Gastric and duodenal ulcer disease Ulcer disease n



 Ø smooth non-elevated borders and smooth base Ø")


 - acute (major, form affected")


 – gastro-duodenoanastomosis end-to-end Ø Billroth II (BII)")






 Ø appears after")


























- Slides: 56
Gastric and duodenal ulcer disease
Ulcer disease n ulcer is a defect of gastric or duodenal mucosa which interfere over lamina muscularis mucosae, submucosa or penetrates across whole gastric or duodenal wall n rise of ulcer is conditioned by presence of acid gastric content n frequent disease, men are afected 3 -4 x more than women
n Pathogenesis: Ø multifactorial Ø dysbalance between protective and aggressive factors - Protective f. : saliva, food, alcalic duodenal fluid, mucus mucine, fast regeneration of gastric epithelial cells, well perfused gastric mucosa - Aggressive f. : HCl, pepsin, bile acids (reflux), helicobacter pylori, drugs (analgetics, aspirin, korticoids), nicotine, alcohol
n Classification: Acute ulcer (ulcus acutum) Ø smooth non-elevated borders and smooth base Ø major bleeding into upper GIT Chronic ulcer (ulcus chronicum) Ø rushed and elevated boders, inflammation with hypertrophic and fibrotic proliferation is present Ø the most frequent form of ulcer disease • • Ulcus chronicum mediogastricum Ulcus chronicum ventriculi et duodeni Ulcus chronicum praepyloricum Ulcus chronicum duodeni
n Symptoms of gastric ulcer disease: Ø epigastric pain after meal or during meal Ø upper dyspeptic syndrome – loss of appetite, nauzea, vomiting, flatulence Ø vomiting brings relief Ø reduced nutrition Ø loss of weight
n Symptoms of duodenal ulcer disease: Ø epigastric pain 2 hours after meal or on a empty stomach or during night Ø pyrosis Ø good nutrition Ø obstipation Ø seasonal dependence (spring, autumn)
n Complications: Ø Bleeding - chronic (minor, cause anaemia) - acute (major, form affected vessel) Ø Perforation - mostly bulbus duodeni, anterior gastric wall - acute violent pain - bleeding can be present Ø Penetration - of the ulcer deeply through whole wall into neighbor organ (pancreas, liver) Ø Stenosis - narrow of the lumen caused by scar, oedema or inflammatory infiltration after healing of the ulcer - rise only at pyloric localization - vomiting of huge volume of gastric content
Zeman, M. et al. , Speciální chirurgie, ISBN 80 -7262 -260 -9, 2004 A – penetration B – perforation C – bleeding D - stenosis
