/ACS - Chronic CHD, PAD, DM(? ), CKD(? ) - Post-stroke/TIA • Primary Prevention - High, intermediate, low global risk - Individual risk factors • Primordial Prevention - Prevention of RF development
Guiding Concepts in Prevention • Thomas Strasser, 1978 - “Primordial prevention” - Prevention of the development of risk factors, not just disease • Once risk factors develop, risk for disease is high and difficult to reduce substantially • Geoffrey Rose, 1981 - “High-risk” vs. “population” strategies for prevention of disease - Current guidelines focus mostly on “high-risk” strategies, where relative risk is high - Shifting the population distribution of a risk factor can have dramatic impact on disease
Estimated 10 -Year Risk Current (a la 2012) Risk Prediction The CHD Prevention Iceberg High Prevalence in US ~8 -10% >20%, CHD or DM Intermediate 10% - 20% Low <10% ~10 -12% ~80%
Population-Based Strategy Stamler 1991; Whelton 2002
Clinical Prevention Trials in CV Disease • The first question: “Why the heck are we talking about clinical trials in a course that is supposed to focus on epidemiology? ” • Answer: “How do we know all of these risk factors actually cause CVD? ”
Criteria to Postulate a Causal Association between RF and Disease 1. Exposure to the RF precedes the onset of disease 2. Strong association between exposure and incidence of disease 3. Association is dose-dependent 4. Exposure predicts disease in a variety of populations 5. Association is independent of other RFs 6. Association is biologically plausible And…
Criteria to Postulate a Causal Association between RF and Disease 7. Intervention to modify or abolish the RF results (in large samples) in a lower incidence of disease Here is where clinical trials come in… They are just extensions of epidemiology, but we have more control over the environment/exposure
What is a clinical trial? Critical features of design • Hypothesis to be tested: e. g. , lowering cholesterol will lead to a reduction in CHD events • Equipoise exists – is it ethical to do a trial?
What is a clinical trial? Critical features of design • Appropriate selection of patients • Easily definable phenotype on which to intervene • Relative homogeneity of study sample • People who have some risk of disease – With whom should you start to test your hypothesis? • Secondary>primary high risk>primary low risk
What is a clinical trial? Critical features of design • Define intervention: YOU CONTROL THE EXPOSURE! - What is it? - How do you decide who gets it? - How long do you deliver it?
What is a clinical trial? Critical features of design • Sample size • Easily definable endpoint • Close follow up - Compliance - Endpoints • Data management and statistical issues - On-treatment vs By-randomization analysis
What is a clinical trial? Critical features of design • Which leads us to the Prospective, Randomized, Double-blind, Placebocontrolled Clinical Trial • Considered the highest form of clinical evidence
Secondary Prevention
Secondary Prevention Scope of the Problem • Within 1 year after an initial recognized MI: - The mortality is as high as 25% for men and 38% for women • Within 6 years: - 18% of men and 35% of women will have a second MI - 7% of men and 6% of women will have SCD - 22% of men and 46% of women will have overt CHF
Secondary Prevention Scope of the Problem • Outcomes similar after unrecognized MI and after unstable angina • The elderly are at highest risk for recurrent events and death • Patients with clinical CHD have a large burden of subclinical disease - Not necessarily evident/impressive at angiography - Prone to plaque rupture - Goal of secondary prevention is to stabilize/regress residual disease
Secondary Prevention Historical Perspective • 1950 s-1970 s • 1970 s-1980 s • 1980 s-1990 s • 1990 s-2000 s • 2000 s- Bedrest, CCU Aspirin, Beta-blockers Initial interest in cholesterol Rx, diet, exercise ACE-I Lipids, inflammation, thrombosis, metabolic syndrome HF prevention, SCD prevention
