Human Immunodeficiency Virus Retroviruses Possess enzyme RT Reverse

 that directs synthesis of DNA from RNA after")
")






 , gp 41 (trans-membrane pedicles)")

 RTase enzyme synthesizes DNA by using RNA as template")


 based on differences in env gene")
, confined to Africa Was first isolated in India")




















 can occur during latent period. It is")









 is responsible for implementing policy")


 (kit from a different manufacturer) is reactive -- Rapid")














. In")


 testsa. ELISA b. Rapid tests- Latex Agglutination, Dot blot assay c.")



. It prolongs survival of patients")
 is approved for combination with other 2")

 + 3 rd drug Indinavir")







- Slides: 88
Human Immunodeficiency Virus
Retroviruses: Possess enzyme RT (Reverse Transcriptase) that directs synthesis of DNA from RNA after they infect host cell
CLASSIFICATION OF RETROVIRUSES Sub family Genera Virus 1. Oncovirinae Retrovirus HTLV-1(adult T cell leukemia/lymphoma) HTLV-2 (prevalent in IV abusers not known to cause human disease)
2. Lentivirus HIV-1 HIV-2 Animal virus of Visna 3. Spuma virinae Spuma virus AIDS and slow virus diseases.
HIV was previously known as HTLV-3: Human T lympho-trophic virus LAV : Lymphadenopathy associated virus ARV : AIDS related virus Zoonotic transmission from chimpanzees to humans
1 st case of AIDS: New York in 1981 Isolation of the HIV-1 virus in 1983 by Luc Montagnier and co-workers at Pasteur Institute Paris. Robert Gallo, NIH USA named it HTLV -3 in 1984. Isolation was from homosexual patients with unexplained illness.
In 1986, the first known case of HIV was diagnosed by Dr. Suniti Solmon amongst female sex workers in Chennai
MORPHOLOGY
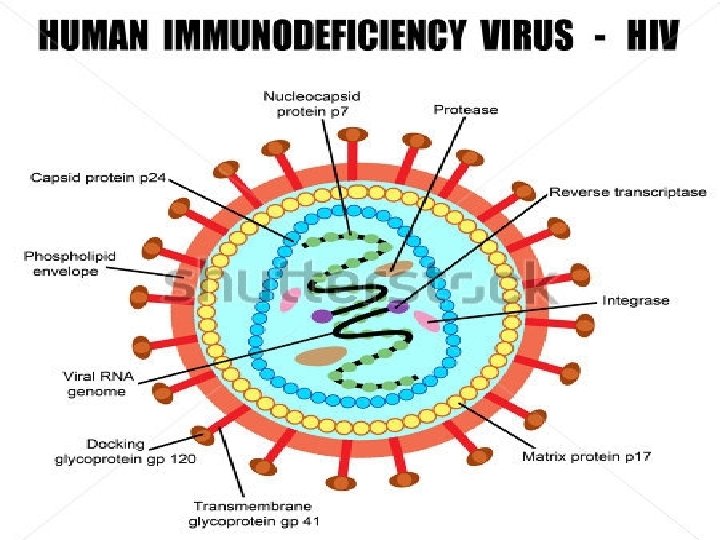
Spherical enveloped virus 80 -110 nm size Icosahedral capsid and with 2 +ve ss identical RNA (i. e. , +ve polarity)
Envelope has virus specific glycoprotein: gp 120 (Knobs) , gp 41 (trans-membrane pedicles) Genome is diploid because 2 identical molecules of +ve ss. RNA. Viral enzymes: RT, integrase & proteases closely assoc with RNA
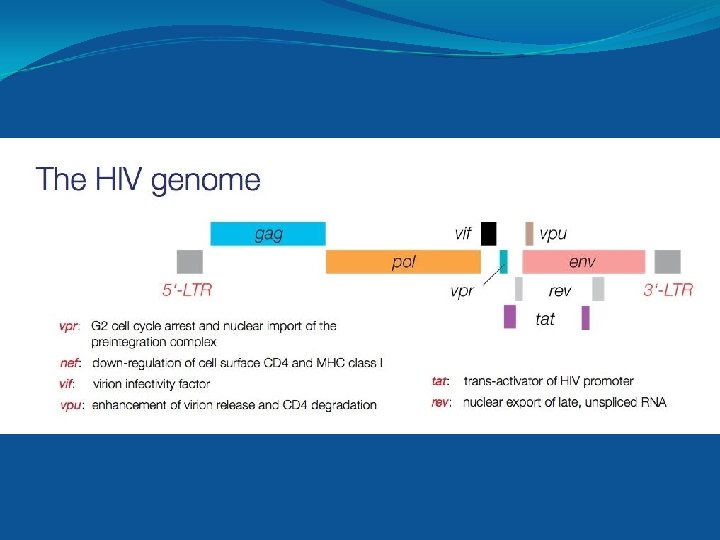
3 genes encode structural proteins—gag, pol, env 6 regulatory genes: viral pathogenesis & pathogenesis gag—encodes for the core & shell of the virus Encodes p 55: precursor protein (cleaved into p 17, p 24, p 15) p 24: core Ag: serves as important early serological marker of infection
pol– encodes viral enzymes a) RTase enzyme synthesizes DNA by using RNA as template (p 51) b) Integrase integrates viral DNA into host cellular DNA (p 32) c) Protease cleaves various precursor proteins env-- encodes gp 160 precursor gp (cleaved to form gp 120 and gp 41) gp 120: binds to CD 4 receptor gp 41: fusion protein
