BDSIII Fixed Prosthodontics Pharmacology COMMONWEALTH OF AUSTRALIA Copyright

BDSIII: Fixed Prosthodontics & Pharmacology

COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING This material has been reproduced and communicated to you by or on behalf of The University of Adelaide under Part VB of the Copyright Act 1968 (the Act). The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. The AUDSS assumes no responsibility or liability for any information, materials or other content provided by any of our student lecturers. All content is viewed and used by you at your own risk and we do not warrant the accuracy or reliability of any of the lecture material. The views expressed are those of the individual contributors and not necessarily those of the AUDSS of Adelaide School of Dentistry. Do not remove this notice.

Fixed Prosthodontics Definitions galore Direct v indirect Connector Crown Abutment Inlay/onlay Veneer Bridge Post Retainer Core …

Crown Direct v indirect Inlay/onlay Veneer Bridge

Post Core

Post Core

Crowns - indications: protection, occlusion, replacement, retainer, tooth-modifications, aesthetics - contraindications: OH, cost, age/ill health, excess removal of tooth structure - considerations: occlusion, endodontic status, future of tooth (i. e. perio), restorability, future of dentition, other tx req

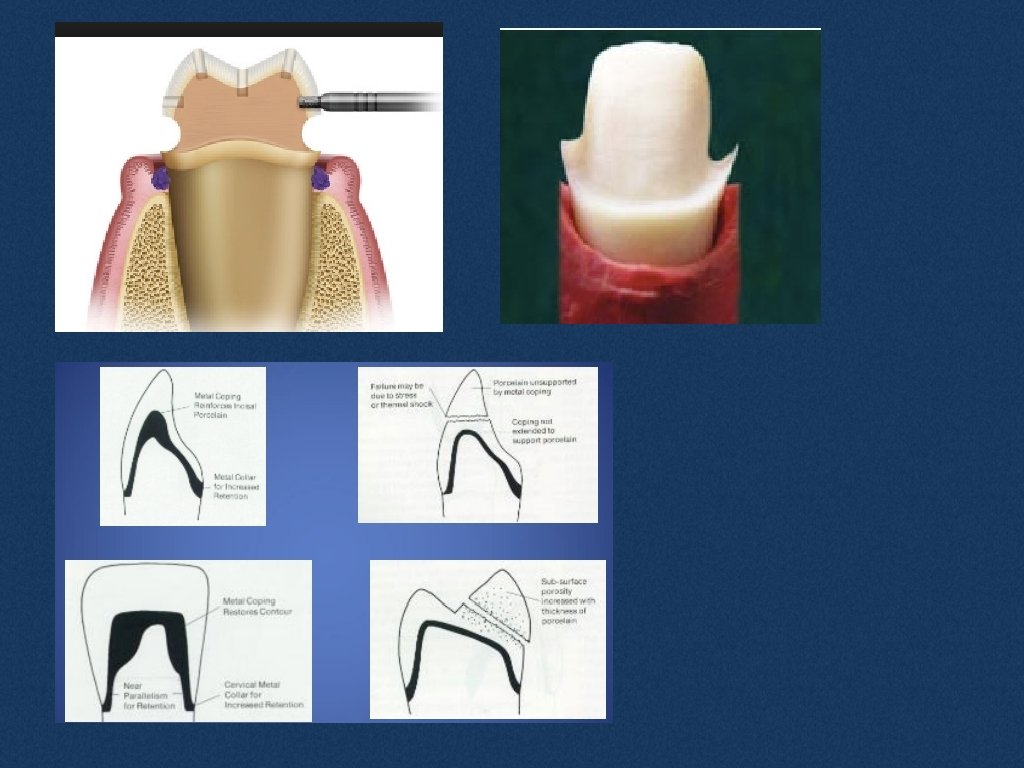
Crown-prep Principles - preserving tooth structure - preserving the periodontium - structural durability - marginal integrity