AHA/ACC Secondary Prevention Guidelines 2011 JACC/Circ Nov, 2011
Lifestyle Modification Cornerstone of Secondary Prevention • Smoking Cessation - 50% reduction in recurrent MI in 2 years - 33% reduction in restenosis post-PTCA • Cardiac Rehabilitation - 25% reduction in sudden cardiac death; less clear reductions in MCE • Glucose control: Equivocal but sensible • Weight control: Equivocal but favorable effects on risk factors
Secondary Prevention “Standard” Therapies for Overt CHD • Aspirin: 50% reduction in death/NFMI • Other anti-platelet agent (for most) • Beta-blockers: 25% reduction in CHD death, especially SCD • ACE-inhibitors: 15 -20% reductions in mortality/HF depending on setting • Statin
ACE Inhibitor Evidence Secondary Prevention Meta-Analysis of the HOPE, EUROPA and PEACE Trials* Clinical Trial N Deaths RR of Mortality HOPE 9, 297 EUROPA 12, 218 795 HR=0. 89 P=0. 10 8, 290 633 HR=0. 89 P=0. 13 33, 960 >3, 000 PEACE All Trials 1, 051 HR=0. 84 P=0. 005 HR=0. 86 P<0. 001 0. 4 0. 6 0. 8 ACE-I Better 1. 0 1. 2 1. 4 1. 6 Placebo Better * 7 RCTs, 33, 960 randomized patients and 4. 4 years of mean follow-up. Other findings include a CVD HR=0. 81, MI HR=0. 82 and stroke HR=0. 77. ACE-I = Angiotensin converting enzyme inhibitors, CVD = Cardiovascular disease, MI = Myocardial infarction Danchin N et al. Arch Intern Med 2006; 166: 787 -796 22
b-blocker Evidence Secondary Prevention Summary of Secondary Prevention Trials of b-blocker Therapy for Mortality Prevention Phase of Treatment Total # Patients Acute treatment 28, 970 2 o prevention 24, 298 Overall 53, 268 RR (95% CI) 0. 87 (0. 77 -0. 98) 0. 77 (0. 70 -0. 84) 0. 81 (0. 75 -0. 87) 0. 5 1. 0 2. 0 RR of death b-blocker better Placebo better Still true? CI = Confidence interval, RR = Relative risk Antman E, Braunwald E. Acute Myocardial Infarction. In: Braunwald E, Zipes DP, Libby P, eds. Heart Disease: A textbook of Cardiovascular Medicine, 6 th ed. , Philadelphia, PA: W. B. Sanders, 2001, 1168. 23
Cholesterol-Lowering Drug Therapy Drug Class Demonstrated Benefits Statins ↓Total/CHD mortality, MACE, revascularization, stroke, CHF Niacin (alone) ↓MACE (no effect beyond statins) Fibrates ↓MACE Resins ↓MACE, CHD mortality Ezetimibe ↓MACE
Cholesterol-Lowering 4 S – Overall Survival Lancet 1994; 344: 1383
Cholesterol-Lowering 4 S – Secondary Endpoints Lancet 1994; 344: 1383
HPS
HPS Implication?
CHD Reduction in Chronic CHD Secondary Prevention Trials Statin Placebo/Comparator Achieved LDL-C, mg/d. L CHD Event Rate, % Patients 4 S 122 19. 4 190 28. 0 LIPID 112 12. 3 150 15. 9 CARE 98 HPS 89 8. 7 128 11. 8 IDEAL 81 9. 3 104 10. 4 TNT 77 6. 7 101 8. 3 Study 10. 2 135 What’s the NNT? 13. 2
IMPROVE-IT (N=18, 000) LDL-C and Lipid Changes Simva 40 vs. Simva 40/Ezetimibe 10 7 years’ F/U (!) Differences between groups Median 69 mg/dl Median 54 mg/dl LDL Total Chol Trig HDL hs. CRP -15 mg/dl -17 mg/dl -9 mg/dl +0. 5 mg/dl -0. 5 mg/dl NEJM 2015
IMPROVE-IT (N=18, 000) Primary Endpoint Cardiovascular Death, MI, Stroke, documented Unstable Angina requiring rehospitalization, or coronary revascularization (>30 days) Eze/Simva (N=9067) (N=9077) HR 95% CI P value 32. 7% 0. 94 (0. 89, 0. 99) 0. 016 34. 7% Kaplan-Meier event rates to 7 years Median follow-up 57 months Total patient years follow-up for primary endpoint = 80, 286 NEJM 2015
Event Reduction in Angiographic Trials % Stabilizing the Vulnerable Plaque Event Reduction % Stenosis (Niacin/ (Lovastatin/ (Diet/Resin) Triple Fluvastatin Colestipol) Therapy Circulation 87: 1781
Secondary Prevention LDL-Lowering vs PCI • Atorvastatin Versus Revascularization Treatment (AVERT) - Pts with stable CAD and LDL>115 - Atorvastatin 80 mg/day vs Angioplasty + Usual Care - Primary endpoint: Total ischemic events in 18 months
AVERT Cumulative Incidence (%) Time to First Ischemic Event Angioplasty / UC Atorvastatin p = 0. 027 Risk Reduction 36 % (95 % CI: 5 % - 67 %) Time Since Randomization (Years) NEJM, 1999; 341: 70
Have COURAGE! Medical Therapy Works for Stable CAD
Should We Raise HDL-C with Pharmacotherapy? • No!
