Peptic Ulcer Disease Cengiz Pata MD Dept Gastroenterology






 Systemic mastocytosis Basophilia")
")











 20% no warning")




 Specificity (%) Histology")










")
 • Perforation (2 3%) •")




, Pancreas (40 80%) Pituitary (30 60%) •")





















- Slides: 67
Peptic Ulcer Disease Cengiz Pata, MD Dept. Gastroenterology, Yeditepe University, Medical center
Case • 30 year old male • Epigatsric pain radiating to the back Questions? Possible diagnosis Deferential diagnosis Possible complications
Case • Pain: • What type of pain? How often? Awakes at night? Relation to food? • Complications: • Vomiting? (obstruction? ) Stools? (melena? ) • Common deferential diagnosis: • Pnacreatobiliary disease Dyspepsia Tumors
Case • Next diagnostic step? • Endoscopy Abdominal US UGI? • DU Ulcer detected next step? • Test for H. pylori Exclude NSAID use Rare – assess gastrin, mainly in unusual cases
(Benign gastric ulcer (B
Peptic Ulcer • A defect in the gastrointestinal mucosa extending through the muscularis mucosa. • Two main forms: 1) Helicobacter associated 2) NSAID associated ( Steroids alone – no additional risk, Increased risk when combined with NSAIDS)
Peptic Ulceration : Additional Causes • Acid hypersecretion: Gastrinoma ( ZE) Systemic mastocytosis Basophilia in myeloproliferative disorders • Viral Herpes simplex CMV ( mainly in immune compromised)
Peptic Ulceration : Additional Causes • Vascular Insufficiency ( including due to crack cocaine) • Radiation induced • Chemotherapy induced • Stress ulceration
Electron micrograph of H. pylori
Prevalence of Helicobacter pylori in peptic ulcer
Seroprevalence of H. pylori with increasing age in developed and developing countries 100 Developing countries Developed countries 64 96% Prevalence (%) 75 10 75% 50 7 54% 6 39% 25 0 <20 40 50 Age range (years) Adapted with permission from Heatley-Helicobacter pylori and Gastrointestinal Disease; Oxford, UK: Blackwell Scientific Publications
Risk factors for H. pylori infection • Age • Country of origin • Socio economic status poor housing bed sharing overcrowding large families
Modes of transmission of H. pylori infection • Zoonosis unlikely • Environment unlikely • Person to person oral likely gastro oral likely faecal oral likely
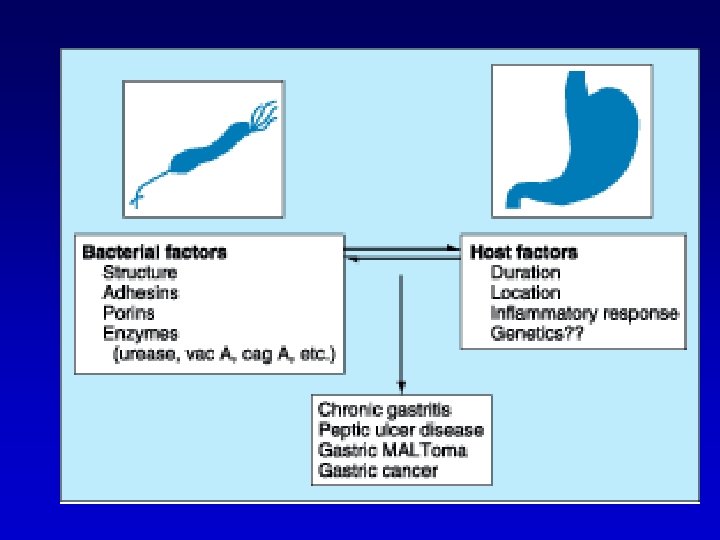
H. pylori infection and disease associations • Chronic gastritis • Duodenal ulcer • Benign gastric ulcer • Gastric carcinoma • Gastric MALT and non Hodgkin‘s lymphoma • Ménétrier‘s disease
Pattern of gastritis Duodenal ulcer Gastric ulcer Corpusitis * Antral gastritis *H. pylori colonizes areas of gastric metaplasia, leading to chronic duodenitis and eventually duodenal ulcer.
