Peptic Ulcer Wendy Langen Peptic Ulcer Disease PUD










 with collapse, vomit, • Rigid abdomen,")



, or fecal antigen test (S&S>70%) or")







 Early Diagnosis")

- Slides: 32
Peptic Ulcer Wendy Langen
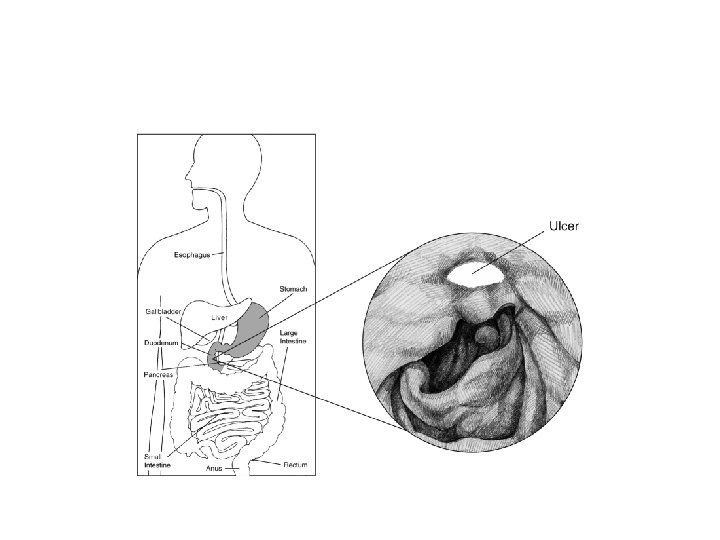
• • Peptic Ulcer Disease= PUD Refers to ulcers of stomach or duodenum Prevalence 10% USA in 96 Am J Public Health 1996 Feb; 86(2): 200 Gastric> duodenal
Ulcer Sx • Gnawing, burning epigastric pain radiating to back • Duodenal- 2 -5 hours post-prandial or with empty stomach, or at night • Peptic- may be worsened with food, feeling of fullness, aggravation with fatty food, even N/V • Relieved with antacids and antisecretories
Risks • • H. pylori NSAIDs list GERD Smoking Crohn’s, CMV Steroid use Bisphonates, chemo http: //www. dynamed. com/topics/dmp~AN~T 116374/Peptic-ulcer-disease#General-Information • Not coffee, nor etoh! http: //www. ncbi. nlm. nih. gov/pubmed/23776588? dopt=Abstract, Neth J Med 2001 Jul; 59(1): 23
DDx • • • GERD Acute upper GI bleed Gastric CA IBS Pancreatitis • Cholecystitis
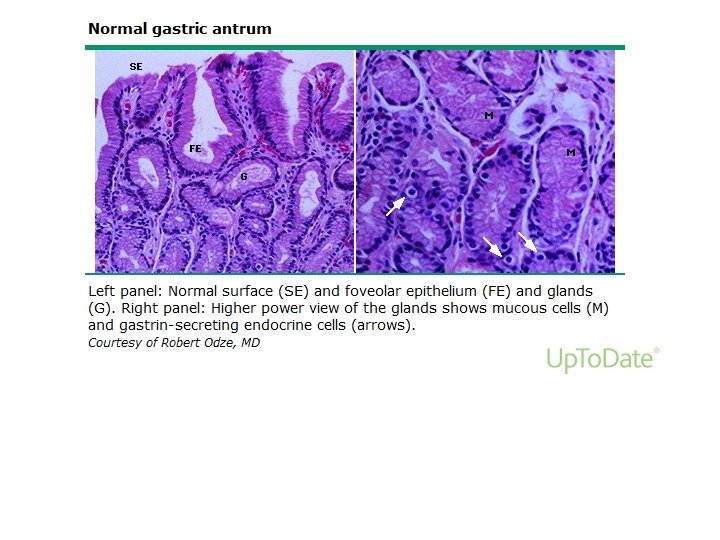
Evaluation • Ask about NSAIDs, diet, weight loss • Signs of shock- HR, BP, pallor • Abdomen- rigid, tender, rebound, hypoactive BS • Rectal Blood • CBC, breath urea, LFTs, lipase • Endoscopy can Dx, biopsy gastric ulcers