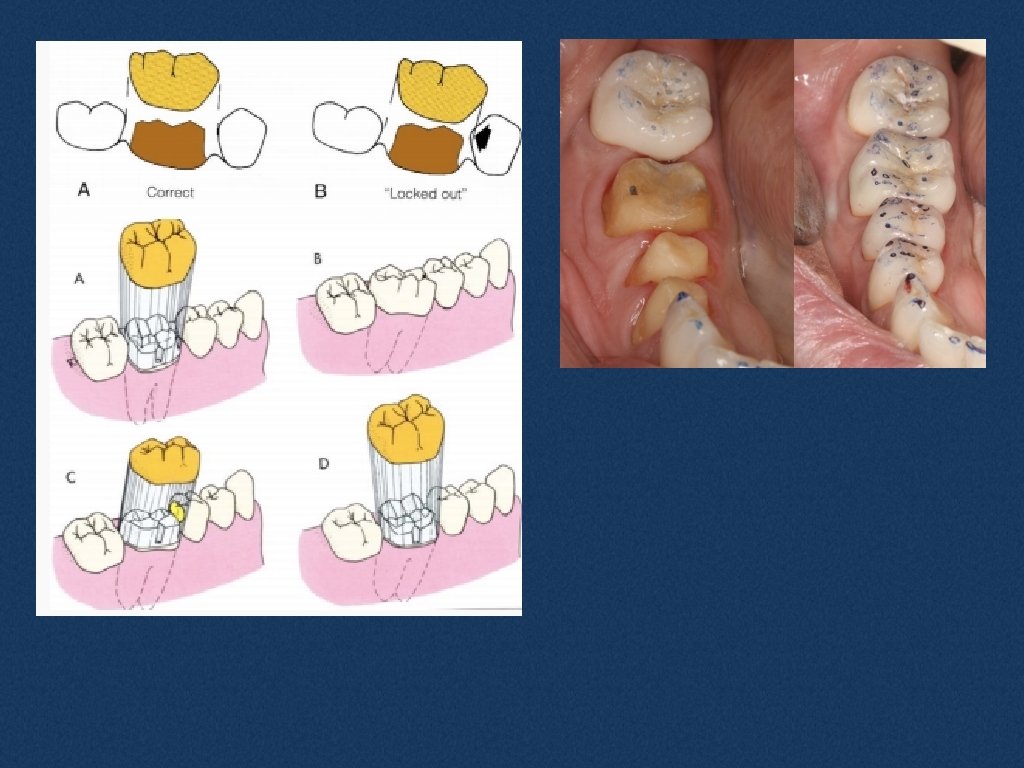
- retention and resistance form

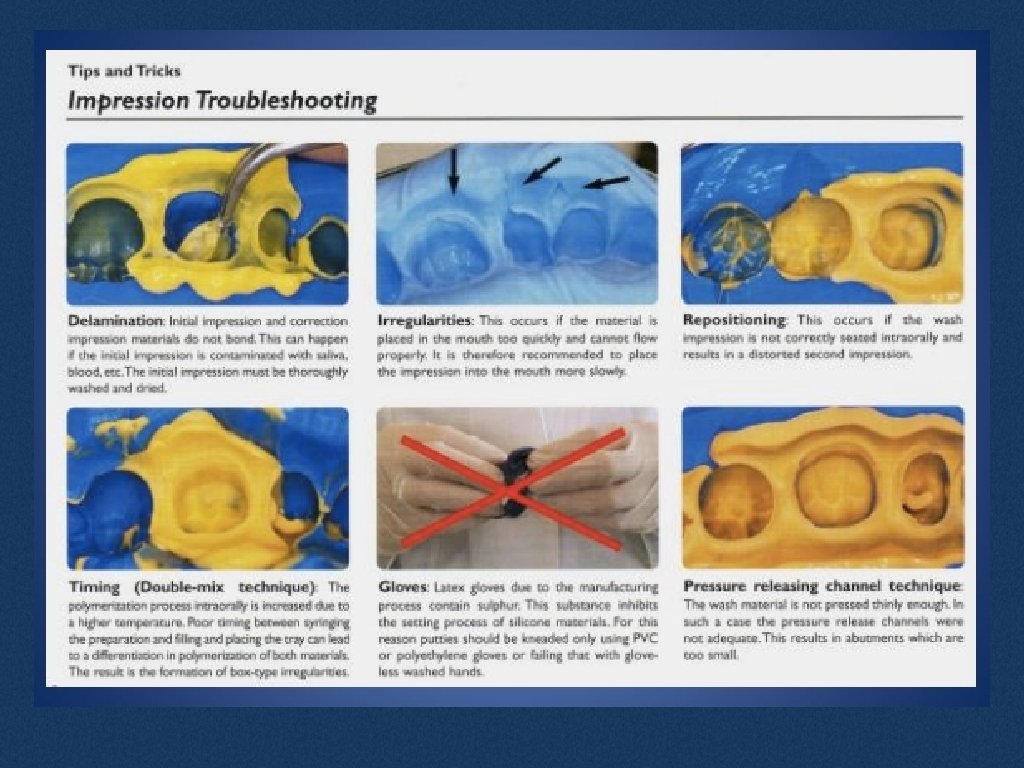
- soft tissue management and secondaries Do you need retraction cord? Consider where your margins are and moisture control 2 cord technique is “gold standard” - cord sz 000 -4 haemostastic solution = Al. Cl (Haemodent), Astringent (Fe. SO 4) Primary cord = whys it there? secondary cord = ? Dual viscosity technique Impression materials = PVS (Imprint III, Honigum) and PE (Impregum), most critical reason for one or the other? LB, HB Temp = custom made (Pro. Temp 4), celluloid, polycarbonate