REGULATORY GENES Tat Transcriptional trans-activator gene essential for HIV replication Nef ‘Negative replication factor”, retards HIV replication by down regulating CD 4 expression Rev ‘Regulator of virus gene’ : enhances expression of structural proteins Vif “virion infectivity factor”, a protein that increases the infectivity of the HIV particle. Vpu “Viral protein U” downregulates CD 4 & helps virions bud from host cell. Vpr “Viral protein R” accelerates the production of HIV proteins Vpx vpx is found in HIV-2 related to vpr LTR Long terminal repeat: provide promoter, enhancer & integration signals
Antigenic variation and diversity Extensive antigenic diversity: high rates of mutation Due to error prone nature of RT enzyme Most mutations in env gene. Env proteins main target for Abs Mutation in env gene results in: 1. HIV evades hosts immune response 2. Vaccination difficult
Two serotypes of HIV (1 & 2) based on differences in env gene HIV-1: has 3 distinct groups- M, N, and O M: Worldwide, 10 subtypes/ clades (A-J) Subtype A West Africa aa Subtype B Europe, America, Japan, Australia (transmitted through blood & homosexual contact) Subtype C Most common worldwide including India & China (transmitted heterosexually)
HIV-2 comprises 8 groups (A-H), confined to Africa Was first isolated in India in 1991 Group A most common
PATHOGENESIS OF HIV INFECTION Modes of transmission: 1. Exposure to infected blood and blood products 2. Sexual exposure 3. Injection drug abuse 4. Vertical transmission Viral load is maximum in blood, genital secretions & CSF, variable in breast milk & saliva. Zero to minimal in urine & other body fluids
Epidemiology-
Epidemiology…………. . 78 million infected, 39 million deaths worldwide About 35 million living with HIV (global prevalence of 0. 8%) In India: prevalence 0. 27%, 20. 8 lakh adults 7 1. 4 lakh children PLHA Andhra Pradesh, Maharashtra, Karnataka: PHLA High prevalence: Northeast ( Nagaland)
REPLICATION OF HIV
1. Entry of HIV: – binding of gp 120 env protein to CD 4 on cell surface. Chemokine Co-receptor: on cell surface. (CXCR 4: T cells, CCR 5: Macrophages) 2. gp 41 mediates fusion of viral envelope with host cell membrane and virion enters the cell like an injection
3. Uncoating of the virus inside host cell 4. RNA dependant DNA polymerase transcribes the genome RNA into ds. DNA 5. Integration: ds. DNA integrates into host cell DNA 6. Viral m. RNA is transcribed from proviral DNA by host cell RNA polymerase and translated into viral structural & regulatory proteins 7. Assembly and release of virions: Virus assembles in cytoplasm released from cell by budding.
