Hypertension Dr Mustafa Sahin Ankara Universitesi Tp Fakltesi


















 Thresholds and Recommendations for Treatment and Follow-Up (continued on next slide)")
















 20 ― 15")




 ATP III criteria : Aşağıdakilerden ≥ 3 • Abdominal obezite :")


- Slides: 73
Hypertension Dr. Mustafa Sahin Ankara Universitesi Tıp Fakültesi Endokrinoloji ve Metabolizma Hastalıkları Bilim Dalı
Factors Influencing Blood Pressure = Cardiac Output x Systemic Vascular Resistance
Factors Influencing BP • • HR SNS/PNS Vasoconstriction/vasodilation Fluid volume • • • Renin-angiotensin Aldosterone ADH
DEFINITION • Essential, primary, or idiopathic hypertension is defined as high BP in which secondary causes or mendelian (monogenic) forms are not present • High BP – repeatedly measured BP exceeding 140/90 mm. Hg, i. e. a systolic BP above 140 and/or diastolic BP above 90
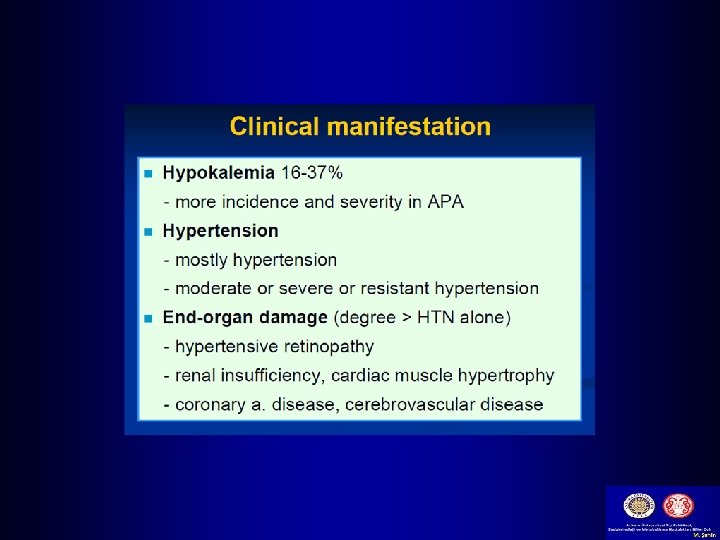
Giriş • Hipertansiyon sıklığı % 30 civarında • Esansiyel HT bunların % 85’i • Primer aldosteronizm eskiden düşünüldüğünden çok daha sıktır; esansiyel HT hastaları indikasyona bakılmaksızın tarandığında 10 -15 % ‘unda saptanmaktadır. Mulatero P Clin Endocrinol Metab 2004; 89: 1045. • Aldosteron, kan basıncı etkisinin yanında hedef organ hasarı yapar (İnflamasyon/fibroz) Sato A Hypertens Res 2004; 27: 303.
ALDOSTERON TUZ HEDEF ORGAN HASARI. Pimenta E Hypertension 2008; 51: 339.
