CAUSES OF THYROTOXICOSIS WITH INCREASED THYROID SECRETION Graves




- first described (1825) Named after Robert Graves(1835)")








 Hair loss Pretibial myxoedema Gynaecomastia Audible bruit")



 {severe} diplopia Optic n. damage blindness (decreasing visual")
,")

 • Thyroid antibodies are elevated • A I 123 radionuclide scan")













 • Pregnancy • suspicious nodule in graves glands • Large toxic nodular")










 • Oxygen • Glucose infusion")


- Slides: 51
CAUSES OF THYROTOXICOSIS WITH INCREASED THYROID SECRETION • • • Graves disease Toxic nodular goitre Toxic thyroid adenoma Jod basedows hyperthyroidism Secondary hyperthroidism due to TSH Thyroiditis WITHOUT INCREASED THYROID SECRETION • • Factitious hyperthyyroidism Struma ovarii Molar pregnancy Rare metastatic thyroid ca.
PRIMARY THYROTOXICOSIS • The goitre is diffuse and vascular, large or small, firm or soft, • Thrill and a bruit may be present. • The onset is abrupt. • Hyperthyroidism is usually more severethan in secondary thyrotoxicosis but cardiac failure is rare. . SECONDARY THYROTOXICOSIS • the goitre is nodular. • The onset is insidious • may present with cardiac failure or atrial fibrillation. • hyperthyroidism is not severe. • Eye signs other than lid lag and lid spasm (due to hyperthyroidism) are very rare.
PRIMARY THYROTOXICOSIS
GRAVES DISEASE q. The commonest form of thyrotoxicosis q More prevalent in young adults q 6 times more
HISTORY Caleb Parry(Welsh phy. )- first described (1825) Named after Robert Graves(1835)
AETIOLOGY • • Genetic factors Association with other autoimmune diseases • Association with HLA DR 3, B 8, BW 35, BW 46 • Emotional uphaevals • Consumption of iodine excess Use of thyroid hormone
PATHOLOGY & PATHOGENESIS • Autoimmune disorder • Thyroid stimulating Igs produced against antigen in thyroid • Appear to be directed against TSH receptors TRAbs
THEORIES • Defect in suppresssor Tcells-allows helper T cells to stimulate TSI from B cells • Another theory is that an immune response is launched to altered antigens on the follicular cell surface
PATHOLOGY MACROSCOPY • Diffuse and smoothly enlarged • Vascularity incresed
MICROSCOPY • Hyperplastic columnar epithelium, pappilary projections. • Nuclei exhibit mitosis • Aggregates of lymphoid tissue • Vascularity increased • Minimal colloid
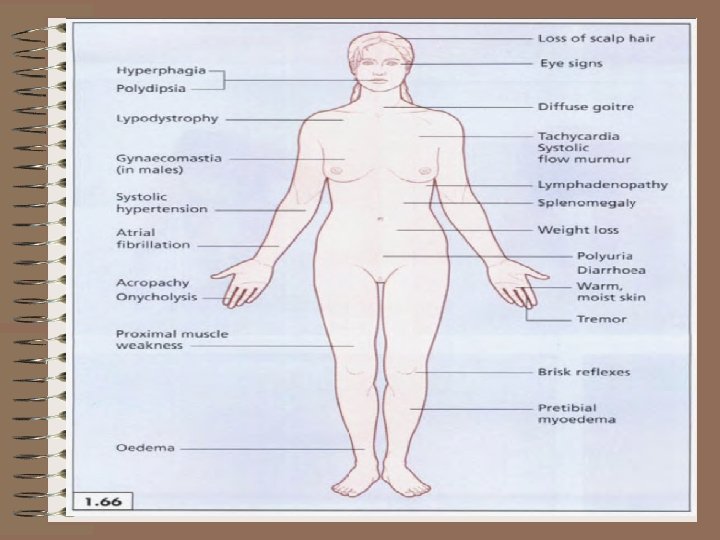
CLINICAL FEATURES • • • Heat intolerance Increased thirst Sweating Weight loss Menustrual irregularities Emotional liability Shortness of breath Fatigue Prominent eyes Diarrhoea Goitre Hair loss and pruritus
SIGNS • Tremor • Warm moist skin • Tachycardia, AF, widened pulse pressure • Heart failure • Myopathy(proximal) • Hyper active tendon reflexes
FEATURES SPECIFIC TO GRAVES DISEASE Thyrotoxicosis Exophthalmos Goitre Classical triad
Other features Onycholysis(thyroid acropathy) Hair loss Pretibial myxoedema Gynaecomastia Audible bruit
THYROID OPHTHALMOPATHY • Spasm of upper eyelid with retraction and lid lag • External ophthalmoplegia • Exophthalmos with proptosis • Supra orbital and infraorbital swelling • Congestion and oedema of conjunctiva
Pathogenesis • cross-reaction of the thyroid antigen and ocular muscle antibodies is apossible explanation