PATHOGENESIS AND IMMUNITY HIV infects helper T cells & kills them, Result- suppression of CMI, predisposition to opportunistic infections, certain cancers e. g. Kaposi’s sarcoma and lymphoma. HIV also infects brain monocytes & macrophages – formation of multinucleated giant cells and significant CNS symptoms.
A person infected with HIV is considered infected for life Reason- integration of viral DNA into the DNA of infected cells. Antibodies are produced but they neutralize the infectivity of the virus poorly. Immunity is incomplete because infection and antibodies co-exist. This is one of the reasons in failure of development of effective vaccines.
Abnormalities of B cells also occur. Polyclonal activation of B cells occurs. High immunoglobulin levels and also auto immune diseases seen. e. g. thrombocytopenia.
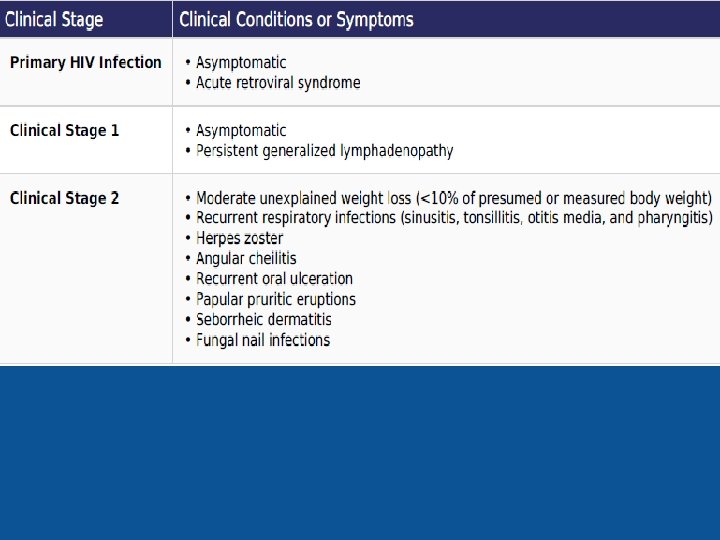
SPECTRUM OF HIV INFECTION 1. Acute retroviral syndrome 2. Asymptomatic stage 3. Persistent generalized lymph-adenopathy 4. Symptomatic HIV infection 5. AIDS
Acute retroviral syndrome: Following infection, HIV carried to lymph nodes Further multiplication inside T cells Destroys T cells, HIV spills into blood stream: PRIMARY VIREMIA. Flu like illness 3 -6 wks after exposure: drop in CD 4 T cell count
Asymptomatic stage: Effective immune response develops in 1 month CMI ( CD 8 T cells) & HIV specific Viremia drops & CD 4 countneutralizing stabilizes Abs develop CLINICAL LATENCY , not microbiological latency Immune response cannot clear infection completely: viral replication Clinical latency (10 -30 yrs)
