Complications of the ulcer disease of the stomach
")



 Perforation (10%) Bleeding (20%) Malignization (0, 3 -15%) Penetration (5%)")

 Localization А) in")
 1. Dagger pain 2.")


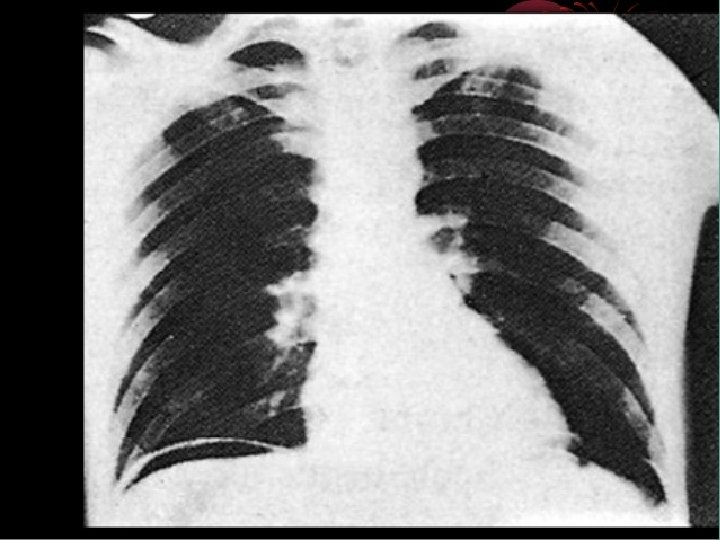
 “free” gas Overview")








 – defeat with the ulcer")








- Slides: 44
Complications of the ulcer disease of the stomach and duodenum (perforation, penetration, malignization)
The relevance of the problem • Ulcer perforation of the stomach and duodenum in 2012 registered 14. 4% of patients with peptic ulcer disease • Postoperative mortality in ulcer perforation of the stomach and duodenum is 0, 5 -2, 7%, especially in the elderly. • The bulk of the patients with perforation occurs between the ages of 20 and 45 years of working age. • The frequency of surgical interventions in ulcer penetration is 5. 9% • Timely detection and diagnostic of malignancy of gastric ulcers in the developed countries of 0. 07%, when developing countries (Uzbekistan), the frequency of detection of malignant ulcers is 0. 69%
Complication ulcer disease Stenosis(10%) Perforation (10%) Bleeding (20%) Malignization (0, 3 -15%) Penetration (5%)
Tasks of GP • Healthy life propagation • Early diagnosis • Gastric and duodenal ulcer primary diagnostics execution • Lab-instrumental diagnostics of gastric and duodenal ulcer (EGDFS, morphology) • Treatment of uncomplicated ulcer states • Early defining the complications and sending to hospital treatment • Execution of excellent rehabilitation after surgical manipulations • Dynamic examination of patients
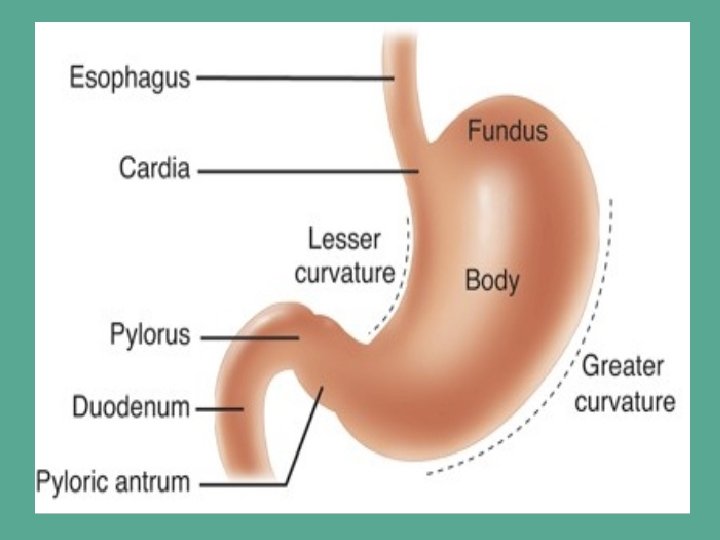
Classification of the ulcer perforations (B. D. Komarov, V. S. Savelev) Localization А) in the stomach By small curvature Anterior wall Posterior wall Cardial zone Pyloric zone B) In the duodenum Anterior wall Posterior wall Clinic currency А) perforation into the free space, into the abdominal cavity B) Hidden perforation C) Perforation with the atypic currency
Main signs of the perforation of the ulcer (Mondor’s triad) 1. Dagger pain 2. Board abdomen 3. Presence of the ulcer anamnesis The board abdomen defines at the palpation
The rate of development of peritonitis is higher, the lower the acidity of gastric juice. • That is why the propagation phenomena (diffuse) purulent peritonitis can not be 6 or even 12 hours after perforation of a duodenal ulcer. At the same time, these terms are usually expressed with perforation of stomach ulcers (very quickly within 2 -3 hours there is a diffuse purulent peritonitis with destruction and tumor perforation of the stomach).