Hypertension Complications § Hypertensive Heart Disease • Coronary artery disease • Left ventricular hypertrophy • Heart failure
Hypertension Complications § Cerebrovascular Disease • Stroke § Peripheral Vascular Disease § Nephrosclerosis § Retinal Damage
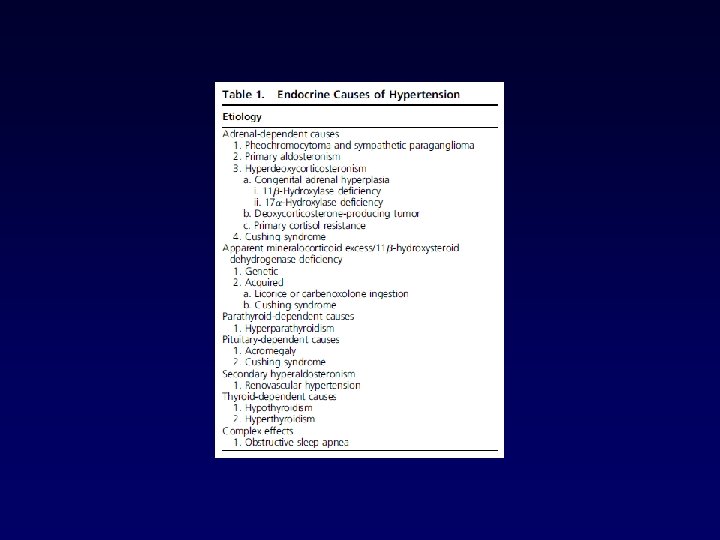
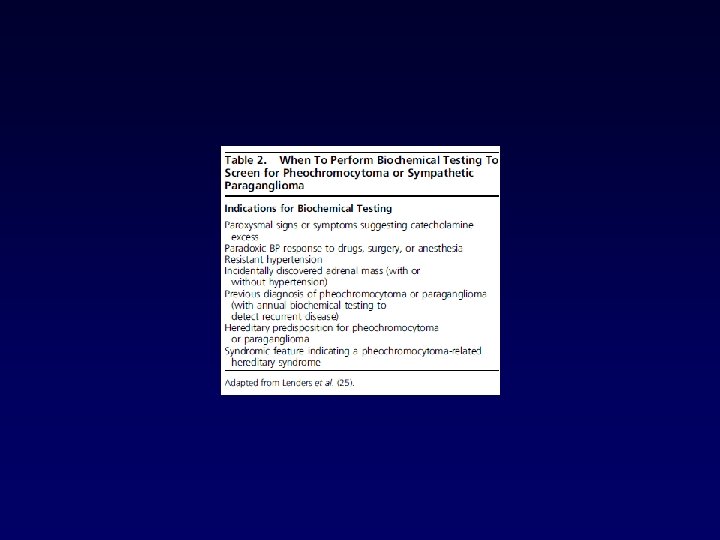
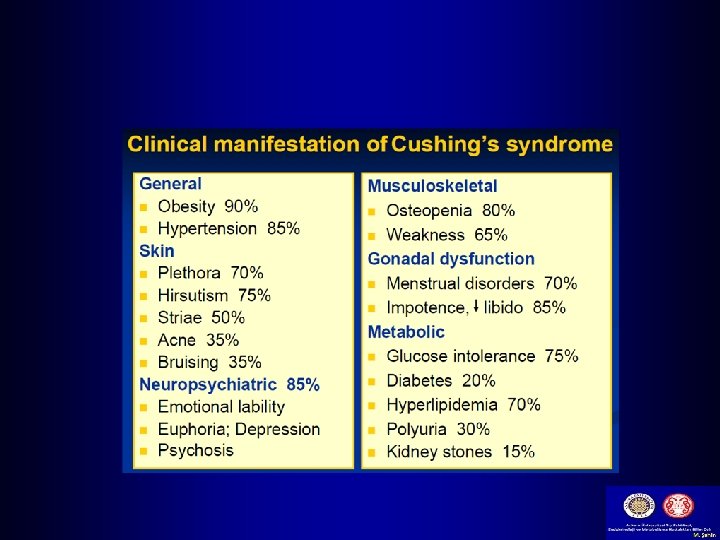
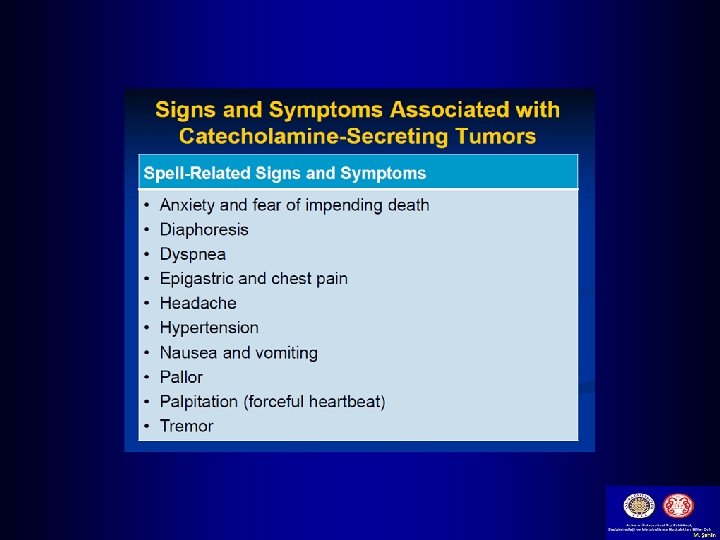
