Lung Conditions Traumatic Injury to the Lung Read










 n")



























- Slides: 39
Lung Conditions & Traumatic Injury to the Lung Read Neuro Chapter 60
Objectives To outline and discuss management of some of the commonly encountered lung conditions and traumatic injuries to the lung including: n Pneumonia n Pulmonary embolis n Pneumothorax n Pleural effusion n Barotrauma
Figure U 13 -2: Structures of the Lower Airways
Pulmonary Embolism n Pulmonary embolism occurs when a blood clot becomes lodged in a lung artery, blocking blood flow to lung tissue. Blood clots often originate in the legs.
Video: PE What is a Pulmonary Emoblism? What are the symptoms associated with it?
Pulmonary Embolism n Blockage makes it more difficult for the heart to pump blood through lungs. As a result, less oxygen is available to the rest of the body. If the blockage is large enough, tissue death (infarction) occurs in the lung area cut off from circulation. Pulmonary embolisms are commonly misdiagnosed.
Signs and Symptoms n Easily attributed to other conditions and vary with the size and number of clots. n Such as a heart attack n Pneumonia n Hyperventilation n Congestive heart failure n Panic attacks.
No Classic Pattern: Most common symptoms: n. A sudden unexplained onset of shortness of breath, tachypnea or tachycardia, as well as sharp knifelike chest pains (pleuritic chest pain), when taking a breath, & sense of impending doom.
WHAT ELSE? Blood may be coughed up as a result of lung tissue damage n If the clot is particularly large, it can lead to dizziness and even fainting due to dangerously low blood pressure. n
Who is at risk? n n n Immobilization — Being immobilized puts a strain on the circulatory system. Although the heart acts as the body’s main pump, movement also assists in keeping blood circulating properly. Long periods of inactivity may increase risk of blood clots. Examples include lengthy road trips or flights, or bed rest due to illness or surgery. Blood abnormalities — Some people are born with blood that’s more prone to clotting & those dehydrated, septic, have Ca, those giving birth.
Other Risk Factors for Pulmonary Embolism n Advanced age (especially over age 70) n Significantly overweight n Birth control pills, HRT drugs & the osteoporosis drug raloxifene (Evista) are examples of drugs that list a small risk of developing blood clots.
About 90 % of Pulmonary Emboli Result When a Clot Travels from a Leg to a Lung - often no symptoms n n Blood tests, a chest X-ray, an electrocardiogram — to help rule out other possible reasons for symptoms. Sometimes a leg blood clot may cause redness, swelling and pain in the calf muscle area. Refer to a physician promptly. A pulmonary angiogram is a more definitive test, although it involves some risk and is more expensive. the CT scan (computed tomography scan) — instead of lung scan or pulmonary angiogram. CT scan is a less invasive test that provides fast and accurate results.
Thoracic Surgery n n Teaching: why frequent monitoring of vital signs, hematocrit, and amount of plural drainage is important following thoracic surgery. At what point should the attending physician be called? Explain why regular assessment of the trachea is important post-op. Why are pulmonary function tests important? What results may indicate an increased risk of complications?
The patient is nursed upright in bed to allow for maximum chest expansion and unrestricted drainage and may even be extubated in the upright position. Because the patient is not in the recovery position, particular care must be taken that the airway is not obstructed and respiration rate, effort and oxygen saturation levels are closely monitored. As there is a risk of CO retention, a maximum of four litres per minute of oxygen is given and blood gases may have to be checked. The ECG is checked for cardiac arrhythmias, a potential complication for these patients (Schedel & Connolly)
Think What should you do, if while turning a client just back from the OR following a segmental or wedge resection, there is a sudden gush of fluid through the chest tube? n Shouldn’t pooled blood have clots in it? n Following post-op chest surgery, why is the client at risk of hypoxemia? Identify how gas exchange may be improved. Should the “good lung or bad lung” be down? n
Common Respiratory Problems Following Thoracic Surgery n Refer also to student presentations & presentation on Lung Cancer earlier in term they all relate
Keep in mind!! n n Patients tend to gasp milliseconds before a crash or a fall. This fills lungs with air, distends alveoli, making them more prone to rupture.
PNEUMOTHORAX
Pneumothorax
Pneumothorax Open Air enters the chest during inspiration & exits during expiration. A slight shift of the affected lung may occur because of a decrease in pressure as air moves out of the chest (Smeltzer, 2000, p. 468) Tension Air enters but cannot leave the chest. As the pressure increases, the heart & great vessels are compressed & the mediastinal structures are shifted towards the opposite side of the chest. The trachea is pushed from its normal midline position toward the opposite side of the chest & the unaffected lung is compressed (see picture- next)
Pneumothorax Chest Tube CT scan of the chest showing a pneumothorax on the patient's left side. A chest tube is in place (small black mark on the right side of the image), the air -filled pleural cavity (black) and ribs (white) can be seen. The heart can be seen in the center.