Complications • Bleeding • Perforation • Gastric outlet obstruction- suspect CA
Actively bleeding from ACP
Clotted
Ready to rebleed
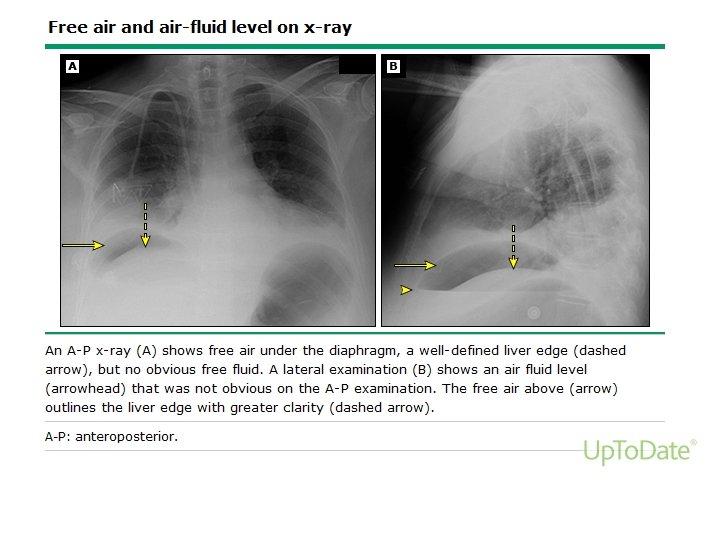
Ulcer perforation • Sudden extreme pain (to shoulder) with collapse, vomit, • Rigid abdomen, cold extremities, pale face • Improvement in 2 hours, but abdomen remains rigid, tympany over liver, free air seen in plain film • Then “catastrophe” in 6 -12 hours- peritonitis, shock, death
Free air after perforation
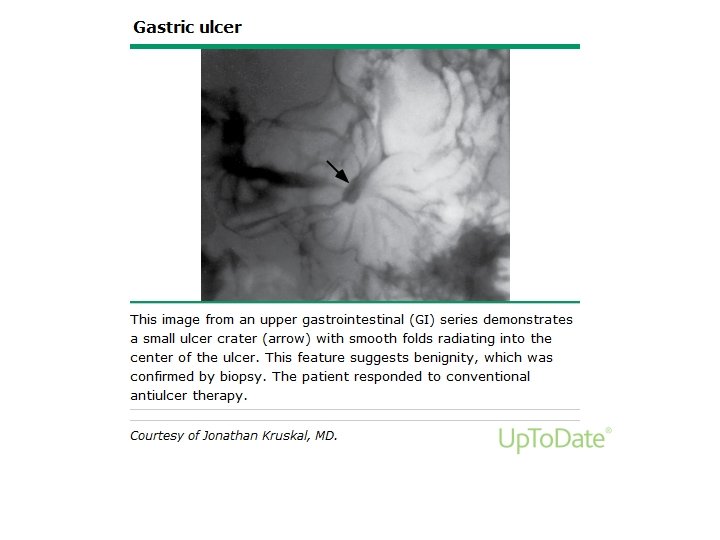
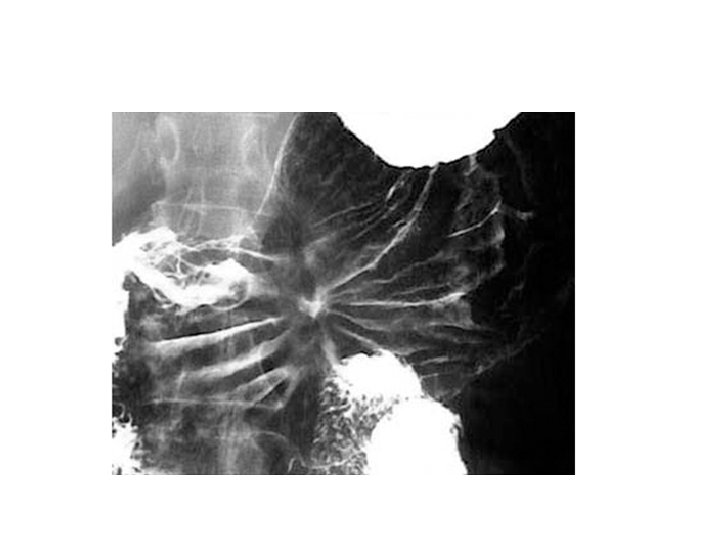
Diagnosis of Ulcer • Contrast imaging can show ulcer • H. pylori test and treat. • Endoscopy definitive Dx, but often unnecessary
This case • Peptic ulcer most likely given NSAIDs use, Hx GERD, gnawing pain worse at night • Peptic ulcer more likely with smoking, NSAIDs
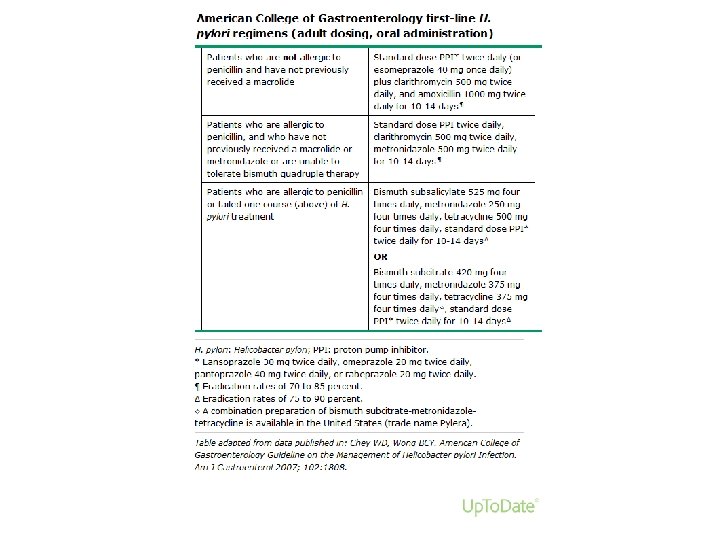
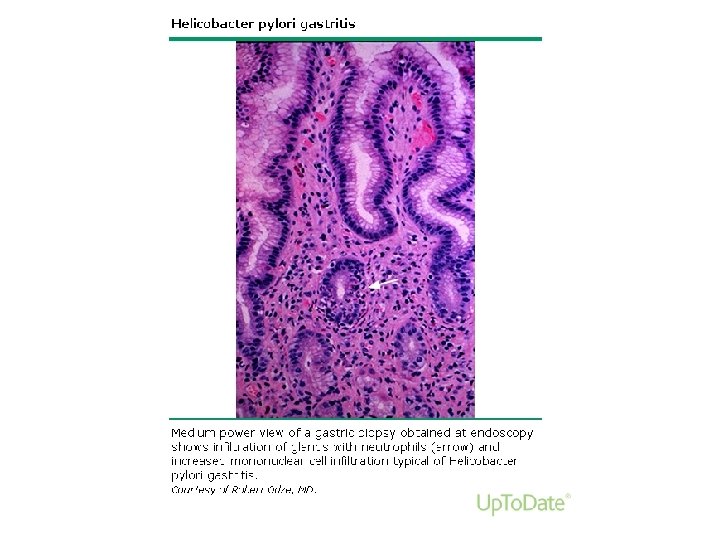
H. Pylori testing • Breath urea test (S&S>90%), or fecal antigen test (S&S>70%) or serology (S&S>60%), No PPIs • My obviate need for endoscopy if Sx match peptic ulcer and H. pylori is positive. (NIHCare. Excellence recommendation) “test and treat” • Retesting (serology) is most consistent recommendation, but some find no evidence to support retesting, and they should not be on PPI
