Head Injury Head Injury Head injury is a









 Motor vehicle collisions Assaults Falls ◦ Penetrating Injury (open)")







 on the brain. • A contusion")


 • Caused by rapid movement of the brain during which")
 ◦ Clinical signs: LOC ICP Changes of postures cerebral")








 into ear (Otorrhea) or nose (Rhinorrhea) ◦ “HALO Sign –")



















 Acute subdural hematoma High mortality Signs within")



- Slides: 58
Head Injury
Head Injury Head injury is a broad classification that includes injury to the scalp, skull, or brain Head trauma includes an alteration in consciousness no matter how brief
Death from head injury trauma occurs at three time points after injury Immediately after injury – massive hemorrhage and shock Within 2 hours after injury – internal bleeding Approximately 3 weeks after injury – multisystem failure
Causes ◦ Motor vehicle accidents ◦ Firearm-related injuries ◦ Falls ◦ Assaults ◦ Sports-related injuries
Pathophysiology Sudden impact force to the head or inertial force with in the skull (skull is rigid and not allow any expansion) Disruption of blood vessels and rapid brain tissue displacement Bleeding or swelling with in the skull increases the volume of contents with in a fixed size
Increase ICP Downward or lateral displacement of the brain through or against the rigid structures of the skull Restriction Cell of blood flow to the brain in the brain become anoxic Ischemia and infarction Irreversible brain damage
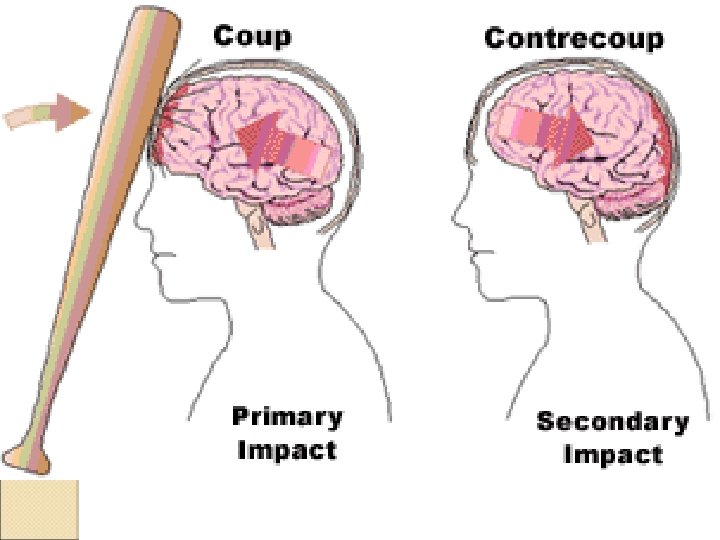
Mechanisms of injury Deformation – results from the direct or indirect transmission of energy to the skull If the force is sufficient, the skull is deformed and fractured. Acceleration – deceleration injuries – it occur when the accelerating skull, moving in a motor vehicle, suddenly decelerates when it hits an immobile object such as the steering wheel (coup – contracoup)
Rotational – distort the brain and can cause tension, stretching and diffuse shearing of brain tissues
Type of head injury Based on location , force imposed, and the cause head injury is classified as total brain injury, cranial injury etc
◦ Blunt Injury (closed injury) Motor vehicle collisions Assaults Falls ◦ Penetrating Injury (open) Gunshot wounds Stabbing Explosions
Scalp lacerations ◦ The most minor type of head trauma ◦ Scalp is highly vascular with poor constrictive abilities profuse bleeding ◦ Major complication is infection
Craniocerebral trauma Trauma must be extreme to fracture
Frontal fracture – CSF rhinorrhea Orbital fracture – periorbital ecchymosis Temporal Parietal fracturre – CSF otorrhea fracture – deafness, CSF otorrhea, facial paralysis, loss of taste, battles sign Posterior fossa fracture – cortical blindness and visual field defects Basilar skull fracture – CSF otorrhea, battles sign, bulging of tympanic membrane, tinnitus, facial paralysis, vertigo
A skull fracture is a break in the continuity of skull caused by forceful trauma. • Linear or depressed • Simple, comminuted, or compound • Closed or open
Brain Injury Direct brain injury • Immediate damage due to force Indirect brain injury • Results from hypoxia or decreased perfusion • Response to primary injury • Develops over hours Head Trauma - 15
Direct Brain Injury Types Coup ◦ Injury at site of impact Contrecoup ◦ Injury on opposite side from impact A coup injury occurs under the site of impact with an object, and a contrecoup injury occurs on the side opposite the area that was impacted.