Histologically, • Diffuse lymphocytic infiltration of the retro-orbital tissues occurs, • Fibroblast activation with glycosaminoglycan (a mucopolysaccharide) production leading to edema and fibrosis.
OPHTHALMOPATHY Protrusion opthalmoplegia (elevators are involved) {severe} diplopia Optic n. damage blindness (decreasing visual acuity Impaired colour vision) MALIGNANT EXOPHTHALMOS
Exophthalmos…. . • result of increased retro-orbital tissue • assessed with an exophthalmometer (Hertel), [which measures the distance from the lateral bony orbital margin to the anterior surface of the cornea. ]
DIAGNOSIS A cost-effective work-up can include • extensive history • physical examination, Thyroid function tests. • elevated levels of T 3 and T 4 , • a decreased or undetectable level of TSH should be demonstrated.
DIAGNOSIS (CONTD. ) • Thyroid antibodies are elevated • A I 123 radionuclide scan demonstrate diffuse uptake throughout an enlarged gland. • An ultrasound or computed tomography (CT) scan of the neck may be used to evaluate clinical landmarks).
TREATMENT STRATEGIES • Reducing functional mass of thyroid tissue by removal of large part of the gland • Destruction of most of the gland by I 131 • Anti thyroid drugs to decrease seretion • Drugs that block beta adrenergic receptors
ANTI THYROID DRUGS • PROPYL THIOURACIL • METHIMAZOLE , CARBIMAZOLE • MECH. OF ACTION • Inhibit organic binding of thyroid iodine and also inhibit coupling • PTU also inhibit peripheral conversion of T 4 to T 3 • PTU is said to decrease thyroid antibody level
SIDE EFFECT • Rash, fever , peripheral neuritis, polyarteritis, granulocyt openia, agranulocytosis, arthritis liver dysfuction PREGNANCY • Drug cross plancetae and also secreted in breast milk – PTU is preferred drug
DOSE • PTU 100 -300 mg tds • Methimazole 1030 mg tds ; then OD
BETA BLOCKERS • Hyperdynamic adrenergic effect of thyrotoxicosis are alleviated. • Decrease peripheral conversion • Reduce heart rate , control tremor , agitation • Not effective as sole mean of therapy as hyper metabolism and weight loss continue • Usually preferred - propranalol • May ppt heart failure and asthma
RESULTS • Improved symptom by 2 wks • Euthyriod by 6 wks • Given 12 – 18 months [relapse 50%] • Thyroxine can be added to prevent hypothyroidism
RADIOACTIVE IODINE SUITABLE PATIENT • Small or medium sized goitre • Relapse after medical or surgical therapy • Contraindication to antithyriod drug or surgery
CONTRAINDICATION ABSOUTE • Pregnancy • Breast feeding RELATIVE • Thyroid opthalmopathy • Isolated thyroid nodule • Toxic nodular goitre • Young age
ADMINISTRATION • Should be euthyroid before I 131 • Stop all anti thyroid drugs 2 -3 wks prior for uptake • A drink of I 131 sodium iodide • Initial dose is about 10 mci of I 131
ADMINISTRATION • After std. treatment- euthyroid within 2 months. Some become hypothyroid • Long term follow up –hypothyroidism and recc. Hyperthyroidism may aggravate ophthalmopathy
COMPLICATIONS • Exacerbation of thyrotoxicosis • Overt thyroid storm • Hypothyroidism • Risk of foetal damage in pregnancy • Worsening of eye signs • Hyperparathyroidism
