Esophageal Tumors Cengiz Pata Gastroenterology Yeditepe University Istanbul

Esophageal Tumors Cengiz Pata Gastroenterology, Yeditepe University, Istanbul

Bening esophagial tumors l l l l l Leiomyoma Hemangioma Granuller cell tumor Congenital cell tumor Fibrovasculer polyp Bronchogenic cyst Eosinophilic granuloma Lymphangioma Squamose cell papilloma lipoma

epidemiology 60 -70 years l 4/1 towards to men l 5 -10/100. 000 l 7. ca mortality in men l Squamose cell carcinoma(80%), adenocarsinoma, sarcomas, lymphoma, malignt melanome l

etiology Squamose Ca l Alchol, tabacco l Nitrosemanine l Radiation l Achalasia l Tylosis l Plummer Winson syndrome l Radiation l HPV Adenoca l Baret’s (5% malignancy) l GERD (85% baret’s) l Obesity l Scleroderma

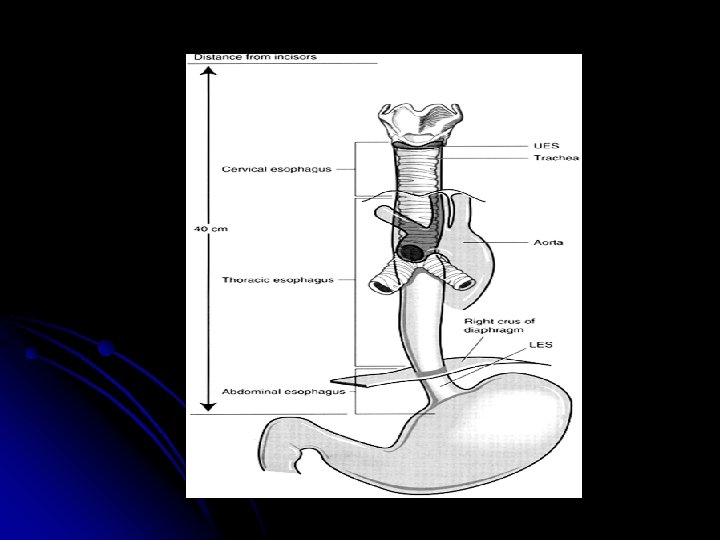
Clinacal presentation l l l l l 1/3 upper esophagus 15%, middle 50% Progressive dysphagia (firstly solid) Odynofagia Back pain Anorexia Weight loss Regurgitaion Voice change Aspritaion/pnomonia hematemesis
 l Small")
prognosis >5 cm involvement l Lymph node metastas (5 year survival %20) l Small cell, malign melanoma l

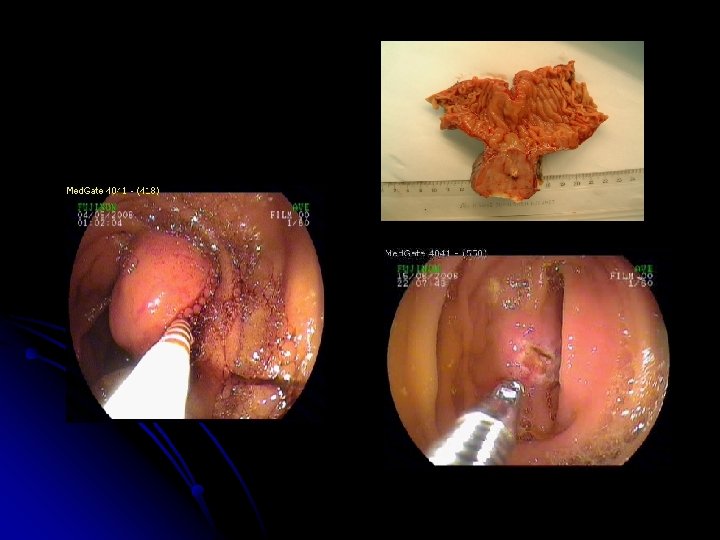
diagnosis Endoscopy l Barium graphy l Chest radiogram l CT l EUSG l
 Radiation Cheomoradiation Dilataion Ablation Photodynamic thrapy")
treatment l l l l Surgery (only %40) Radiation Cheomoradiation Dilataion Ablation Photodynamic thrapy EMR (<3 cm) Stents

Tumors of Stomach Cengiz Pata, M. D Gastroenterology Department, Yeditepe University Istanbul