Tension Pneumothorax Inspiration Expiration
Nursing Alert n Traumatic open pneumothorax is an acute emergency requiring immediate intervention. n Stopping the air from entering the chest is life saving. Relief of tension pneumothorax is an emergency measure
Signs and Symptoms of an open/closed pneumothorax n n n Respiratory distress hypotension compensatory tachycardia Increased central venous pressure pallor cyanosis n n Sounds of an air leak, bubbles in blood from wound in chest wall. Compression/compro mise of heart and unaffected lung is a LIFETHREATENING EMERGENCY!!!
Open versus Closed Pneumothorax If chest injury is caused by blunt trauma and chest wall remains intact, pneumothorax is CLOSED. Air enters chest cavity from the lungs. n If chest injury is penetrating and chest wall is compromised, pneumothorax is OPEN. Air enters chest cavity from the wound. n
Nursing Alert n n n Traumatic open pneumothorax is an acute emergency requiring immediate intervention. Stopping the air from entering the chest is life saving. Relief of tension pneumothorax is an emergency measure
Chest Tube
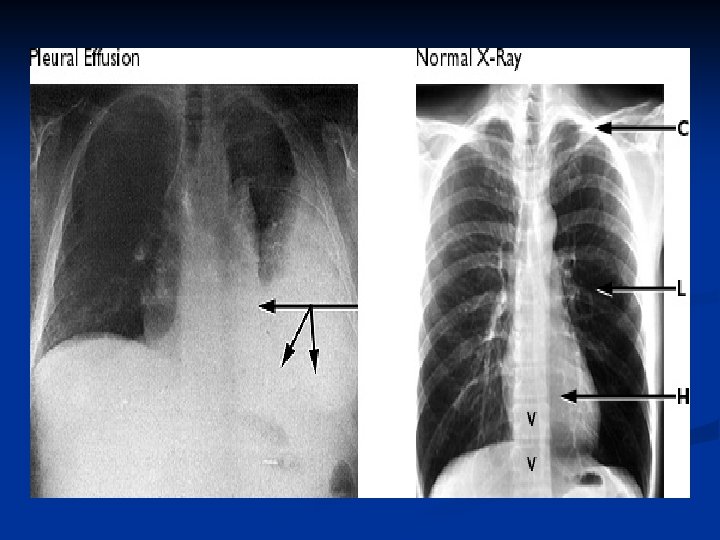
Pleural Effusion Abnormal buildup of fluid between linings of the lung and chest wall n result of a disease process or inflammation n Normally 5 to 10 m. L of serous fluid in the visceral and parietal pleura. n Any more can cause great changes in intrathoracic pressure. n
Pleural Effusion Pleural = Pleural Cavity Effusion = abnormal, excessive collection of this fluid
Signs and Symptoms Pleural effusion in itself does not cause symptoms. n If effusion expands and presses on lung, patient may develop n sharp, localized pain that worsens with coughing, or deep breathing. n Dyspnea n non-productive cough. n
Signs and Symptoms cont. . . Early signs include decreased or bronchial breath sounds on the affected side, dullness to percussion, and decreased fremitus over area of fluid accumulation n Auscultation: EGOPHONY n n Hear “A” over fluid accumulation when patient speaks “E”.
Complications of Pleural Effusion Respiratory compromise and distress from fluid compressing lung. n Infection in pleural space--Sepsis/Empyema n Fistulas in bronchi or chest wall n Inflammation/infection in pleural space leads to increased potential for adhesions. Adhesions isolate effusion to one lung and complicates treatment. n
Barotrauma n Barotrauma results from increased airway pressure and decreased expiratory flow mechanical bag-valve-mask ventilation n faulty equipment n misuse of positive pressure ventilation Thus, Barotrauma is physical damage to body tissues caused by a difference in pressure between an air space inside or beside the body and the surrounding gas or liquid n
Barotrauma n 4% of all mechanically ventilated patients develop a pneumothorax n 20% of patients receiving positive endexpiratory pressure develop a pneumothorax
Cor Pulmonale n Enlarged right side of heart due to diseases that affect the structure and function of the lung n Signs and symptoms n Increased edema in hands and feet n Distended neck veins n Enlarged liver n Pleural effusion n Ascites and heart murmur n SOB n Wheeze n Cough and fatigue
Atelectasis Collapsed or airless condition of alveoli n Caused by n n n hypoventilation, obstruction to the airways or compression Manifestations n Shallow breathing, dyspnea, pleural pain, central cyanosis, increased heart rate, cough, sputum production and low grade fever
Atelectasis
Cardiac Tamponade n Compression of the heart as a result of fluid within the pericardial sac n n Usually due to chest trauma Manifestations Hypotension n Jugular-venous distention n Muffled heart sounds n