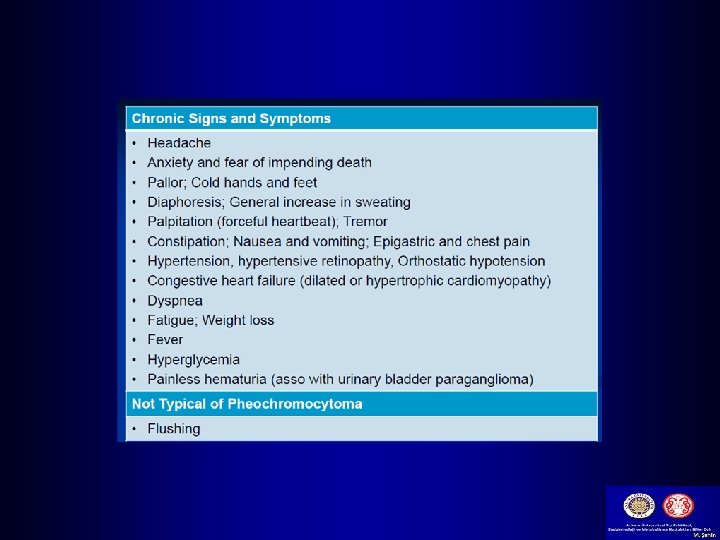
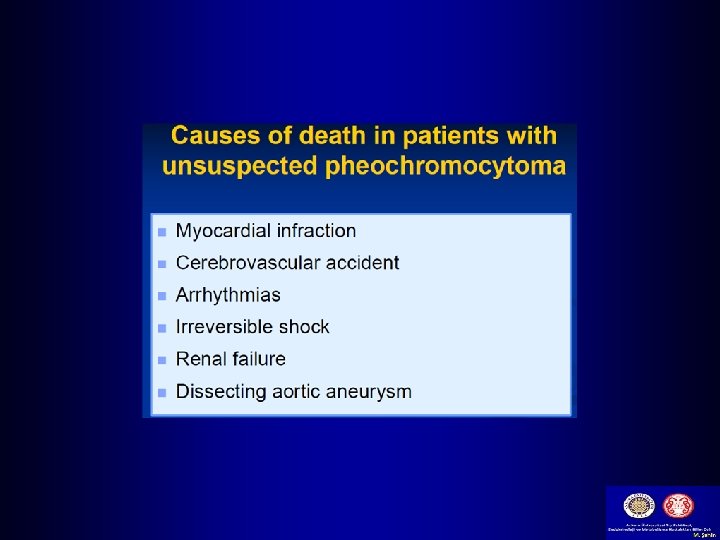
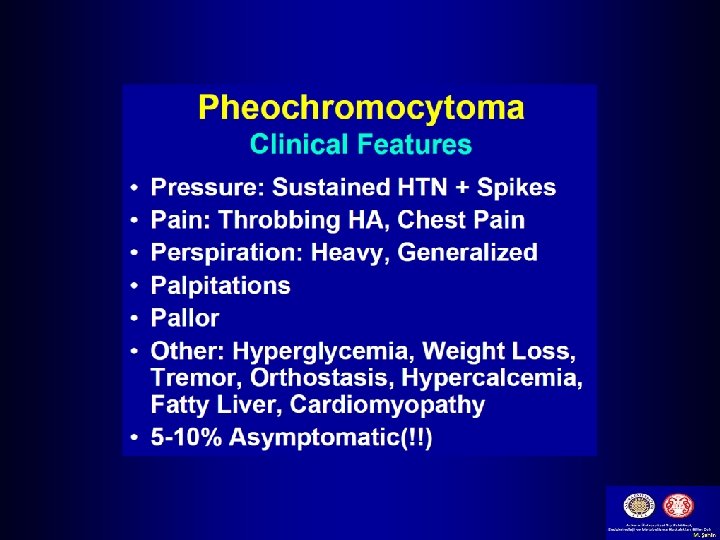
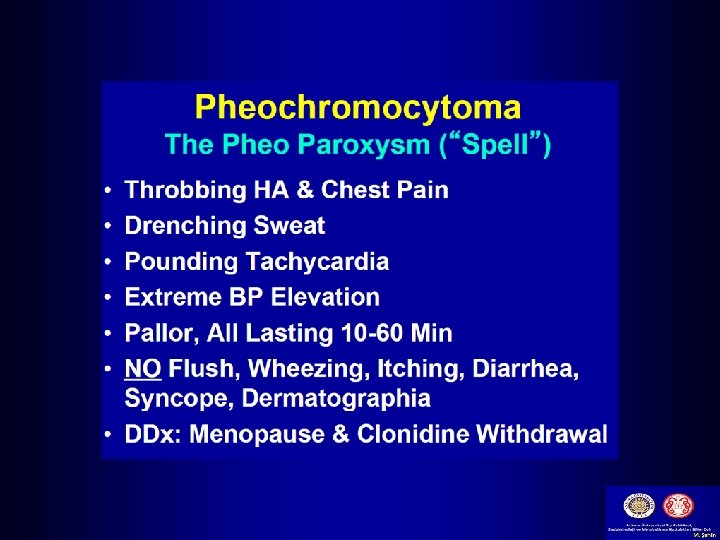
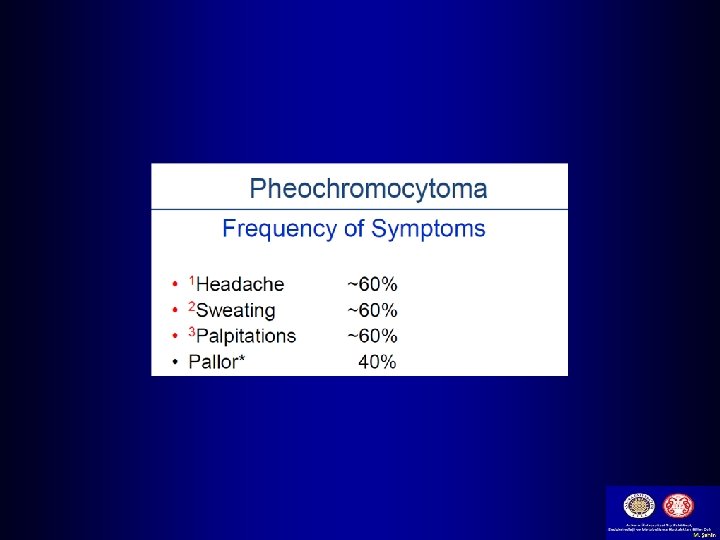
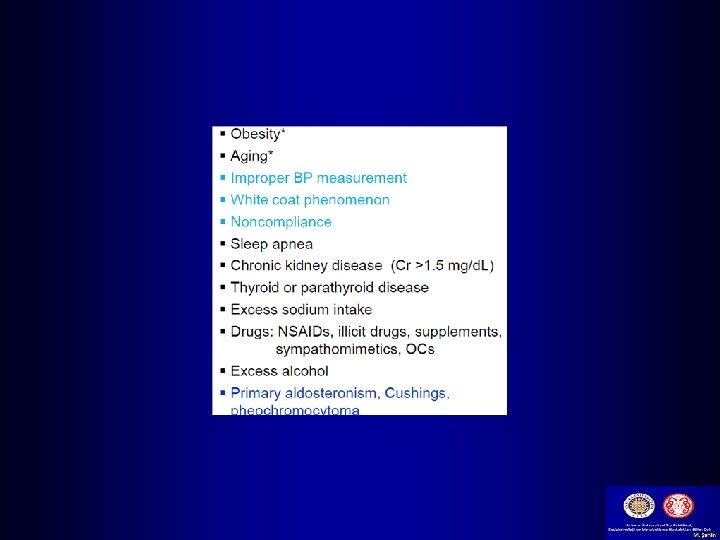
Causes of Secondary Hypertension With Clinical Indications Common causes Renal parenchymal disease Renovascular disease Primary aldosteronism Obstructive sleep apnea Drug or alcohol induced Uncommon causes Pheochromocytoma/paraganglioma Cushing’s syndrome Hypothyroidism Hyperthyroidism Aortic coarctation (undiagnosed or repaired) Primary hyperparathyroidism Congenital adrenal hyperplasia Mineralocorticoid excess syndromes other than primary aldosteronism Acromegaly
The left ventricle is markedly thickened in this patient with severe hypertension that was untreated for many years. The myocardial fibers have undergone hypertrophy.