HISTOLOGY 95% Adenocarcinoma - papiller - tubular - mucinous 4% Adeno-squamous < 1% Squamous < 1% undifferentiated
 l BI, BII resection")
Stomach Carcinoma Epidemiology l Chronic A-Gastritis l Chronic B-Gastritis (HP) l BI, BII resection l Polyposis l Chr. Ulcer Ventriculi l M, Menetrier l Blood Group A l Men > Women
 I. Polypousform II. Ulcerated III. Ulcerated-infiltrative IV. Diffuse-infiltrative")
Macroscopic (Borrmann Classification) I. Polypousform II. Ulcerated III. Ulcerated-infiltrative IV. Diffuse-infiltrative
 III. Excavated")
Early Cancer Japan I. Protrusion II. Surface ( , , ) III. Excavated

Therapy Radical Tumour Resection St. Op : Gastrectomy Lymphadenectomy Omentum major + minor Splenectomy Antrum Ca : partial resection ? Primary inoperable neoplasm chemotherapy radiation

Prognosis 5 year rate l Carcinoma l Early in citu 100 % Ca : 90 %

Small intestine tumors Cengiz Pata, M. D Gastroenterology Department, Yeditepe University Istanbul

clasification Adenoca %35 -50, proximal l Carcinoid TM %20 -40 apendix, ileum l Lymphoma %14 -MALTOMA -IPSID -EATCL (after the gluten enteropathy %7 -10) -multiple Lymphoid Poliposis -Periferal Nodal lenfoma l Fibrosarkom l Angiosarkom l Liposarkom l Leiyomyosarkom l
 Adenoma l GIST l Hamartoma l Angioma l Pseudotumor (brunner gland hyperplasia,")
Bening (41%) Adenoma l GIST l Hamartoma l Angioma l Pseudotumor (brunner gland hyperplasia, pancreatic rest, endometrioma, hyperplastic polyps l
 Carcinoids tumors (25 -45%) l GIST (15 -25%) l Adenocarcinoma (30 -40%)")
Malign (51%) Carcinoids tumors (25 -45%) l GIST (15 -25%) l Adenocarcinoma (30 -40%) l Lymphoma (4 -10% ) l Metastatic carcinoma l Malign melanoma l
 cell")
NET l APUD (Amine precursor uptake and decarboxylation) cell

Introduction İntestine and pancreas l İncidance 1/ 100, 000 l Carcinoid %50 l

Clinics

Zollinger Ellison Syndrome l Severe peptic ulcer diathesis + gastric acid hypersecretion due to b-cell endocrine tumor l 0. 1 -1% of PUD patients l Sporadic, or associated with MEN type I (25%)

Zollinger Ellison Syndrome l >80% Localized to gastrinoma triangle: cystic & common bile ducts, duodenum, junction head and body of pancreas. l 60 % malignant, up to 50% with metastasis l Clinical: PUD >90% (recurrent, multiple, refractory, complicated)

Clinical features of Zollinger. Ellison syndrome
, Pancreas (40 -80%) Pituitary (30 -60%) l")
MEN I l Autosomal Dominant: Parathyroid (~90%), Pancreas (40 -80%) Pituitary (30 -60%) l Contributory effect of hyperparathyroidism, hypercalcemia hypergastrinemia acid secretion l Higher incidence of carcinoids l Smaller and multiple duodenal gastrinomas
")
Diagnosis of Gastrinoma Combination of clinical signs l Fasting gastrin levels (> 150 pg/ml) l Avoid confounding factors (hypochlorhydria, PPIs, outlet obstruction, renal failure) l Assess acid secretion (if low- excludes) l Provocative tests (calcium, secretin) l
 l Exclusion of metastasis l If")
Treatment l Localization (EUS, Oct scan, MRI, CT) l Exclusion of metastasis l If positive – symptomatic cure l If negative attempt surgical resection ( less likely in MEN I ~ 6%)

NET Diagnosis l Clinics l Histopathology l Hormon level l Stimulating test l Radyology
 l Stopping tumor growth And Better life l")
NET treatment Surgery (total excision difficult) l Stopping tumor growth And Better life l Image courtesy of Dr. L. Anthony.