PERSISTENT GENERALISED LYMPHADENOPATHY: Due to viral replication in lymph nodes 30% of infected people develop lymph-adenopathy PGL: defined as enlarged lymph nodes of more than 1 cm size in 2 or more contiguous sites persisting for at least 3 months
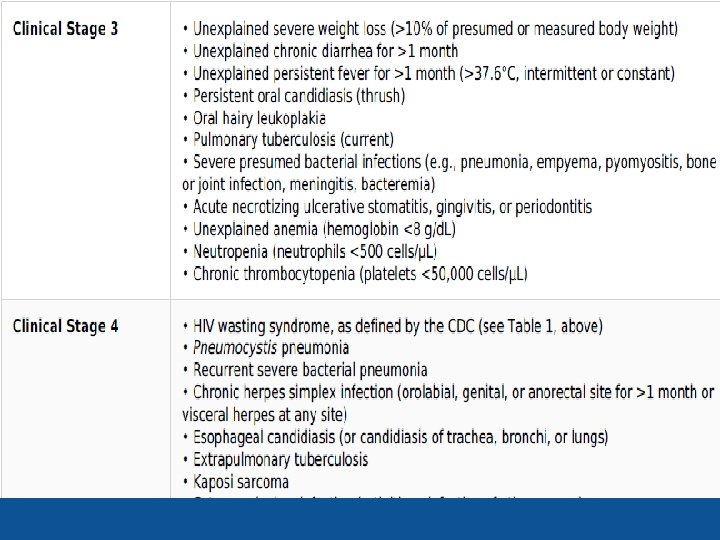
Symptomatic HIV infection: After clinical latency CD 4 count starts falling Patient begins to develop constitutional symptoms such as: ØUnexplained diarrhea lasting > than 1 month ØWeight loss > 10% body weight, fatigue, malaise, night sweats Mild opportunistic infections: oral thrush
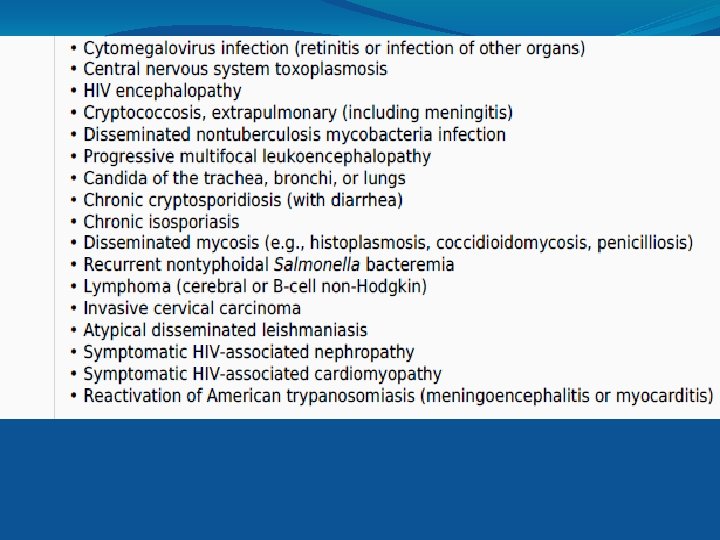
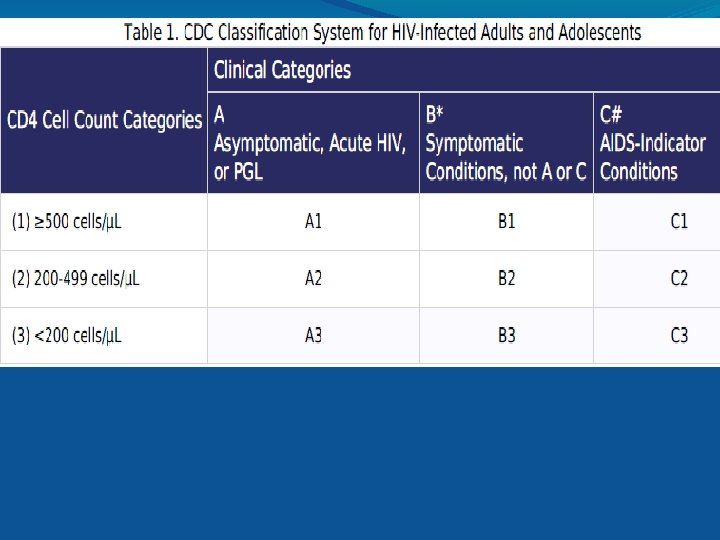
AIDS: Advanced stages of HIV infection called AIDS Rapid fall in CD 4 T cell count (usually < 200 cells/ul) High viral load Lymphoid tissue totally destroyed & replaced by fibrous tissue Plethora of opportunistic infections HIV induced manifestations: HIV encephalopathy
Clinical features and staging of infection Clinical staging and case definition of HIV for resourceconstrained settings were developed by the WHO in 1990 and revised in 2007. Staging is based on clinical findings that guide the diagnosis, evaluation, and management of HIV/AIDS, it does not require CD 4 cell count. Early – acute stage Middle- latent stage Late or immunodeficiency stage
Early or acute begins 2 -4 weeks of infection. A mononucleosis like picture- fever, lethargy, sore throat and generalized lymphadenopathy is seen. Maculo-papular rash is also seen.