H. Pylori test and treat • Unless “alarm” features: • “bleeding, anemia, early satiety, unexplained weight loss, progressive dysphagia, odynophagia, recurrent vomiting, family history of gastrointestinal cancer, previous esophagogastric malignancy” (Upto. Date)
Biopsy • Gastric ulcers, which can be malignant • Not duodenal, unless Crohn’s • Biopsy can include urease testing for H. pylori (S&S>90%), which is cheaper than histology
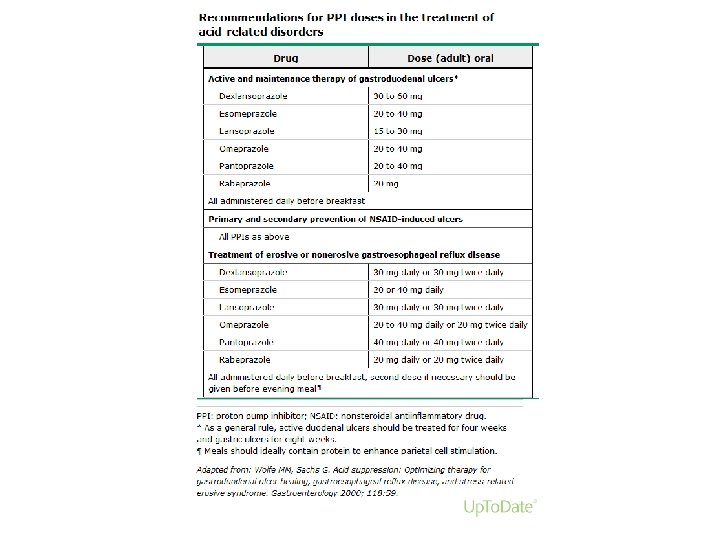
PUD treatment • If H. pylori, treat • Stop NSAIDs • Antisecretory therapy
Maintenance PPI in some • • • Giant ulcer Refractory ulcer Still H. pylori Recurrent disease NSAIDs
Re-endoscopy “Surveillance” Endoscopy if: • Bleeding, • Persistent symptoms, • Gastric ulcer without NSAIDs nor H. pylori
Osteoarthritis • X-ray can confirm, Ortho can replace joints • Lose weight – Stop etoh – walk – improve diet, – eat breakfast, lunch • Acetaminophen
Control BP, screen • At least BP check within a week • Up lisinopril from 10 to 20 mg is best choice, with BP check in 2 weeks • This patient needs a flu shot, Mammogram and pap smear
References • Upto. Date • Dynamed- as indicated • Cope, Z. (1957) Early Diagnosis of the Acute Abdomen. 19 th Edition, NY: Oxford University Press
OCPs or Pt ed • Everyone, • Give an OCP of this case to a peer • Convince a patient (peer) to follow the instructions given for this patient – Stop NSAIDs – Start PPI – Walk, exercise – Diet, lower etoh