NET, medical treatment l Somatostatine l interferone l Cheomothreapy

Carcinoid tumore syndrome

Carcinoid tumor l GIS system end respiratory system l İncidance 100, 000 1/2 l Apendectomy and diagnose !
 – dyspepsia – misdiagnosis")
Carcinoid tumor l Asymptomatic (up to liver metastase ) – dyspepsia – misdiagnosis
 %10 l Large, metastatic poor survive l")
Carcinoid syndrome (disease) %10 l Large, metastatic poor survive l

Carcinoid syndrome l serotonine
 Bronkokonstriksiyon (%3– 19) Abdominal pain (%10– 55) Artriis")
Carcinoid sendrom – symptoms Telanjektzy (%25) Bronkokonstriksiyon (%3– 19) Abdominal pain (%10– 55) Artriis (%7) flushing (%63– 94) Heart disease (%14– 41) cyanose (%18) Diarrhea (%68– 84) Dermatitis (%5)

Attack of Carcinoid

5 -HIAA Carcinoid tumor 5 -HIAA, serotoninine l Urinary expression of 5 -HIAA l 40
 l Biochemical (5 -HIAA, chromogranin A) l")
Diagnosis l Pathology( arginofil and argentaffin ) l Biochemical (5 -HIAA, chromogranin A) l Octreo. Scan®*, CT, MR l Bronchoscopy, gastroscopy, colonoscopy
: 14 S– 27 S.")
survive Vinik A, et al. Dig Dis Sci. 1989; 34(suppl): 14 S– 27 S.

treatment

Carcinoid disease treatment

Carcinoid tumor follow up Asymtomatic Every year • 5 -HIAA • Chromogranin A • Pre-operative marker • Abdominal CT (6 -12 mounths) Symtpmatic Every 4 - 6 mounths • 5 -HIAA • Chromogranin A • Follow up high marker Every 6 - 12 muonths • Abdominal CT • Echocardiography • Octreo. Scan®
 l Binding Sst-2/sst-5 receptor l %70 and %80")
Treatment, Sandostatin Long activation (every mounths) l Binding Sst-2/sst-5 receptor l %70 and %80 l Activation of these receptor l

Sandostatin • Theropatic level: 7 - 11 day • One mounths Adapted from Lancranjan I, et al. Metabolism. 1995; 44(suppl 1): 18– 26.

Effect of 5 IHAA Supress to 50% *L 1. Rubin J, Ajani J, Schirmer W, et al. J Clin Oncol. 1999; 17: 600– 6. 2. The Medical Network. Healthcarenews. http: //www. themedicalnetwork. org/full_magazine/june 2003 -p 28– 40. pdf.
; BASE = baseline (başlangıç). Rubin J, et al. J")
defecation SCN = screening (tarama); BASE = baseline (başlangıç). Rubin J, et al. J Clin Oncol. 1999; 17: 600– 6. flushing

diarhea 1. Rubin J, Ajani J, Schirmer W, et al. J Clin Oncol. 1999; 17: 600– 6. 2. The Medical Network. Healthcarenews. http: //www. themedicalnetwork. org/full_magazine/june 2003 -p 28– 40. pdf.
: 50– 3. after")
Survive before Anthony LB, et al. Digestion. 1996; 57(suppl 1): 50– 3. after

adenocarcinoma High animal fat and protein, bile acid, polyposis syndrome, crohn disease, celiac disease Crampy periumblical pain, bloating, nausea, Bleeding, obstruction, intussiception, volvulus, weight lessions 5 year survive %20 -35 Cheomotherapy, surgery
 MALToma Multiple lymphoid polyposis Difuse large")
lymphoma l l l T cell lyphoma (celiac) MALToma Multiple lymphoid polyposis Difuse large cell Small noncleaved lymphoma (malabsorbtion: T cell, others: obstruction, pain, mass unless bacterial overgrowth) l IPSID
 beningn or")
IPSID l l l l alfa chain disease (west type lymphoma ) beningn or low grade lymphoma Ig. A 15 -25 year severe diarhea, abdominal pain, weight loss, fever Double bloon endoscopy, band alfa 2 or beta in electrophoresis, Early stage antibiotics (tetracyline plus metranidazole 6 -12 mounts) Malignant chance occurs: cheomathrapy
, leiomyoblastoma, myofibroblastic")
GIST Nonepithelial neoplasms l Primitive mesencymal cells l Leiomyoma, schwanoma, leiyomyosarcoma (70%), leiomyoblastoma, myofibroblastic tumor l All segments of GIS, 60% stomach, 30% intestine l Prognose: size>5 cm, mitotic count 1 -5 per 10 high power, presence of c kit gene l bleeding l 5 year survive 25 -30% l Radiotion, cheomotherapy (tyrosinase kinase İnhibitor –St 1 -571)`, surgery l
- Slides: 56