n Therapy: Ø Conservative • • regular lifestyle prohibition of the smoking and alcohol diet (proteins, milk and milky products) pharmacology (antagonists of H 2 receptors, antacids, anticholinergics Ø Surgical • • BI, BII resection proximal selective vagotomy with pyloroplastic suture of perforated or haemorrhagic ulcer
n Stomach resections: Ø Billroth I (BI) – gastro-duodenoanastomosis end-to-end Ø Billroth II (BII) – gastro-jejunoanastomosis end-to-side with blind closure of duodenum Ø Proximal selective vagotomy – denervation of parietal gastric cells
Zeman, M. et al. , Speciální chirurgie, ISBN 80 -7262 -260 -9, 2004 Billroth I
Zeman, M. et al. , Speciální chirurgie, ISBN 80 -7262 -260 -9, 2004 Billroth II
Zeman, M. et al. , Speciální chirurgie, ISBN 80 -7262 -260 -9, 2004 Gastro-enteroanastomosis on Roux Y crankle
Zeman, M. et al. , Speciální chirurgie, ISBN 80 -7262 -260 -9, 2004 Vagotomy
n Complications after stomach resection: Ø Early – dehiscence, stenosis of anastomosis, bleeding, pancreatitis, obstructive icterus, affection of neighbour tissues Ø Late - days, weeks - early dumping syndrome - late dumping syndrome - incoming crankle syndrome - outcoming crankle syndrome - ulcer in anastomosis or in outcoming crankle