AIM-HIGH Results (N=3500) NEJM 2011
HPS 2 -THRIVE (N=25, 000) ER niacin/laropriprant-simvastatin vs. simvastatin: No ASCVD event reduction vs placebo-simvastatin LDL-c -10 mg/d. L HDL-c +6 mg/d. L TG +33 mg/d. L P=0. 29 NEJM 2014
HPS 2 -THRIVE (N=25, 000) ER niacin/laropriprant-simvastatin vs. simvastatin: No ASCVD event reduction vs placebo-simvastatin NEJM 2014
Novel Targets for Intervention? • Homocysteine • Hormone replacement therapy • Antibiotics • Vitamin supplements X X
Primary Prevention
Primary Prevention Potential Targets for Intervention • Diet • Weight • Physical activity • Antiplatelet agents • Dyslipidemia • Blood pressure • Diabetes • Metabolic syndrome
Risk factor levels improved significantly, and similarly, with all diets
Take Home • De-emphasize dietary content (micronutrients) somewhat for weight loss • Focus on calories and find what works (substitution!) • Referral to dietician • Increase physical activity - Concrete recommendations, pedometer - Aim for vigorous, if possible • Set achievable goals - 1 lb/week glidepath - Soft landing • Motivational interviewing • Electronic media/m. Health technology
AHA Guidelines for Primary Prevention of CVD and Stroke Goal Recommended Intervention Risk factor Assess beginning at age 20 screening Update family history Goals: Adults Assess Et. OH, smoking, diet, should know physical activity at every visit levels and BP, BMI, waist, pulse (for AF) significance of at every visit (q 2 years) RFs as measured FLP and FBG q 5 yrs or q 2 routinely by PCP yrs if risk factors present
Primary Prevention - Lipids
CHD Outcomes in Clinical Trials of LDL Cholesterol-Lowering Therapy Rx No. of No. Trials Treated P-Y LDL Δ CHD Δ Surgery 1 421 4084 -22% -43% Resins 3 1992 14491 -9% -21% Diet 6 1200 6356 -11% -24% Statins 12 17405 89123 -20% -30%
Achieved LDL and Event Rates American Journal of Cardiology 2006 98, 1405 -1408 DOI: (10. 1016/j. amjcard. 2006. 039)
Achieved LDL and Event Rates American Journal of Cardiology 2006 98, 1405 -1408 DOI: (10. 1016/j. amjcard. 2006. 039)
Prevention Paradigm - Lipids • “The intensity of prevention efforts should match the absolute risk of the patient”
ASCVD Risk Estimator Search “ASCVD risk estimator”
4 Statin Benefit Groups • Clinical ASCVD • LDL–C >190 mg/d. L without secondary cause • Primary prevention/Diabetes: Age 40 -75 years, LDL– C 70 -189 mg/d. L • Primary prevention/No Diabetes: Age 40 -75 years, LDL–C 70 -189 mg/d. L, ASCVD risk ≥ 7. 5%* * Requires risk discussion with clinician before statin prescription. Statin therapy may be considered if risk decision is uncertain after use of ASCVD risk calculator.
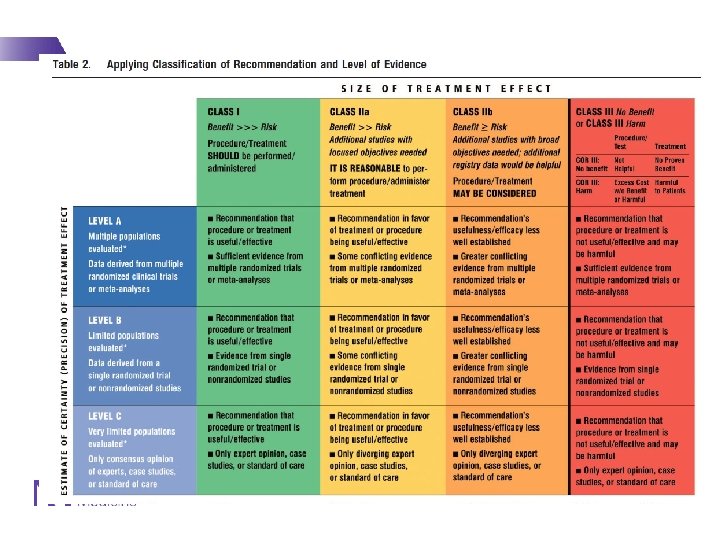
Major recommendations for initiating statin therapy - 1 IA IA IB IA IIa. B 1
Major recommendations for initiating statin therapy - 2 IIB
Men >50 Women >60 LDL <130 CRP >2
JUPITER - Results At 2 Yrs: 44% RRR 1. 36/100 p-y vs. 0. 77/100 p-y NNT 100 -150
JUPITER - Results FRS <10% 10 -20% >20% HR Pintxn 0. 67 0. 95 0. 49 0. 70 RFs <2 ≥ 2 HR Pintxn 0. 91 0. 03 0. 51
Primary Prevention - BP
Prevention Paradigm - BP • “All high BP is bad; treat all high BP”
2013 European HTN Guidelines Eur J Hypertens 2013; 31(7): 1281 -1357
2013 European HTN Guidelines Eur J Hypertens 2013; 31(7): 1281 -1357
Progression of BP-Lowering Trials • Started with very high DBP 1960 s • Then moderately high DBP • By 1980 s, epidemiological data suggested SBP was more important • Isolated systolic hypertension trials – 1991 -1999 64 2/20/2021