BP Measurement • At least two measurements should be made and the average recorded. • Clinicians should provide to patients their specific BP numbers and the BP goal of their treatment.
CVD Risk Factors Common in Patients With Hypertension Modifiable Risk Factors* Current cigarette smoking, secondhand smoking Diabetes mellitus Dyslipidemia/hypercholesterolemia Overweight/obesity Physical inactivity/low fitness Unhealthy diet Relatively Fixed Risk Factors† CKD Family history Increased age Low socioeconomic/educational status Male sex Obstructive sleep apnea Psychosocial stress *Factors that can be changed and, if changed, may reduce CVD risk. †Factors that are difficult to change (CKD, low socioeconomic/educational status, obstructive sleep apnea, cannot be changed (family history, increased age, male sex), or, if changed through the use of current intervention techniques, may not reduce CVD risk (psychosocial stress). CKD indicates chronic kidney disease; and CVD, cardiovascular disease.
Categories of BP in Adults* BP Category SBP DBP Normal <120 mm Hg and <80 mm Hg Elevated 120– 129 mm Hg and <80 mm Hg 130– 139 mm Hg ≥ 140 mm Hg or 80– 89 mm Hg ≥ 90 mm Hg Hypertension Stage 1 Stage 2 or *Individuals with SBP and DBP in 2 categories should be designated to the higher BP category. BP indicates blood pressure (based on an average of ≥ 2 careful readings obtained on ≥ 2 occasions, as detailed in DBP, diastolic blood pressure; and SBP systolic blood pressure.
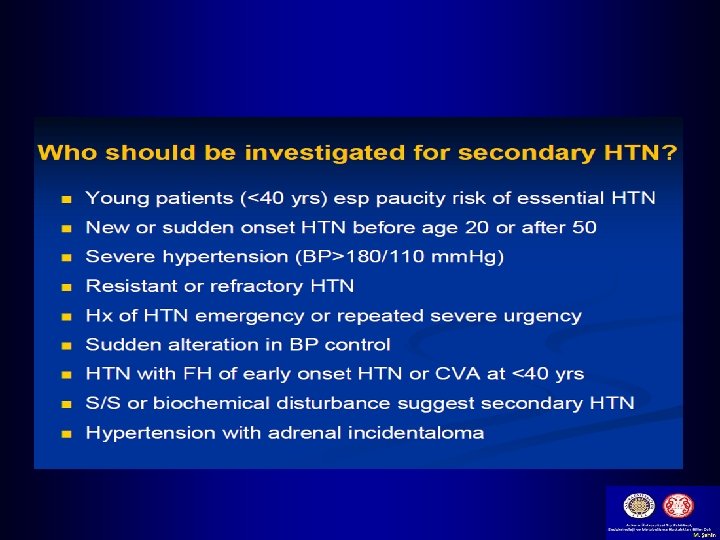