n Early dumping syndrome: Ø group of symptoms approved shortly after meal Ø appears after BII resection Ø vasomotoric sy. - face redness, fall of blood pressure, dizziness Ø GI sy. - vomiting, diarrhoea Ø Th. : diet, no sugar, low quantities of food, change BII to BI resection
n Late dumping syndrome: Ø hypoglycaemia (sugar is not enough digested) Ø appears after BII resection Ø weakness, perspiration, dizziness, tremor cca 3 h after meal Ø Th. : no sugar, change BII to BI resection
n Incoming crankle syndrome: Ø stasis of the content at incoming crankle increase intraluminal pressure Ø appears after BII resection Ø Th. : diet, change BII to BI resection
n Outcoming crankle syndrome: Ø chronic or acute closure of outcoming crankle Ø appears after BII resection Ø vomiting after meal, convulsive pain Ø Th. : change BII to BI resection
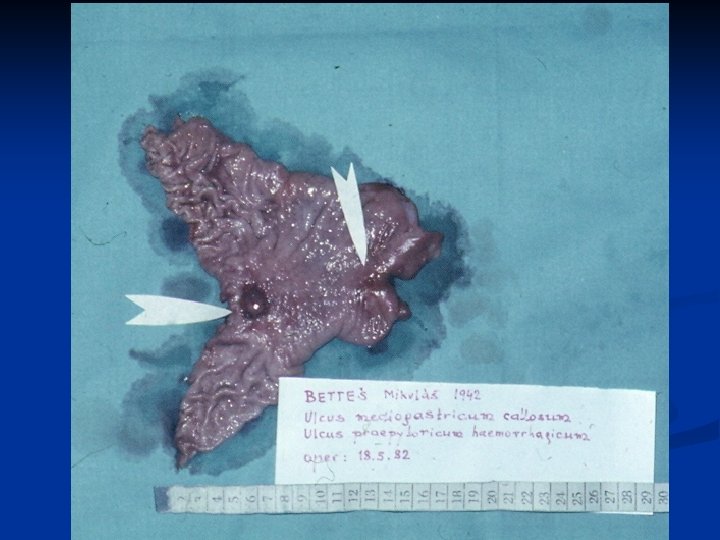
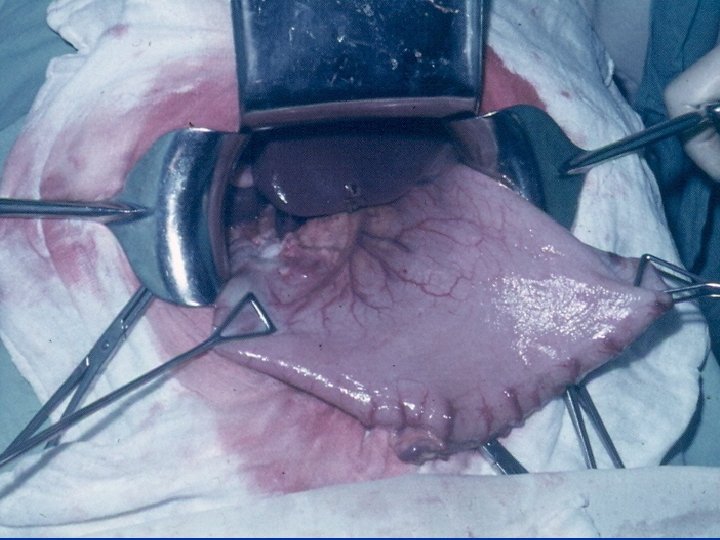
Haemorrhagic mediogastric ulcer
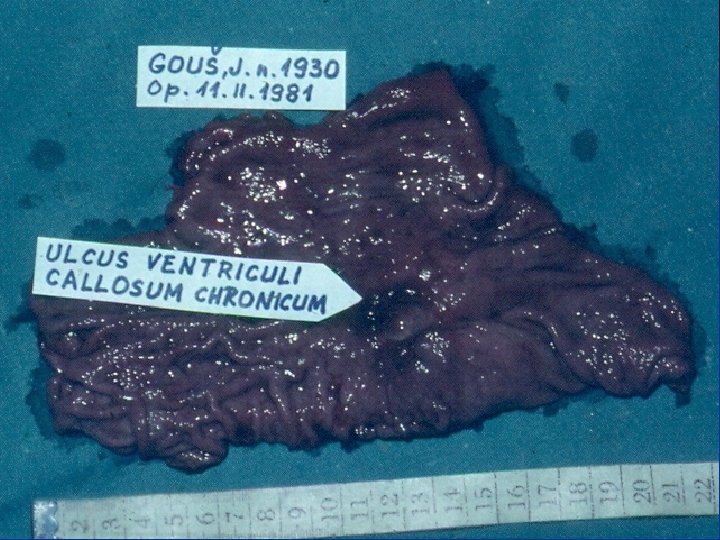
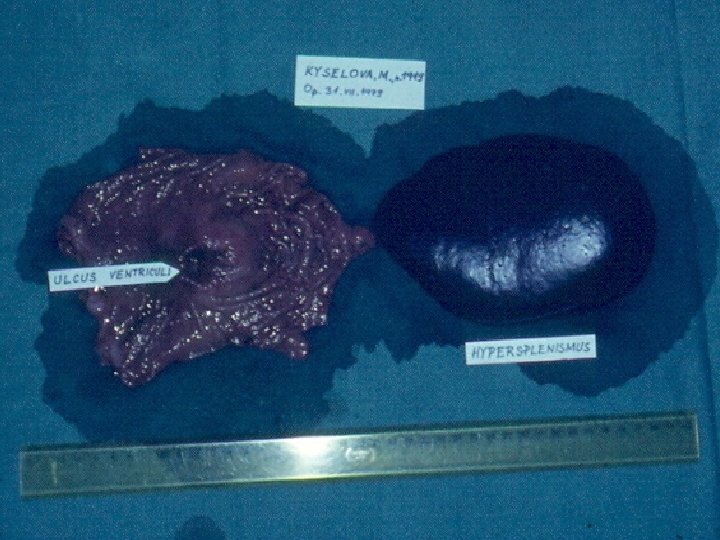
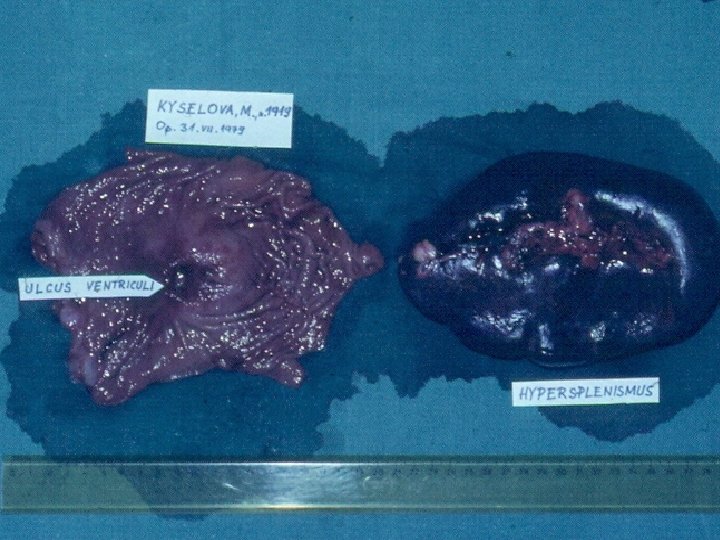
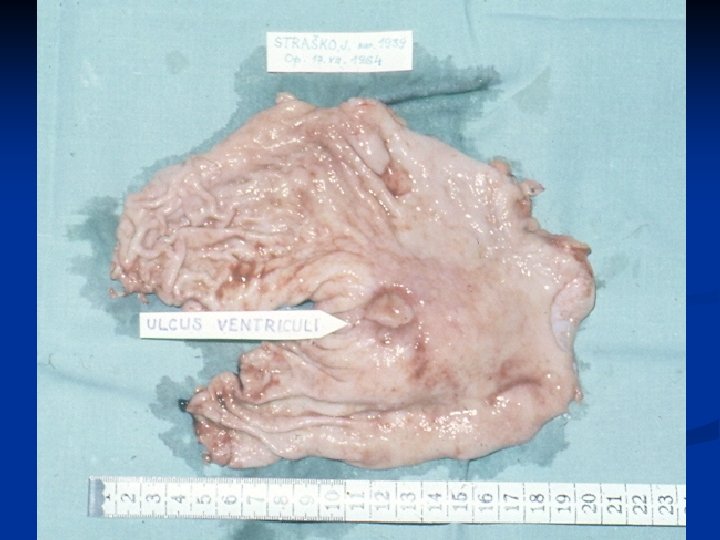
Chronic gastric ulcer