Ways of the spreading of pain at the prforation of the UDS and duodenum 1. 2. 3. 4. 5. Epigastria Right lateral channel Right iliac area Pelvis Left iliac area 1 2 3 5 4 At the ulcer perforation the clinic of the spreading of the pain is similar with the clinic of acute appendicitis (Cocher-Volkovich symptome).
Free gas under the dome of the diaphragm (Spijarskiy symptome ) “free” gas Overview X--ray
Differential diagnostis 1. Acute appendicitis - laparosopy 2. Acute cholecystitis – US, X-ray 3. Acute oancreatitis – US, diastasa 4. Intensification of the UDS an duodenum – Xray, EGDFS 5. Acute mesenterial thrombosis - laparoscopy 6. Acute inferct - ECG
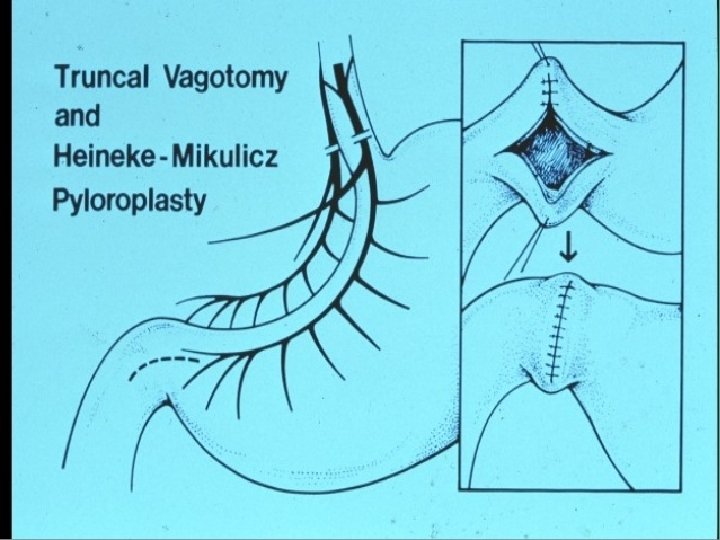
Choose of the method of the operation at the perforation of the ulcer Stage of the fermentative desinteration Stage of the festering peritonitis Radical operation Palliative operation Resection TV+ antrumectоmy TV+ pyloroplastic Sewing of the prforative ulcer
Conservative treatment by the method of Taylor • When the patient categorically refuses surgery. • Under local anesthesia with 1% tetracaine thick administered into the stomach probe, through which it was freed from contents. After removal of the large probe transnasally a delicate stomach tube and connect it to an apparatus for continuous aspiration, which is carried out over several days. Put an ice pack on his stomach. The correction of water and electrolyte balance, full parenteral nutrition, detoxication therapy and prescribed massive doses of antibiotics for 7 -10 days. Before removing the probe on it introduced a water-soluble contrast and radiographically convinced of the absence of its flowing contours of the stomach or duodenum. Meanwhile, even in the case of separating the perforations gastroduodenal ulcer, the likelihood of formation of local abscesses of the abdominal cavity is very high. Therefore, this method can be recommended as a last resort, since its ineffectiveness is lost time, suitable for surgery, and the patient will be doomed, despite its belated consent for surgery.