ADVANTAGES • Avoidance of surgery DIADVANTAGES • Hypothyroidism • Overall treatment cost is less • Adverse effect on opthalmopathy • Treatment ease Reccurent thyrotoxicosis is managed by radioiodine because reoperation carries higher morbidity
SURGERY INDICATIONS • Intolerance or non compliance with anti thyroid drugs • When radioiodine is contraindicated • Young patients • Graves optthalmopathy
Indications(contd. ) • Pregnancy • suspicious nodule in graves glands • Large toxic nodular goitre with low I 131 uptake • Very large goitre and severe thyrotoxicosis at initial presentation
RISKS • R. L. N. injury • Hypoparathyroidism • Permanent hypothyroidism
PREOPERATIVE PREPERATION • Thyrotoxicosis is controlled medically -better nutritional state - provides normal homeostatic mechanisms and responses to stress of operation • Wait for 2 months after euthyroid-other wise more chance for thyroid storm • Treated with lugols iodine for 10 days prior to operation to decrease the vascularity of the gland
Preferred surgery TOTAL THYROIDECTOMY • Low chance for relapse but more chance for nerve damage and hypoparathyroidism SUBTOTAL AND NEAR TOTAL THYROIDECTOMY • Higher chance for relapse lesser complications
COMPLICATION • • • Hoarseness of voice Hypoparathyroidism Infection Air embolism Thyroid storm
ADVANTAGES • Immediate cure • Decreased long term incidence of hypothyroidism • Decreased op visits • Potential removal of a carcinoma DISADVANTAGES • All complications • Haematoma • Hypertrophic scar
TREATMENT OF EXOPTHALMOS • Severity is independent of thyrotoxicosis • Treatment is directed to prevent infection and reduce periorbital swelling • High dose systemic corticosteroid (prednisolone 60 mg) • Retrobulbar injection of depot steroids
• SURGICAL INTERVENTIONS • Lateral tarsoraphy • Orbital decompression • Cryosurgical rduction of pituitary OTHERS • Radiation therapy with steroids • Plasma exchange therapy • Immunosupppressants-cyclosporine, azathioprine
THYROID STORM • Rarely during thyroidal or other surgery PRECIPITATING FACTORS • Infection, labour, administaration of iodine, after treatment with I 131
• MANIFESTATIONS • Hyperthermia, tachycardia, intense irritability, profuse sweating, hypertension, extreme anxiety, prostration, hypotension and death • All are adrenergic phenomenon • Caused by adrenergic outburst in a sensitised patient by thyroid hormone induction
MANGEMENT • Best management –prophylaxis • Patients with toxicity should be made euthyroid before operation. TREATMENT • Fluid replacement • Lugols iodine • Hydrocortisone (cortisol beakdown is increased) • Cooling blanket avoid aspirin
• Reserpine and guanethidine (sympatholytic treatment) • Oxygen • Glucose infusion
SUMMARY • Thyrotoxicosis can be primary or secondary • Graves disease is the most common type • It is an autoimmune disorder • Classical triad – goitre, thyrotoxicois, exophthalmos • Investigations-T 3 , T 4, TSH, thyroid antibodies
• Treatment options are –drugs, radioactive iodine, surgery • Over 45: radioiodine. Under 45: surgery for the large goitre, antithyroid drugs for the small goitre. • Thyroid storm is an adrenergic outburst in a sensitised patient which is better prevented than treated