NSAIDS • • • In the USA 30 bil OTC 20 mil prescriptions 3 4% ulcerations 20, 000 die of NSAID complications 80% have no preceding dyspepsia Important to identify at risk populations Previous gastritis Elderly
PD & Systemic Diseases • COPD • Renal Failure • Cirrhosis • Mastocytosis
Clinical Presentation • Abdominal Pain: Epigastric dull “hunger pain” DU 11/2 – 3 hrs postprandial relived by food May awake at night GU – May occur with meals • nausea weight loss more frequent in GU • Sudden pain – perforation? • Vomiting – obstruction?
Clinical Presentation • • Physical examination: Poor predictive value, not specific Pain may occur in RUQ ~ 20% Detect complications: Tachycardia, orthostasis bleeding? Radiation to the back perforation? Succussion splash – outlet obstruction?
Complications • Bleeding ~ 15% ( More in >60 yrs –NSAID) 20% no warning sign • Perforation 6 7% Free Penetration: DU posterior to pancreas GU into Lt hepatic lobe Gastrocolic fistula
Complications • Outlet obstruction 1 2% Inflammatory – reversible by Tx Scar tissue – balloon dilatation, Surgery • Presentation : Gradual onset Sudden
Clinical manifestations of ulcer disease
Differential Diagnosis • • Non ulcer dyspepsia Tumors of the UGIT Biliary disease Reflux disease Vascular diseases Pancreatitis Coronary heart disease
Diagnosis • Radiology: Single contrast 80% sensitivity Double 90% (worse for ulcers<0. 5 cm, scar tissue) • Endoscopy: examination of choice good for small ulcers biopsy samples for HP and malignancy therapeutic • Assay for HP infection
Diagnostic methods for H. pylori Diagnostic method Main indication Sensitivity (%) Specificity (%) Histology Diagnosis 90 90 Culture H. pylori antibiotic sensitivities 80 90 95 Rapid urease test Endoscopy room diagnosis 90 90 Serology Screening and diagnosis 90 90 Urea breath test To confirm eradication 95 100
The principle of the urease test NH 2 C O + 2 H 2 O + H+ Urease 2 NH 4+ + HCO 3 NH 2 Urea CLOtest p. H change
The principle of the 13 C- or 14 C-urea breath test Reproduced with permission from Mr Phil Johnson, Bureau of Stable Isotope Analysis, Brentford, UK.
Therapy • Treat H. pylori • Healing by inhibition of acid secretion: H 2 receptor antagonists (H 2 RA) Proton Pump inhibitors ( PPI) Anti Acid • Cytoprotection Sucralfate Anti Acid Bismuth Based Prostaglandin Analogs
Therapy of DU • H 2 RA – Cure in 80% at 4 wks ~95% at 8 wks Split and once daily equally effective • PPI Cure in 60 93% at 2 wks 80 100 % at 4 wks • Omeprazole Vs ranitidine 14% advantage at 2 wks 9% advantage 4 wks
Therapy of GU • Suppress acid by H 2 RA or PPI • Advantage of PPI less apparent • Sucralfate comparable to H 2 RA • Prepyloric ulcers may resemble more DU in terms of response to acid suppression
Risk stratification of Ulcer Pts • Low risk: Intermittent symptoms Nonsmoker Discontinued NSAID Uncomplicated Easy healing