Direct Brain Injury Categories Focal ◦ Occur at a specific location in brain Contusion Intracranial Hemorrhage Epidural hematoma Subdural hematoma Intracerebral Hemorrhage Diffuse – occurs at diffuse areas ◦ Concussion ◦ Diffuse Axonal Injury
Contusion • A contusion is a bruise (bleeding) on the brain. • A contusion can be the result from a direct impact to the head. • It is characterized by the extravasation of blood into the brain. • Contusion may occur on the site of impact or on the opposite side
◦ Concussion ◦ it is characterized by an immediate and transient impairment of neurologic function induced by mechanical force. ◦ An instant or delayed loss of consciousness may occur but patient usually recovers rapidly ◦ A person who shows any alteration in consciousness after a blow to the head should closely observed
Post concussion syndrome • 2 weeks to 2 months • Persistent headache • Lethargy, memory impairment • Personality and behavior changes
Diffuse axonal injury (DAI) • Caused by rapid movement of the brain during which delicate axons are stretched and damaged. • This damage interferes with nervous transmission and can cause extensive diffuse deficits Process takes approximately 12 -24 hours
Diffuse axonal injury (DAI) ◦ Clinical signs: LOC ICP Changes of postures cerebral edema
Shaken Baby Syndrome is a violent criminal act that causes traumatic brain injury. Shaken Baby Syndrome occurs when the perpetrator aggressively shakes a baby or young child. The forceful motion causes the brain to be injured. Blood vessels between the brain and skull rupture and bleed. The accumulation of blood causes the brain tissue to compress while the injury causes the brain to swell. This damages the brain cells. Shaken Baby Syndrome can cause seizures, lifelong disability, coma, and death. Irritability, changes in eating patterns, tiredness, difficulty breathing, dilated pupils, seizures, and vomiting are signs of Shaken Baby Syndrome.
Levels of brain injury Mild traumatic brain injury – less than 30 min. symptoms appear at the time of injury but many not develop for days or weeks Moderate - causes unconsciousness lasting more than 30 minutes. Symptoms are longer lasting Severe – more than 24 hours. Symptoms are similar to mild injury but more serious and longer lasting.
Signs & Symptoms of Brain Injury Cushing’s Reflex ◦ Increased BP ◦ Bradycardia ◦ Erratic respirations Vomiting § Without nausea § Projectile Body temperature changes Changes in pupil reactivity Abnormal posturing
Unconsciousness Confusion and disorientation Headache Dizziness Blurry vision Ringing in the ears- tinnitus Trouble speaking Changes in emotions or sleep patterns
Reduce mental status or Amnesia Retrograde Unable to recall events before injury Antegrade Unable to recall events after trauma “Repetitive Questioning” ◦ Altered orientation ◦ Alteration in personality Hemiplegia, Weakness or Seizures
Cushing ulcer It is a gastric ulcer produced by elevated intracranial pressure. It is also called von Rokitansky. Cushing syndrome. Apart from in the stomach, it may also develop in the proximal part of the duodenum and the distal esophagus. In increased ICP vagal stimulation occures which leads to increased secretion of gastirc acid