Leucopenia CD 4+ cell count usually normal. Antibodies to HIV typically appear within 6 -8 wks of infection. WINDOW PERIOD
Middle / LATENT stage a long latent period Asymptomatic, viraemia is low or absent, virus relicating in lymph nodes The virus is replicating but disease is latentclinical latency only but virus does not enter latent stage. Infected person produces approximately 10 billion new viruses every day.
This viral load can be estimated by using an assay for viral RNA in patient plasma. Amount of viral RNA will be a guide to treatment and prognosis e. g. if drug regimen fails to decrease the viral load it can be changed. Prognostically if patient has >100, 000 copies of viral RNA/ ml plasma, he is more likely to progress to AIDS than the patient having fewer than 100, 000 copies.
Syndrome called AIDS related complex (ARC) can occur during latent period. It is characterized by persistent fever, fatigue, weight loss and lymphadenopathy. ARC often progresses to AIDS.
Late stage is AIDS – Decline in No. of CD 4 cells to <400 cells/ ul Increase in severity of opportunistic infections.
Opportunistic infections and malignancies commonly associated with HIV infection I. BACTERIAL – 1. Mycobacterium tuberculosis- disseminated and extrapulmonary 2. M. avium intracellulare complex 3. Salmonella – recurrent septicaemia II. VIRAL – 1. Cytomegalo virus (retinitis) 2. Herpes simplex (usually disseminated) 3. Varicella-Zoster 4. Hepatitis B 5. Progressive multifocal Encephalopathy
III. FUNGAL 1. Candidiasis 2. Cryptococcosis 3. Aspergillosis 4. Histoplasmosis 5. Coccidioidomycosis IV. PARASITIC 1. Pneumocystis jerovicii 2. Toxoplasmosis 3. Cryptosporidiosis 4. Isosporiasis 5. Microsporidiosis 6. Generalised Strongyloidiasis
V. MALIGNANCIES 1. Hairy cell leukoplakia 2. Kaposi’s sarcoma 3. B-cell lymphoma or non-Hodgkin’s lymphoma
Neurological symptoms- common in AIDSdementia, neuropathy which is either due to AIDS or opportunistic infections.
Pediatric AIDSClinical symptoms by 2 yrs of age. Death in another 2 yrs. As immune system is not developed during initial infection, devastating effects of HIV seen. Lymphoid interstitial pneumonitis, pneumonia, severe oral thrush, encephalopathy, severe wasting, bacterial sepsis, hepatosplenomegaly and growth retardation.
Children with perinatal HIV-1 acquisition have poor prognosis. High rate of disease progression seen during the first few years of life. High level of plasma HIV-1 load will predict infants at risk of rapid progression of disease.
Pattern of replication is different than in adults. Viral RNA load levels are generally low at birthmeaning infection is acquired at birth Within 2 months of life RNA load increase rapidly and slowly decline till 24 months meaning immature immune system unable to cope with infection. Also a small <5% display transient infection. Some lucky infants may even clear the virus.
Lab diagnosis Serological detection of antiviral Antibodies. Measurement of viral nucleic acids or Antigens Virus isolation Relevant test for opportunistic pathogens if suspected Miscellaneous tests
In India, the National AIDS Control Organization (NACO) is responsible for implementing policy on the control of AIDS and HIV infection. Consent Confidentiality Pre & post test counselling
Serological detection of antiviral Antibodies. Detection of anti HIV Abs : mainstay of HIV diagnosis SCREENING ASSAYS Rapid simple tests High sensitivity Need to be confirmed Egs: Immuno-chromatographic tests, ELISA Ags used: gp 120, gp 160, gp 41
ELISA kits commercially available. 1 st generation ELISA: uses crude preparation of HIV Ag 2 nd generation ELISA: uses recombinant antigens of HIV 3 rd generation ELISA: synthetic oligopeptide Ags 4 th genertaion ELISA: detects both HIV abs and p 24 Ag Positive results of screening test need to be confirmed
If repeat ELISA (E) (kit from a different manufacturer) is reactive -- Rapid test (R) like Cylinder or Cassette ELISA, Immunochromatographic, coated Particle Agglutination, Immunoperoxidase or Dipstick test can be performed If a specimen is reactive in 2 different system a third simple test (S) can be added.