Risk stratification of Ulcer Pts • High risk: Frequent recurrence Refractory to Tx Smoking Continued NSAID Giant Ulcer ( DU >2 cm GU > 3 cm) Anticoagulation Deformity & scarring Elderly Acid hypersecretion
General Scheme • • • HP positive – Eradicate If Non complicated – No further Tx If high risk: Follow by acid suppression for 4 6 wks Withdraw – NSAID Smoking Excess Alcohol • In GU – Biopsy? Cost and effect Most CAs detected in first round of endoscopy
Refractory Ulcers • Consider refractory after 8 12 wks of Tx • Ensure that refractory symptoms = refractory ulcer ( endoscopy ( • If no ulcer investigate pain • Consider “silent” refractory ulcer in high risk pts ( ~25% of refractory ulcers(
Refractory Ulcers causes • • • Persistent HP infection Persistent NSAID use Poor pt compliance Giant ulcers ( healing at 3 mm/wk) Smoking Under laying pathology ( ZE, bands, crohn’s, infections I. e. TB syphilis, Ly, scarcoidosis ) • Impaired response to PPI ( 5% of population)
Refractory Ulcers Approach • Seek causes: DU HP, NSAIDS, r/o ZE ( gastrin levels) GU main concern CA Repeat multiple Bx Evidence for malignancy: CT, EUS No explanation surgery
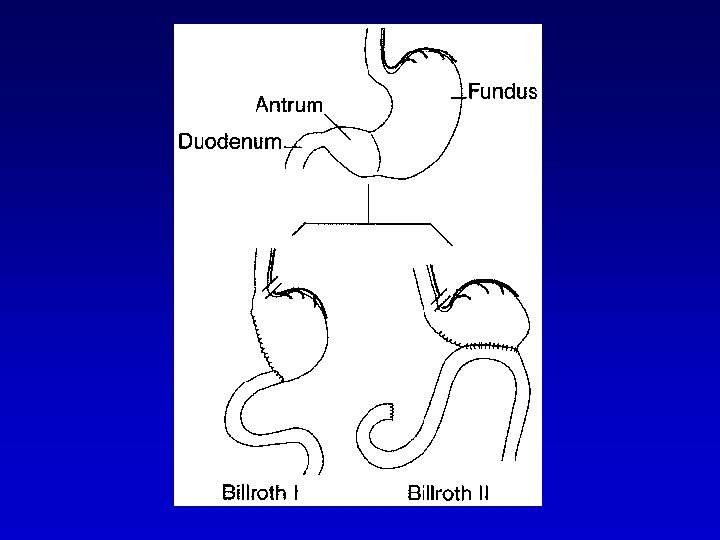
Surgery DU • Refractory bleeding (~5% of transfused Pts) • Perforation (2 3%) • Outlet obstruction • Vagotomy + antrectomy Rec. (1%) Comp Vagotomy + pyloroplasty intermediate (10%) Highly selective vagotomy Rec. Comp
Zollinger Ellison Syndrome • Severe peptic ulcer diathesis + gastric acid hypersecretion due to b cell endocrine tumor • 0. 1 1% of PUD patients • Sporadic, or associated with MEN type I (25%)
Zollinger Ellison Syndrome • 80% Localized to <gastrinoma triangle: cystic & common bile ducts, duodenum, junction head and body of pancreas. • % 60 malignant, up to 50% with metastasis • Clinical: PUD >90% (recurrent, multiple, refractory, complicated (
Zollinger Ellison Syndrome • Esophageal complaints ~60% • Diarrhea ~50% (fluid overload, pancreatic enzyme dysfunction, epithelial dysfunction) • Combination should raise clinical suspicion
Clinical features of Zollinger Ellison syndrome
MEN I • Autosomal Dominant: Parathyroid (~90%), Pancreas (40 80%) Pituitary (30 60%) • Contributory effect of hyperparathyroidism, hypercalcemia hypergastrinemia acid secretion • Higher incidence of carcinoids • Smaller and multiple duodenal gastrinomas
Diagnosis of Gastrinoma • Combination of clinical signs • Fasting gastrin levels (> 150 pg/ml ( • Avoid confounding factors (hypochlorhydria, PPIs, outlet obstruction, renal failure ( • Assess acid secretion (if low excludes( • Provocative tests (calcium, secretin(
Treatment • Localization (EUS, Oct scan, MRI, CT( • Exclusion of metastasis • If positive – symptomatic cure • If negative attempt surgical resection ( less likely in MEN I ~ 6% (
Case 2 • 70 year old lady , RA • Dizziness and weakness for the last week. • Mild abdominal pain • Questions?