Basal Skull Fracture Signs ◦ Battle’s Signs Retroauricular Ecchymosis Associated with fracture of auditory canal and lower areas of skull ◦ Raccoon Eyes Bilateral Periorbital Ecchymosis Associated with orbital fractures
Battle’s sign Raccoon eyes Head Trauma - 31
◦ CSF leak (extravasation) into ear (Otorrhea) or nose (Rhinorrhea) ◦ “HALO Sign – a blood stain surrounded by a yellowish stain ◦ High risk infection or meningitis
Diagnostic Studies Methods to test CSF leakage Tes tape or dextrostix (same as suger test) Glucose is present in CSF gives a +ve reading for glucose. But if the blood is present, it gives a unreliable
Halo or ring sign Collect the fluid into a white pad. With In a few minutes the blood collects into the center and encircles the blood if CSF present
CT scan considered the best diagnostic test to determine craniocerebral trauma MRI Cervical spine x-ray Glasgow Coma Scale (GCS) Routine laboratory test (hemoglobin electrolytes, coagulation studies etc)
Management Medical management Medications depends on the nature and severity of the injury Medications include drugs to reduce ICP, prevent seizures, and analgesics Antibiotics are administered to any patient with a penetrating injury Analgesics to control pain
Nursing Care of Skull Fractures Minimize CSF leak • Bed flat • Never suction orally; never insert NG tube; cautionpatient not to blow nose Place sterile gauze/cotton ball around area
Immediate management Intubation to protect the airway, undergo surgery to treat internal injuries or immobilization to prevent further injures Ventilatory support
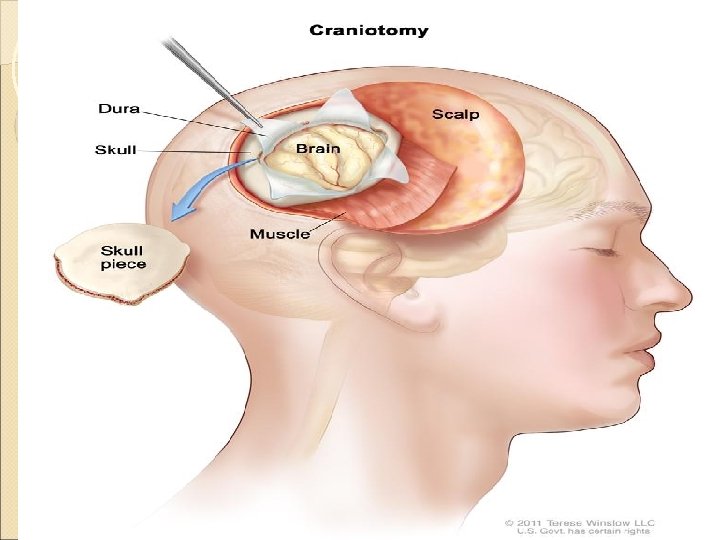
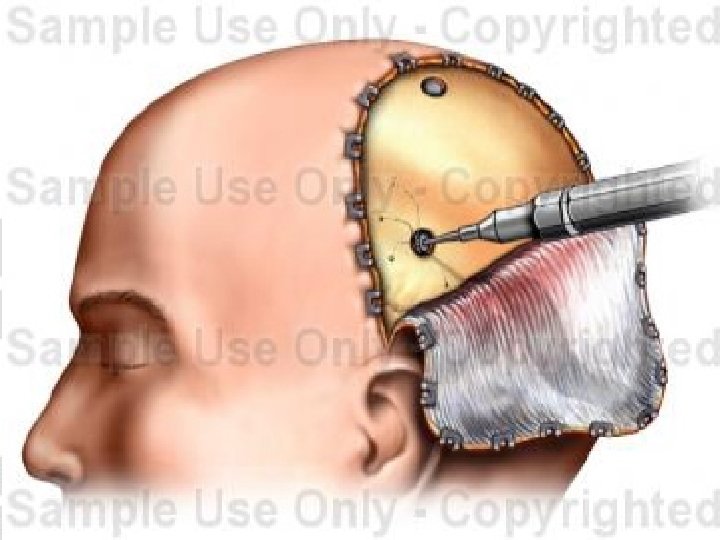
Surgical management If hematoma formation is there surgical intervention should be done Craniotomy - A craniotomy is a surgical operation in which a bone flap is temporarily removed from the skull to access the brain. The bone flap is then replaced using titanium plates and screws or another form of fixation (wire, suture) Decompressive Craniectomy – is a neurosurgical procedure in which part of the skull is removed to allow a swelling brain room to expand without being squeezed
Cranioplasty - Cranioplasty is a surgical repair of a defect or deformity of a skull. Burr-hole or trepanning - is a surgical intervention in which a hole is drilled or scraped into the human skull, exposing the dura mater to treat health problems related to intracranial diseases
Nursing management Emergency management In initial stage • Ensure patent airway • Stabilize cervical spine • Administer oxygen via nasal cannula or mask • Establish IV access with two large bore catheters to infuse NS • Control external bleeding with sterile pressure dressing • Assess for rhinorrhea, scalp wounds • Remove patients clothing's
Nursing assessment The patient with head injury is always considered to have potential for development of increased ICP. • GCS • Neurological status • Leakage of CSF • Obtain cause of injury, time of injury, direction and force of blow, loss of consciousness