Confirmatory test: needed to resolve any discordant result. Western Blot technique Though considered Gold standard, the test is costly and require experienced technologist.
What is Western blot? Viral proteins are displayed by acrylimide gel electrophoresis, transferred to nitrocellulose paper called the blot and reacted with patients serum. If Abs are present they will bind to viral proteins predominantly to gp 41 or p 24 protein. Enzymatically labeled anti-human Ig. G is then added. A color reaction reveals the presence of HIV Ab in the patient’s serum.
Western Blot technique- confirmatory test Antibodies to specific HIV proteins of Specific mol. wt can be determined. gp 160 - precursor of envelope glycoprotein gp 120 - outer envelope gp of virion- SU p 66 – reverse transcriptase and RNAse – polymerase gene product p 55 - precursor of core protein- polyproteins from gag gene p 51 – reverse transcriptase – RT
gp 160, gp 120, gp 41, p 24 most commonly detected.
Virus isolation Specimen- lymphocytes in peripheral blood Technique used: Co- cultivation of test sample with uninfected, mitogen stimulated peripheral blood mononuclear cells. Viral growth is detected in 7 -14 days – culture supernatant is tested for reverse transcriptase activity or for virus specific Ag p 24. Time consuming, laborious,
Measurement of viral nucleic acids or Antigens Amplification assays – RT PCR (Reverse transcriptase PCR) and b-DNA tests b. DNA –amplifies viral RNA by sequential oligonucleotide hybridization steps.
These 2 tests can be made quantitative when reference standards are used. These tests are very sensitive and form the basis for plasma viral load determination. The HIV- RNA levels are important predictive markers of disease progression and valuable tools to monitor antiviral therapies.
REMEMBER 1. During 1 st month after infection, Ab tests are negative, so diagnosis of acute HIV infection typically cannot be made by these tests. 2. So at this time if facility is available—p 24 antigen test or PCR assay is the choice. 3. Approximately 12 -15 days of infection increase in HIV RNA can be detected by PCR assay. 4. By 15 -18 days increase in p 24 antigen can be seen in those patients who had their antibody tests negative.
Relevant test for opportunistic pathogens if suspected Various tests for bacteria fungus, virus and cancer diseases Kaposi’s sarcoma- biopsy and histopathology. Herpes-8 implicated. Predilection for homosexual men. Arises from endothelial cells of blood vessels causing bluish purple, raised irregular lesions arising in many sites. viz skin, mouth, gut, lungs and eye.
Patients with low CD 4+ T cell count may develop T cell lymphoma or B cell lymphoma
Fungi- KOH mount, Culture, LPCB.
Protozoa – cryptosporidiosis- cold AFB staining, Pneumocystis jiroveciibiopsy and fluorescent stain,
Viruses – isolation, culture, inclusion bodies, Tzanck smear. CMV retinitis Inclusion bodies Tzanck smear
Bacterial –MAC- blood culture, M. tuberculosisculture
Immunologically active cells are counted by Flow cytometry (fluorescence activated cell sorting). In the test, patient’s cells are labeled with monoclonal Antibody to the protein specific to the cell of interest. E. g. CD 4 T cell protein to detect the number of helper T cells.
Monoclonal Ab is tagged with fluorescein or rhodamine. Single cells are passed through a LASER beam and number of cells that fluoresce are counted by a machine called Fluorescence Activated Cell Sorter (FACS) this count is useful for monitoring prognosis of the disease.