Case 2 • • • Stools? Melena Drugs? NSAIDS Next action? Gastroscopy
Gastric Ulcer with Stigma
Treatment • H 2 RA • Oral PPI + H 2 RA • IV PPI
H 2 RA • Very safe drugs • Tolerance after 48 hrs IV treatment • Less effective than PPIs in suppressing acid secretion (block only histamin(
Treatment • Heavy consumption of NSAID • Should H. pylori be tested for? Treated? • YES
Drugs for treatment of acid disorders and H. pylori infection • H 2 Receptor antagonists • PPI • Anti H. pylori regimens
Overall Control of Acid Secretion
The parietal cell
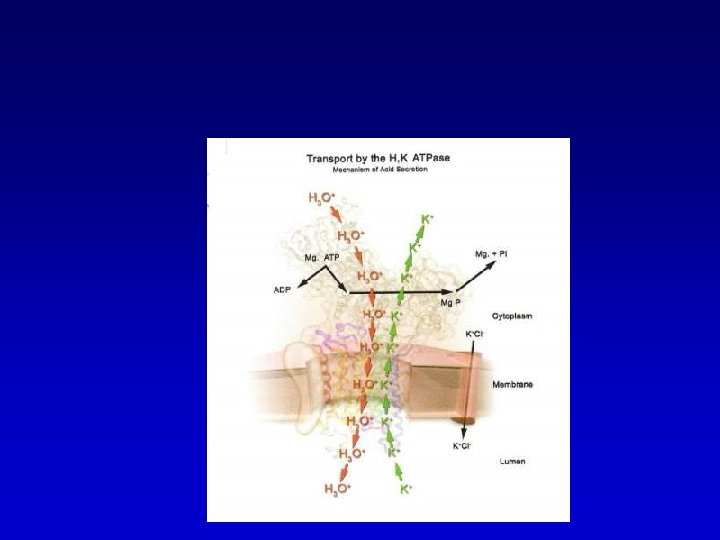
The proton pump
Biologic mechanism of action of substituted benzimidazoles ((proton pump inhibitors
Kinetics of PPI Effect
Summary of PPI effects • Inhibit ~70% of acid secretion • Need to coordinate pump activation & PPI availability (t/2~60 90 min) • Pump re synthesis (half life ~ 50 hours 25% synthesis between single day doses) • Cysteins accessible to reducing activity of glutathione • Spontaneous pump recycle every 60 120 min (Potential to block)
Optimization of acid control
Guidelines for use of antibiotic therapy in patients with Helicobacter pylori infection
Treatment regimens for eradication of Helicobacter pylori
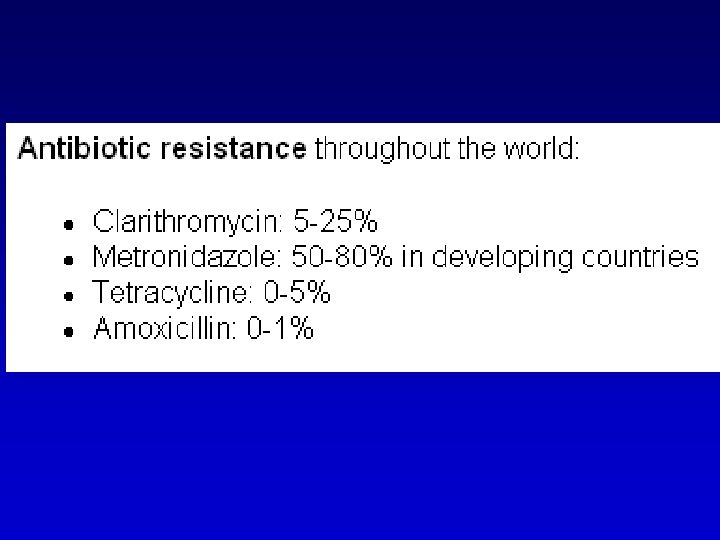
Therapeutic options clarithromycin a 90 tio % nr ic ad er _ eradication rate >80% < _ 2 x 400 500 mg PPI X 2 te ra n io at ic 90% < metronidazole ad at er e 2 x 250 500 mg amoxycillin 2 x 1000 mg
Choice between treatments
Treatment failures