◦ Overall goals: Maintain adequate cerebral perfusion Remain normothermic Be free from pain, discomfort, and infection Attain maximal cognitive, motor, and sensory function
Monitor vitals Assess for slowing of pulse, increased systolic pressure. Respirations become rapid and blood pressure may decrease Monitor for rapid rise in temperature Keep temperature below 38 degree to avoid metabolic demands Tachycardia and hypotension are indicators of bleeding
Assessing motor function Observe spontaneous movements Ask patient to raise and lower extremities Compare strength of hand grasp Assess responses to painful stimuli Determine ability to speak and quality of speech
Health Promotion Prevent car and motorcycle accidents Wear safety helmets
Nursing diagnosis Ineffective airway clearance r/d to hypoxia Ineffective cerebral tissue perfusion r/d to decreased CPP Deficient fluid volume related to disturbances of consciousness Imbalanced nutrition less than body requirement r/d to metabolic changes Risk for injury r/d to disorientation Risk for imbalanced body temp r/d to damage to temp regulating mechanism
Monitor for complications Cerebral edema Brain herniation Decreased cerebral perfusion Intra cranial Hemorrhage and hematoma formations Meningitis, wound infection Anosmia (nerve palsies) – lack of sense of smell Eye movement abnormalities Aphasia – language disorder Memory defects, post traumatic seizures
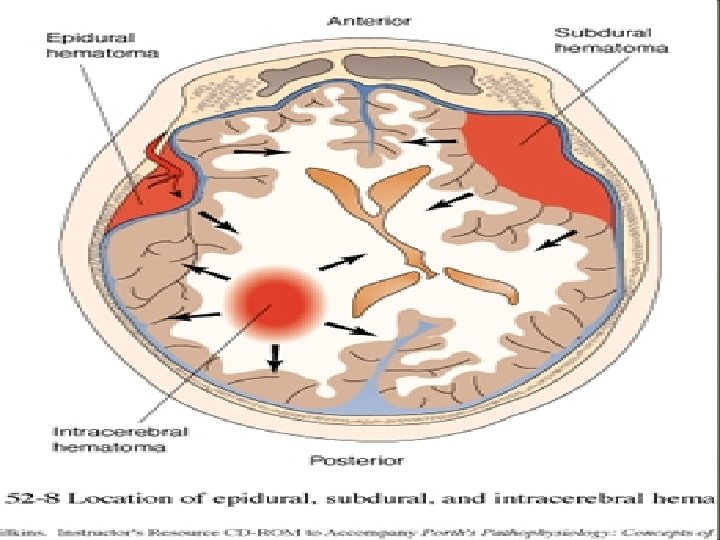
Head Injury Complications Epidural hematoma or extra dural hematoma • Results from bleeding between the dura and the inner surface of the skull • Bleeding in this area mainly caused by laceration of middle meningeal artery • This follows a basilar and temporal skull fractures
Subdural hematoma • Occurs from bleeding between the dura mater and arachnoid layer of the meningeal covering of the brain • Usually venous in origin and is due to rupture of small blood vessels that drain from the surface of the brain (bridging veins)
Epidural and Subdural Hematomas Epidural Hematoma Subdural Hematoma
Subdural hematoma (acute, subacute or chronic) Acute subdural hematoma High mortality Signs within 48 hours of the injury Associated with major trauma (Shearing Forces) Patient appears drowsy and confused with headache Pupils dilate and become fixed
◦ Subacute subdural hematoma Occurs within 2 -14 days of the injury Failure to regain consciousness may be an indicator
◦ Chronic subdural hematoma Develops over weeks or months after a minor head injury. After two to 4 days of bleeding in the brain it will become thicker and darker and later calcification or clot takes place Severe headache confusion and personality changes
Intra cerebral hematoma Bleeding with in the parenchyma leads to intra ceretral hematoma (bleeding into the substance of the brain). Because of rupture of intracerebral vessels at the time of injury. Symptoms are related to the specific area of the brain where clot forms