% Risk Reduction Meta-Analysis: SHEP, Syst-Eur, Syst-China All CV CV Mortality Events -17% -25% -32% Stroke CHD -37% -25% . . . and 50% reduction in CHF in SHEP! Lancet 2000: 355: 865
NNT for 5 Years to Prevent 1 Event CV Event Stroke CHD All pts 26 48 64 Men 18 34 44 Women 38 68 92 Age 60 -69 39 99 89 Age 70+ 19 32 50 Staessen, Lancet 2000: 355: 865
Meta-Analysis of HTN Rx in People >80 Total Mortality CVD Death All CVD RR (%) with Rx Stroke N=1670 participants >80 years old Adapted from Gueyffier, Lancet 1999 and Elliott, Hypertension 2004 CHD CHF
Hypertension in the Very Elderly Trial (HYVET) Design • International multicenter trial • Ppts ≥ 80 yo with HTN - SBP 160 to 199 mm Hg - SBP after standing 2 minutes ≥ 140 mm Hg • Randomized to indapamide 1. 5 mg qd vs. placebo - Target BP <150/<80 mm Hg - Could receive perindopril (2 or 4 mg qd) or placebo • Primary endpoint: Fatal or non-fatal stroke - Secondary endpoints of interest: • Total mortality, CVD death, cardiac death, stroke death, fatal/NF heart failure NEJM 2008; 358: 1887
HYVET Results • 3845 ppts - Mean age 83 years (range 80 -105) - 61% women; 12% with prior CVD - Baseline BP: 173/91 - Mean duration of F/U: 2 years (0 to 6. 5 years) • Terminated early for significant reductions in primary endpoint and all-cause mortality NEJM 2008; 358: 1887
HYVET BP 14. 5/6. 8 BP 29. 5/12. 5 NEJM 2008; 358: 1887
HYVET – Primary Endpoint 17. 7/1000 p-y 12. 4/1000 p-y 30% RRR; NNT 94 over 2 years NEJM 2008; 358: 1887
HYVET – Total Mortality 59. 6/1000 p-y 47. 2/1000 p-y 21% RRR; NNT 40 over 2 years NEJM 2008; 358: 1887
HYVET – Heart Failure 14. 8/1000 p-y 5. 3/1000 p-y 64% RRR NNT 52 over 2 years NEJM 2008; 358: 1887
SPRINT Trial 74 2/20/2021
SPRINT Trial • Randomized 9361 ppts 50 y and older with SBP ≥ 130 - Had to have CVD, increased risk for CHD or have CKD - Randomized to target of <140 vs <120 - Took 2 meds vs 3 meds to achieve targets on average • Stopped early for benefit • Rates of CVD (CHD, HF, stroke) reduced by 30%! • Rates of total mortality reduced by 25%! • Data eagerly awaited –Event rates? In whom?
SPRINT Trial
SPRINT Trial No interactions across subgroups Some significant adverse events: - Hypotension, syncope, AKI, electrolyte abnl
Ancillary Treatment to Reduce Risk in HTN • Comprehensive Lifestyle Modification • ASA - HOT Trial: 36% reduction in MI with ASA 75 mg / day • Statins
Ancillary Treatment to Reduce Risk in HTN • Comprehensive Lifestyle Modification • ASA - HOT Trial: 36% reduction in MI with ASA 75 mg / day • Statins
ASCOT-LLA • 19342 patients enrolled in a trial of newer vs older anti-HTN agents • 10305 with total cholesterol 250 - Mean baseline TC 213 - Stopped early after 3. 3 years • Results - 36% RRR in fatal CHD/NFMI - 21% RRR in total CVD - 27% RRR in stroke
ASCOT-LLA
Primary Prevention - Diabetes
CVD Prevention in Diabetes • Elevated blood sugar increases risk for CVD (all types) • RFs cluster, especially in DM, increasing risk • Diabetics are at high risk, and have worse outcomes when they have an event • Treatment of blood glucose does not effectively reduce macrovascular ASCVD events; just microvascular complications • Focus is on treating other RFs aggressivelt (BP, lipids, weight)
CARDS Study Lancet 2004
CARDS Study 120 mg/d. L <120 mg/d. L Lancet 2004
Reduction of Endpoints in DM Tight Glucose Control vs BP Control Bakris, Arch Intern Med 2001
Benefit in stroke outcome more than outweighed by adverse events
Empagliflozin and CVD Outcomes …But not MI or stroke alone 88 2/20/2021
Questions? 89 2/20/2021