Sekonder HT : “ABCDE” A - Accuracy, Apnea and Aldosteronism B - Bruits & bad kidneys (Renal parenchymal disease) C - Catecholamine, Co arctations & Cushing’s syndrome D - Drugs & Diet E - Erythropoietin & Endocrine disorders
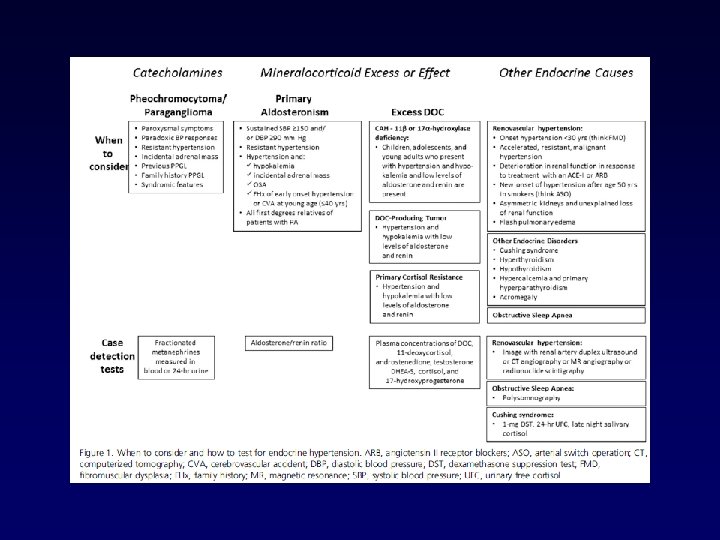
Secondary HTN-Screening Tests www. nhlbi. nih. gov
Screening for Secondary Hypertension Colors correspond to Class of Recommendation in Table 1. TOD indicates target organ damage (e. g. , cerebrovascular disease, hypertensive retinopathy, left ventricular hypertrophy, left ventricular dysfunction, heart failure, coronary artery disease, chronic kidney disease, albuminuria, peripheral artery disease).
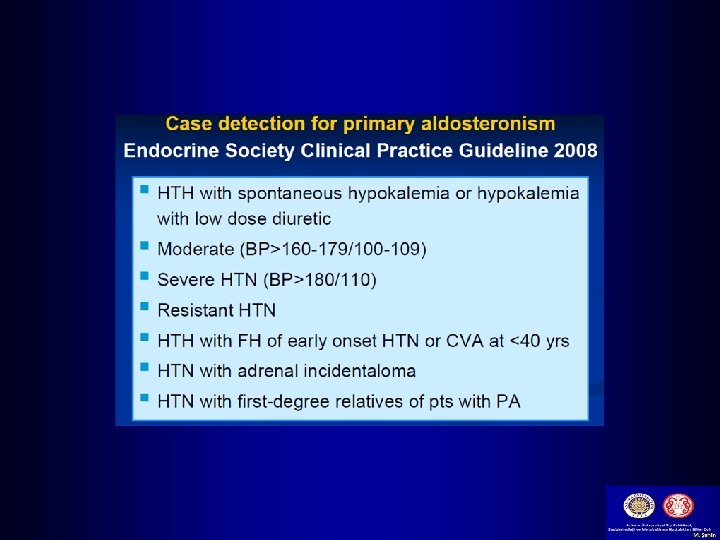
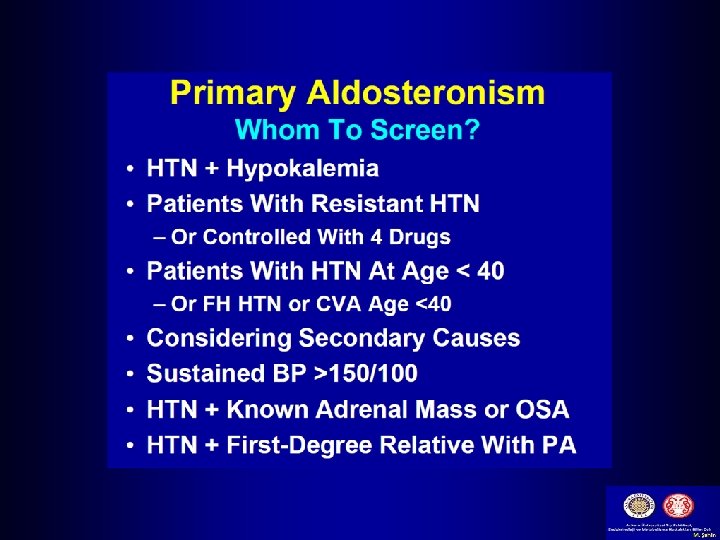
Primary Aldosteronism COR I I I LOE Recommendations for Primary Aldosteronism C-EO In adults with hypertension, screening for primary aldosteronism is recommended in the presence of any of the following concurrent conditions: resistant hypertension, hypokalemia (spontaneous or substantial, if diuretic induced), incidentally discovered adrenal mass, family history of early-onset hypertension, or stroke at a young age (<40 years). C-LD Use of the plasma aldosterone: renin activity ratio is recommended when adults are screened for primary aldosteronism. C-EO In adults with hypertension and a positive screening test for primary aldosteronism, referral to a hypertension specialist or endocrinologist is recommended for further evaluation and treatment.