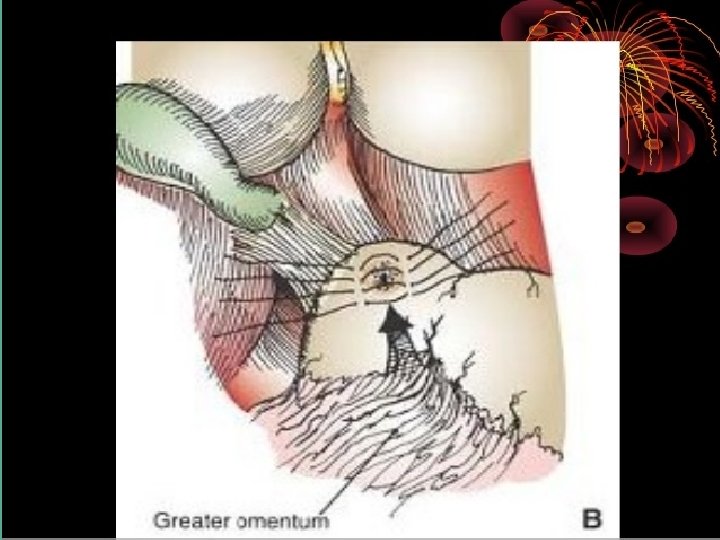
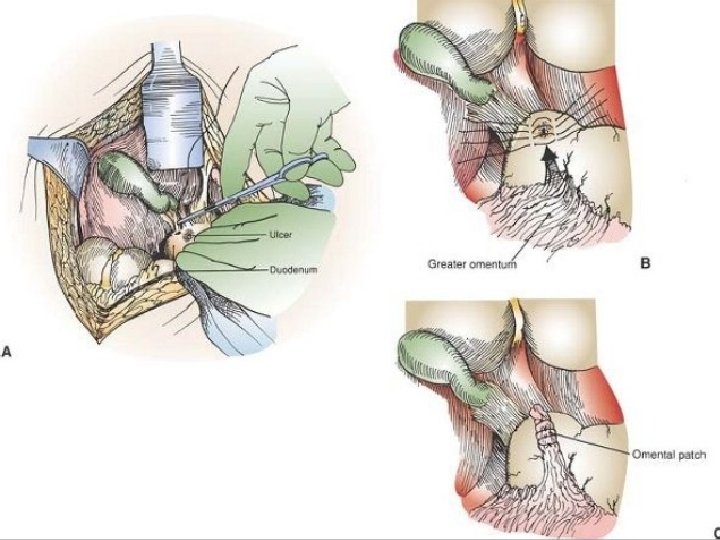
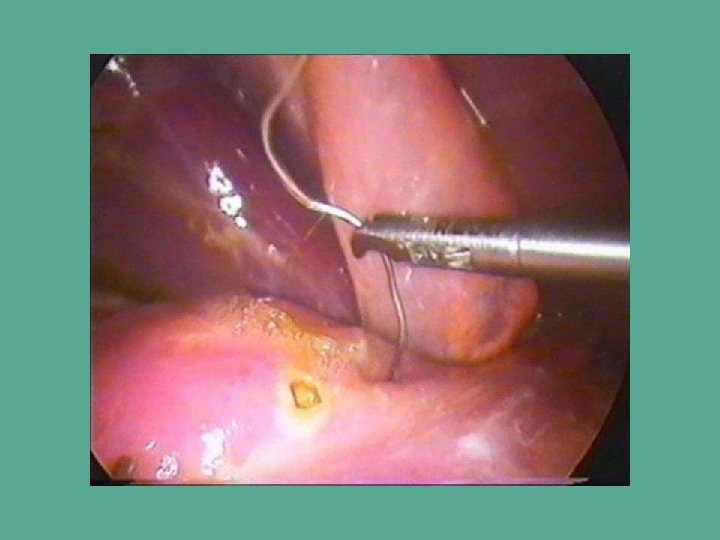
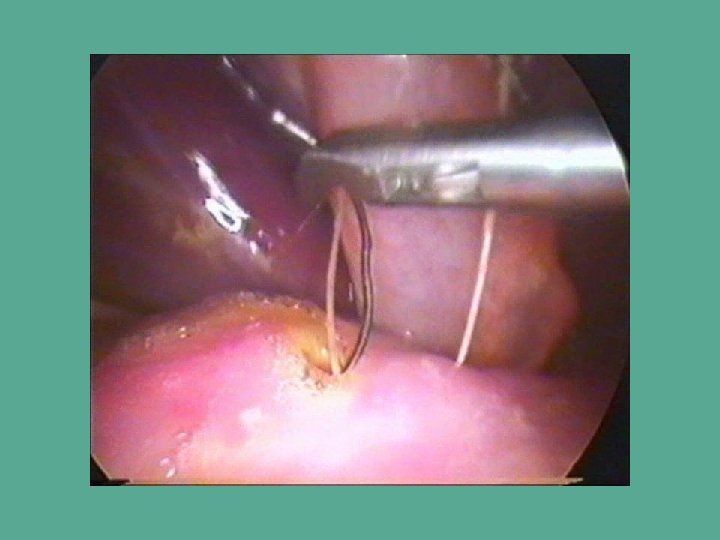
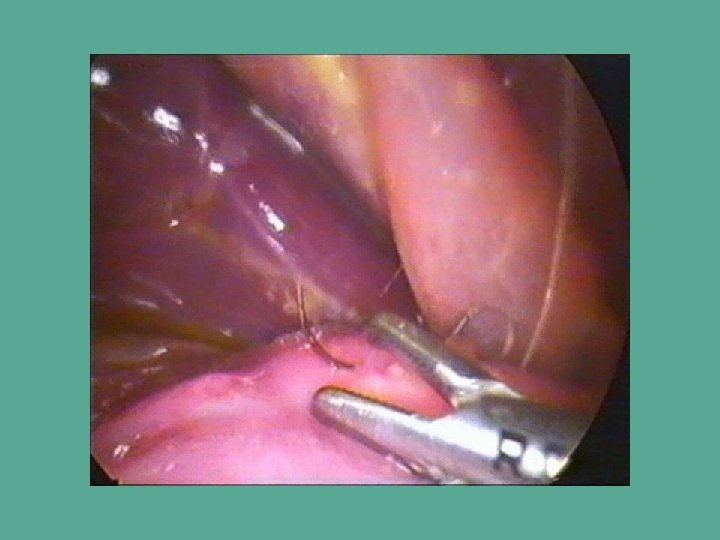
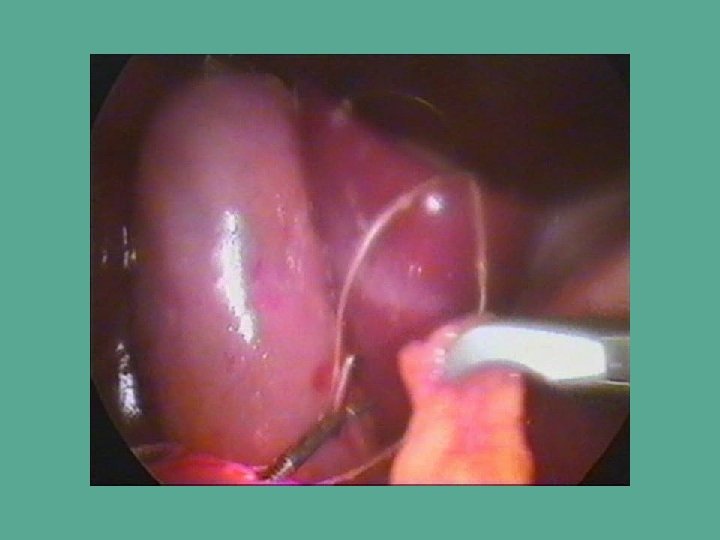
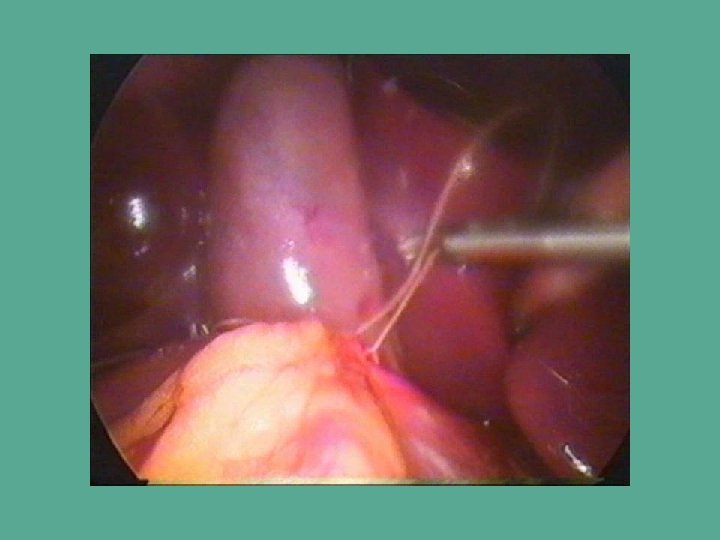
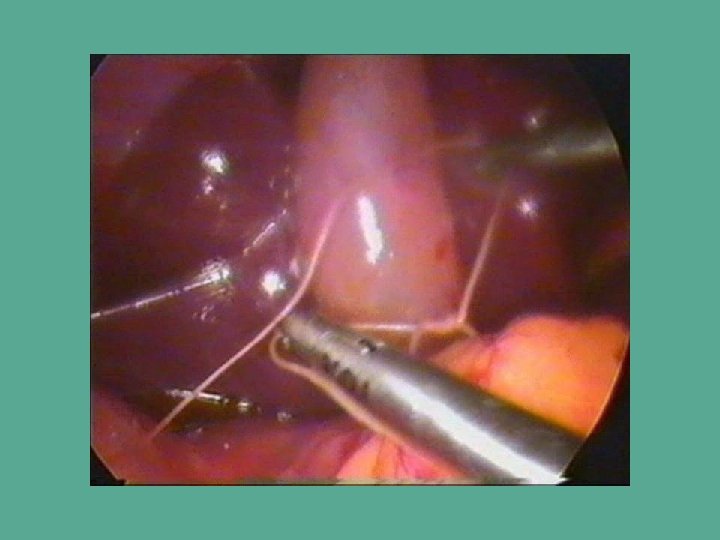
Sewing of the perforative ulcer
Suturing perforated ulcer
Resection of the stomach – radical operation at the perforations of stomach an duodenum
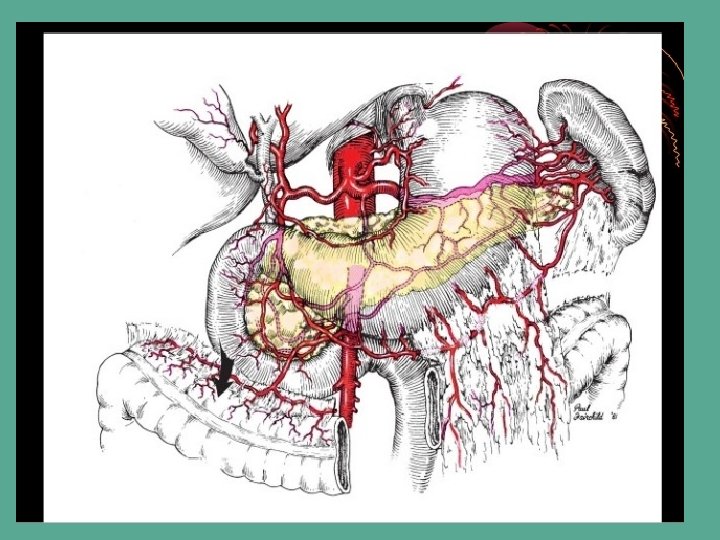
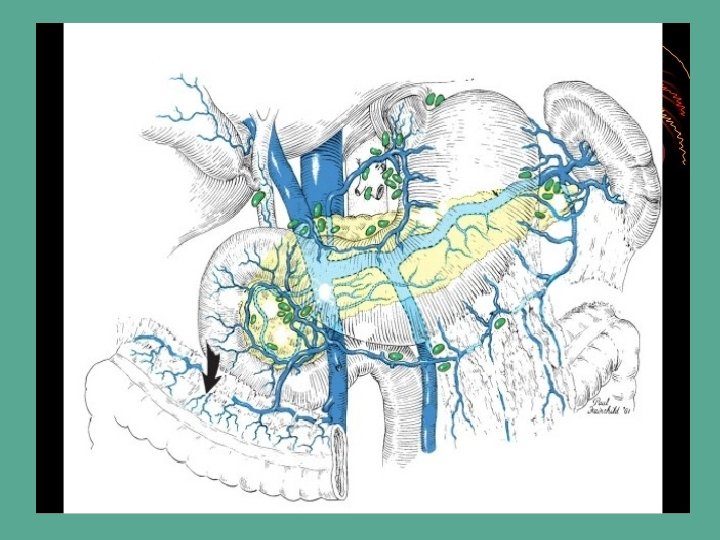
Penetration – passing of the ulcer onto the nearest organs Pancreas Liver Gall bladder