Others platelet - thrombocytopenia, Increased Ig. G and Ig. A levels indicate polyclonal activation, Decreased CMI as indicated by Skin tests LN biopsies for abnormalities.
1. Screening (E/R/S) testsa. ELISA b. Rapid tests- Latex Agglutination, Dot blot assay c. Simple tests- particle agglutination test 2. Confirmatory tests Western blot assay 3. Supplemental tests: Detection of p 24 antigen Detection of viral nucleic acid - in situ hybridization - PCR
Anti retro viral therapy
Anti-retroviral drugs: I. NUCLEOSIDE RT inhibitors Zidovudine, stavudine, lamivudine III. NUCLEOTIDE RT inhibitors- Tenofovir III. NON-NUCLEOSIDE RT inhibitors Nevirapine , efavirenz, III. PROTEASE inhibitors Saquinavir, Ritonavir, Indinavir IV. INTEGRASE inhibitor: raltegravir V. FUSION inhibitors: Efuvirtide VI CCR 5 RECEPTOR inhibitor: Maraviroc
Therapy with combination is called HAART-highly active antiretroviral therapy Currently for advanced disease- regimen of 2 nucleoside inhibitor and protease inhibitor is tried.
Most common- AZT (azidothymidine, Zidovudine, Retrovir- nucleoside inhibitor). It prolongs survival of patients by preventing opportunistic infections, but does not eliminate virus completely. It inhibits virus at the proviral DNA synthesis. It cannot cure infected cell already with integration of copy of genome. Resistance of HIV to AZT is noted. Side effects- severe hematologic side effects can limit its use. So to reduce these AZT is combined with ddi and ddc to lower the dose.
Non-nucleoside inhibitors of reverse transcriptase Nevirapine (viramine) is approved for combination with other 2 drug regimen. AZT, ddi+Nevirapine—decreases viral RNA load.
Protease inhibitors Saguinavir, ritinovir, Indinavir + AZT are also effective. Protease inhibitors can cause abnormal fat deposition in specific areas of body- back & neck “Buffalo hump” appearance. This is a type of lipodystrophy , cause not known. Resistant mutant viruses are rare occurrence. RESISTANCE TO ANY ONE DRUG CONVEYS RESISTANCE TO ALL.
Needle stick injury- 2 days AZT+3 TC (lamivudine) + 3 rd drug Indinavir added. HIV infected children-AZT perinatally to HIV infected mothers and neonates. Also ideally HIV infected mothers should not breast feed.
Treatment to prevent opportunistic infections. Trimethoprim-sulphamethoxazole- Pneumocystis Flucanazole-cryptococcal meningitis. Ganciclovir-CMV retinitis. Oral antifungals-clotrimazole-Thrush by candida.
Vaccine No vaccine is available for human use A vaccine containing recombinant gp 120 protects nonhuman primates against challenge by HIV and HIV infected cells. Vaccine should be therapeutic as well as protective. Therapeutic- should boost anti. HIV immune response, decrease number of virus infected cell, delay the onset of AIDS. Protective-Prevent infection or disease in the uninfected.
Difficulties HIV mutates rapidly. It is not expressed in all the cells that are infected. It is not completely cleared by host immune response after primary infection. Emergence of neutralization resistant mutants because of marked variation of envelope antigens.
Control measures for HIV As there are no proper drugs or vaccines, only way to avoid epidemic spread of HIV is to maintain life style that minimizes or eliminates high risk factors. No cases have been documented as a result of common exposures like sneezing, coughing, sharing meals or other casual contacts. HIV can be transmitted by blood screening of blood donors has decreased the spread of HIV by blood transfusion.
Universal precautions Due to the advent of AIDS, Hep B and other blood borne infections a set of mandatory precautionary measures are to be followed by all health care personnel.
Wash hands before and after all patient and specimen contact Handle the blood of all patients as potentially infectious Wear gloves for potential contact with blood and body fluids
Place used syringes immediately in nearby impermeable container ; DO NOT recap or manipulate needle in any way Wear protective eyewear and mask if splatter with blood and body fluids is possible.