Basic and Optional Laboratory Tests for Primary Hypertension Basic testing Fasting blood glucose* Complete blood count Lipid profile Serum creatinine with e. GFR* Serum sodium, potassium, calcium* Thyroid-stimulating hormone Urinalysis Electrocardiogram Optional testing Echocardiogram Uric acid Urinary albumin to creatinine ratio *May be included in a comprehensive metabolic panel. e. GFR indicates estimated glomerular filtration rate.
Blood Pressure (BP) Thresholds and Recommendations for Treatment and Follow-Up (continued on next slide)
Colors correspond to Class of Recommendation in Table 1. *Using the ACC/AHA Pooled Cohort Equations. Note that patients with DM or CKD are automatically placed in the highrisk category. For initiation of RAS inhibitor or diuretic therapy, assess blood tests for electrolytes and renal function 2 to 4 weeks after initiating therapy. †Consider initiation of pharmacological therapy for stage 2 hypertension with 2 antihypertensive agents of different classes. Patients with stage 2 hypertension and BP ≥ 160/100 mm Hg should be promptly treated, carefully monitored, and subject to upward medication dose adjustment as necessary to control BP. Reassessment includes BP measurement, detection of orthostatic hypotension in selected patients (e. g. , older or with postural symptoms), identification of white coat hypertension or a white coat effect, documentation of adherence, monitoring of the response to therapy, reinforcement of the importance of adherence, reinforcement of the importance of treatment, and assistance with treatment to achieve BP target.
History • Angina/MI Stroke: Complications of HTN, Angina may improve with b-blokers • Asthma, COPD: Preclude the use of bblockers • Heart failure: ACE inhibitors indication • DM: ACE preferred • Polyuria and nocturia: Suggest renal impairment
History-contd. • Claudication: May be aggravated by bblockers, atheromatous RAS may be present • Gout: May be aggravated by diuretics • Use of NSAIDs: May cause or aggravate HTN • Family history of HTN: Important risk factor • Family history of premature death: May have been due to HTN
History-contd. • Family history of DM : Patient may also be Diabetic • Cigarette smoker: Aggravate HTN, independently a risk factor for CAD and stroke • High alcohol: A cause of HTN • High salt intake: Advice low salt intake
Examination • Appropriate measurement of BP in both arms • Optic fundi • Calculation of BMI ( waist circumference also may be useful) • Auscultation for carotid, abdominal, and femoral bruits • Palpation of the thyroid gland.
Examination-contd. • Thorough examination of the heart and lungs • Abdomen for enlarged kidneys, masses, and abnormal aortic pulsation • Lower extremities for edema and pulses • Neurological assessment
Routine Labs • • • EKG. Urinalysis. Blood glucose and hematocrit; serum potassium, creatinine ( or estimated GFR), and calcium. • HDL cholesterol, LDL cholesterol, and triglycerides. • Optional tests urinary albumin excretion. albumin/creatinine ratio.