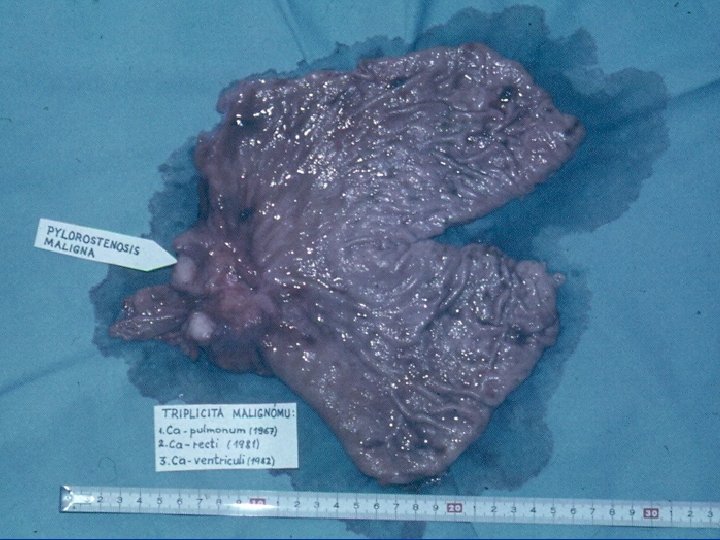
Pylorostenosis and gastrectasia
Duodenal ulcer
Stress ulcers
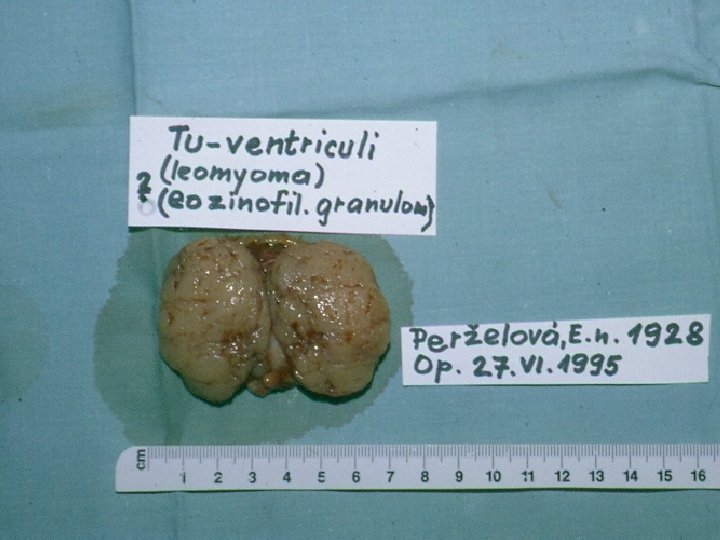
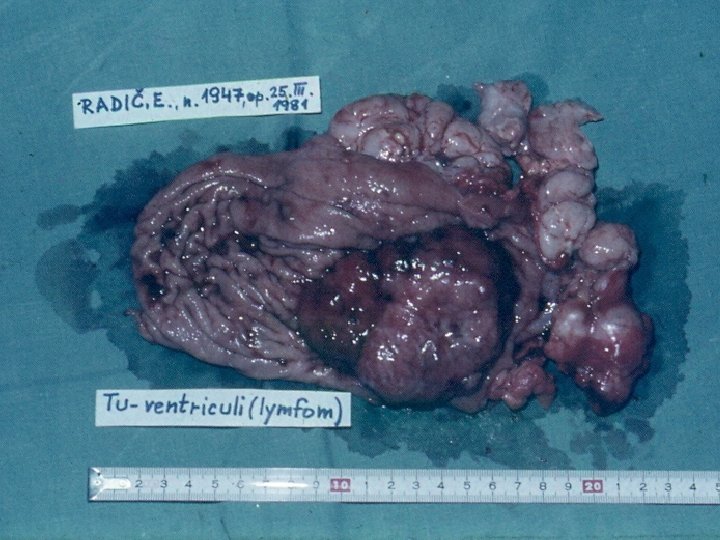
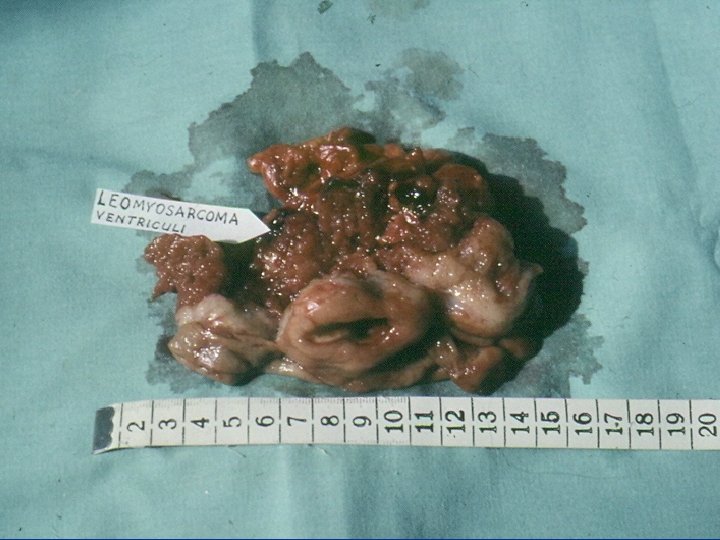
Benign stomach tumors n rise from all layers of stomach wall n often asymptomatic n Polypus, Leiomyoma, Lipoma, Fibroma, Neurofibroma, Neurinoma, Hemangioma, Karcinoids, Lymfoma n Diagnostic: endoscopy, X – ray n Therapy: local excision, stomach resection
Stomach cancer n Symptoms: Ø Ø n long-time asymptomatic feeling of full stomach, odour from mouth, tiredness, anaemia, occasional vomiting, loss of appetite, loss of weight Diagnosis: Ø Ø Ø gastrofibroscopy – biopsy - histology X-ray, USG, CT - metastasis Wirchow´s nodule – enlargement of left supraclavicular nodule
Stomach cancer n Etiopathogenesis: Ø n Praecancerosis: adenomatous polypus, chronic atrofic gastritis, foveolar hyperplasia (Ménétrier disease), stub of the stomach after BII resection Division: Ø Macroscopic: exofytic polypoid form, diskyform ulcerous form, diffused infiltrating form Ø Histopathologic: adenocarcinoma, papilar, tubular, gelatinous cancer, round cell cancer, flagstone cell cancer, etc.