Stages of the penetration • 1 stage (39 -51%) – defeat with the ulcer process all layers of the stomach or duodenum • 2 stage (25 -30%) – fibrous connection with the nearest organs • 3 stage (22 -29%) – the fundus of the ulcer is the parenchima of the nearest organ
Symptoms of the penetration of the ulcer • Constant pain in the epigastria with the increasing • Irradiation of the pain depend on the organ, in which the penetration was: to the lumbar area (pancreas), to the scapula (liver), to the neck (gall bladder) • Not effective conservative therapy • At the penetration into the hollow organ the fistula appears.
Method of sewing of the cult at the penetration
Malignization – regeneration of the ulcer into the cancer The ulcer of stomach maligns in 20% cases The ulcer of the duodenum maligns in 0, 3% cases States at which the risk of malignization is high: • diameter of ulcer more than 1, 5 sm, ØAt the localization of ulcer in the stomach, ØAt the patients elder than 40 years, ØNot effective conservative therapy during 4 -6 months.
ULCUS-TUMOR
Signs of the malignization at X-ray • Defect of filling, • Convergention of the pleats • Absence of the peristaltic around the ulcer Defect of filling (finger pressing in)
Gastrectomy
мо ни то р Point of introduction of trocars and location of the members of the surgical team оператор Асс 2 Асс 1