Pharmacology
 What is the body")
Pharmacokinetics vs pharmacodynamics Pharmacokinetics (effect of body on the drug) What is the body doing to the drug? • Absorption • Distribution – throughout the body • Eliminating: excretion/metabolism • Factors, which alter the concentrations of drug in body: disease, age, other drugs, genetics Used to design drug dosage Pharmacodynamics (effect of drug on the body) • • • Pharmacological response: • Describes the functional change resulting from interaction between drug and body • Paracetamol relieves pain is antipyretic • Those are the pharmacodynamics properties of paracetamol • Drug interactions POTENTIATE the effect of the drugs

Examples 1. Increased risk of drowsiness and difficulty driving in an elderly patient on amitriptyline (antidepressant) who is started on diazepam (sedative). Pharmacodynamic 2. Increased sedation with codeine and temazepam (benzodiazepine for sleeping – similar to Valium) Pharmacodynamic 3. Ineffective antibacterial activity when using doxycycline with antacid Pharmacokinetic 4. Increased bleeding with warfarin and ibuprofen Pharmacokinetic 5. Increased risk of nausea and vomiting in elderly patients taking digoxin (prevent myocardial infarction) and ibuprofen Pharmacokinetic 6. Antibiotics and milk Pharmacokinetic

Examples 7. Antifungal drug and Antacid – fungal infection persists Pharmacokinetic 8. Increased risk of bleeding with warfarin (anticoagulant) and aspirin (antiplatelet agents) Pharmacodynamic 9. Increased risk of seizures in an elderly patient on lithium (mood stabiliser) given an ACE inhibitor. Pharmacokinetic 10. Increased risk of drowsiness and difficulty driving in an elderly patient on amitriptyline (anti-depressant) who is started on diazepam (sedative) Pharmacodynamic 11. Increased risk of ataxia and other adverse effects of phenytoin (anti-convulsant) in a patient also given cimetidine for acid suppression. Pharmacokinetic 12. Increased risk of bleeding in patient stabilized on warfarin (anticoagulant) and carbamazepine (anticonvulsant) – whose carbamazepine is subsequently ceased. Pharmacokinetic

Therapeutic index • Measures drug safety • TD 50 and TC 50 = minimum dose/plasma conc toxicity • ED 50 and ED 50 = minimum dose/plasma conc effect

Therapeutic index • Paracetamol has a narrow therapeutic index FALSE • Caffeine has a wide therapeutic index TRUE • Morphine has a wide therapeutic index FALSE • Ibuprofen has a narrow therapeutic index FALSE

Enzyme inhibitors vs inducers Enzyme Inducers • • Increase metabolism of the drug faster clearance Exception: prodrug – where the active metabolite causes the effect (codeine) Enzyme Inhibitors • Decrease metabolism and clearance • Therefore drug is kept longer in the body • Increased toxicity can be fatal for small TI drugs

Enzyme inhibitors vs inducers Enzyme inducers • • • Phenytoin Carbamazepine Rifampicin Cigarette/smoke Barbiturates St Johns Wort Enzyme inhibitors • • • Grapefruit Azole antifungals Cimetidine (acid suppression) Macrolides i. e. Erythromycin (except azithromycin) Sulphonamides

Triple whammy • NSAID + Diuretic + ACEI RENAL FAILURE Detrimental to kidney function by reducing blood flow to the glomerulus and reducing GFR
- Slides: 22