Stomach cancer Zeman, M. et al. , Speciální chirurgie, ISBN 80 -7262 -260 -9, 2004 n Therapy: Ø Ø Currative – total gastrectomy, sub-total gastrectomy Paliative – gastrostomy, jejunostomy
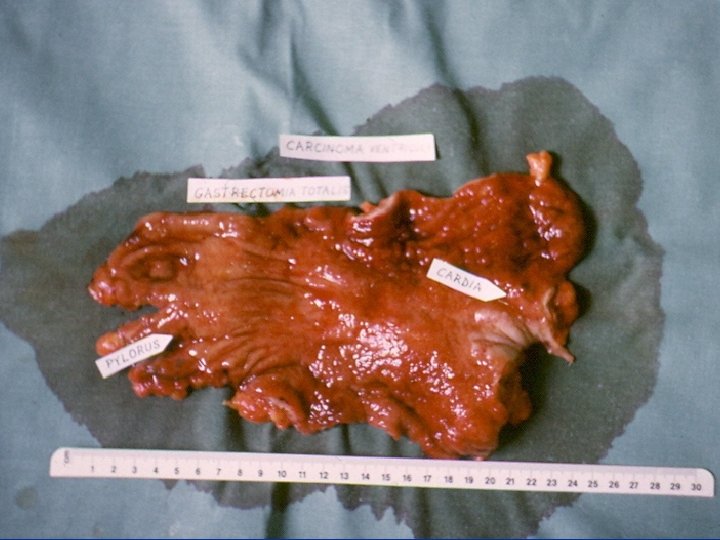
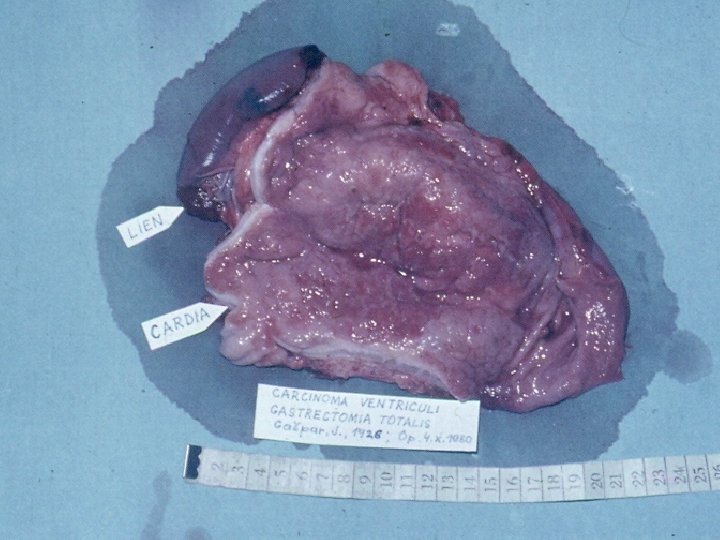
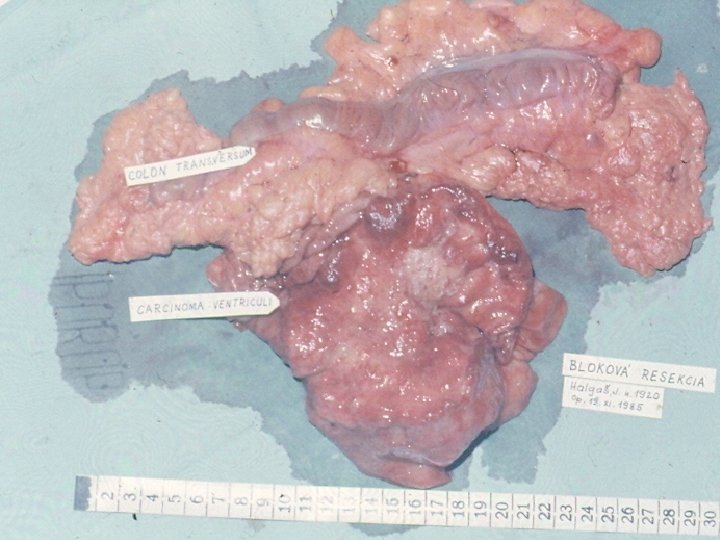
Gastric cancer
Gastric stub cancer after B II resection
Schwanoma fundi vetriculi
Than you for your attention!!!