Young W F. Endocrinology 2003; 144: 2208 -2213
Subtype evaluation of primary aldosteronism. Young W F. Endocrinology 2003; 144: 2208 -2213
Hipertiroidizm 32
Hipotiroidizm • Ödemli yüz • Kuru, soluk, soğuk cilt • Konstipasyon • Apatik görünüm • Hafıza sorunları, seksüel disfonksiyon • Bradikardi, kalp sesleri derin • Diyastolik HT
Akromegali- Klinik şüphe 1991 2005
PLATORE; SUPRAKLAVİKULER YAĞLANMA; HİRSUTİZM AKNE; PLATORE; AYDEDE YÜZ
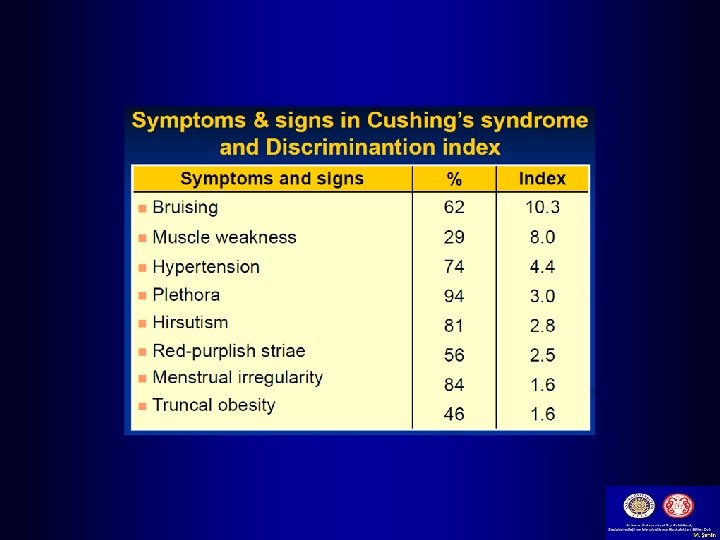
Causes of Cushing's syndrome
Abdominal striae caused by excess cortisol production
Primer hiperaldosteronizmin HT hastalarında sıklığı 25 ― 20 PA sıklığı (%) 20 ― 15 ― 13 10 ― 8 5― PA = primer aldosteronizm 2 0― Evre 1 Evre 2 Evre 3 Evre 4 Mosso L Hypertension 2003; 42(2): 161 -165
Nasıl prezente olur ? • • • Çoğu asemptomatik Karında gaz Sağ üst kadranda hassasiyet Yorgunluk Obez, Tip 2 diyabet, HT Alkol çok az ya da yok
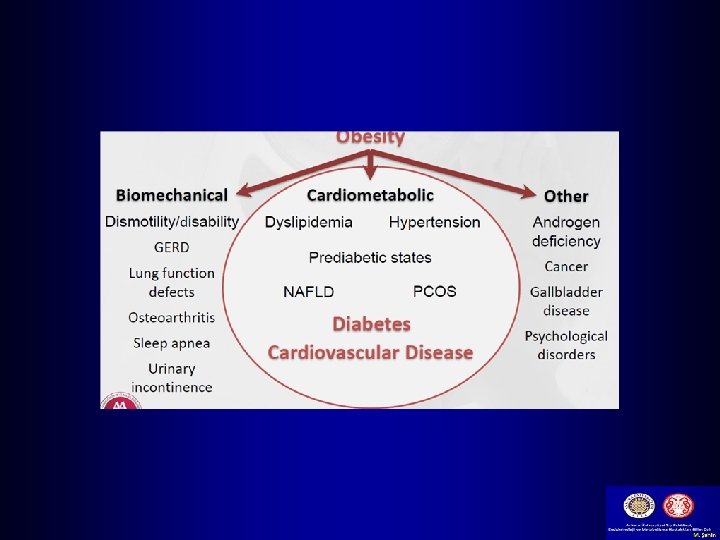
Metabolik Sendrom Obezite Dislipidemi NAFLD Diyabet Hipertansiyon
Metabolik Sendrom (Sendrom-X) ATP III criteria : Aşağıdakilerden ≥ 3 • Abdominal obezite : Etnik farklılık • (Bel çevresi > 102 cm ♂, > 88 cm ♀) • Trigliserid > 150 mg/dl • HDL < 40 mg/dl ♂, < 50 mg/dl ♀ • KB ≥ 130/85 mm. Hg • AKŞ ≥ 110 mg/dl ? ? 100 mg/dl
Obezite ve İnsulin Direnci Thrombofili Makrovasküler hastalık Santral obezite İnsulin Direnci Hyperglisemi Hipertansiyon Hiperurisemi Dislipidemi NAFLD
Teşekkürler