DR RAJESH KF CORONARY ARTERY ANOMALIES CAAs has




 LAD")



 Usually involves anterior/left surface of")
 LCA from posterior facing sinus (2) Cx from")





 a. RCA from")





 Located in upper anterior IVS(Derived from conal septum) Recogonised by systolic phasic")
 Common in TOF")
 (1) Posterior AV groove or retrocardiac")
 Between aorta and PA (2)")

 Anterior to PA (2) Intraseptal")
 Posterior AV groove")






 with respect")


 More than 1% of incidence Most commonly associated with")








 or guide catheter")


 Coronary anomalies (total) 110 (5. 64)")
 Ostial atresia Ostial stenosis ALCAPA Coronary fistula")

 ALCAPA , LCA")








- Slides: 63
DR RAJESH KF CORONARY ARTERY ANOMALIES
CAAs has a global incidence of 5. 64% Incidence of CAA related sudden death is 0. 6%
Normal Features of Coronary Anatomy FEATURE RANGE No. of ostia 2 to 4 Location Right and left anterior sinuses(upper midsection) Proximal orientation 45° to 90° off the aortic wall Proximal common stem Only left (LAD and Cx) Proximal course Direct from ostium to destination Mid-course Extramural (subepicardial) Branches Adequate for the dependent myocardium Essential territories RCA (RV free wall), LAD (anteroseptal), OM (LV free wall) Termination Capillary bed
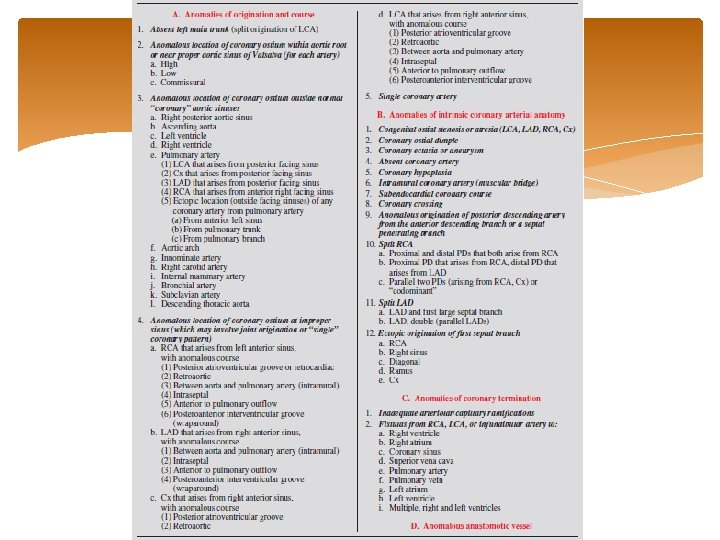
CLASSIFICATION OF CORONARY ANOMALIES
Anomalies of origination and course Absent left main trunk (split origination of LCA) LAD and Cx originates from LCS without common trunk Occurs in about 1% More frequent with BAV No clinical consequences Coronary ostia are smaller JL catheter for selective cannulation of LAD and amplatz left catheter for LCX
Anomalies of origination and course Anomalous location of coronary ostium within aortic root or near proper aortic sinus of Valsalva a. High b. Low c. Commissural High origin of LCA engaged with Amplatz left, MP catheter High origin of RCA engaged with Amplatz catheter
Anomalies of origination and course Anomalous location of coronary ostium outside normal aortic sinuses a. Right posterior aortic sinus b. LV , RV , PA , Aortic arch, Descending thoracic aorta, Innominate artery , Right carotid artery , IMA , Bronchial artery , Subclavian artery c. Pulmonary artery
Ectopic Coronary Ostium in NCS Benign anomaly Most commonly involves LCA ostium Difficult cannulation-unexpected location, tangential or slitlike nature Nonselective angiography-longer than usual LMCA RAO and straight lateral projections are most useful For selective catheterization Amplatz or Multipurpose curved catheters offer best chance of success
Ectopic Coronary Ostium Arising Outside the Aortic Root(Ascending Aorta) Usually involves anterior/left surface of aorta Frequently have slit like orifices and tangential proximal course along aortic wall RCA is most frequently ectopic artery Predisposed to more atherosclerosis Association with Congenital aortic valve anomalies
Ectopic Coronary from Pulmonary artery (1) LCA from posterior facing sinus (2) Cx from posterior facing sinus (3) LAD from posterior facing sinus (4) RCA from anterior right facing sinus (5) Ectopic location (outside facing sinuses) (a) From anterior left sinus (b) From pulmonary trunk (c) From pulmonary branch Smith A. , Arnold R. , Anderson R. H. , Wilkinson J. L. , Qureshi S. A. , Mc. Kay R. Anomalous origin of the left coronary artery from the pulmonary trunk. J Thorac Cardiovasc Surg 1989; 98
ALCAPA LCA arises from PA usually from left posterior facing sinus Fetus-both coronary arteries receive forward flow Early after birth - Anterolateral infarct and slight retrograde flow from LCA to PA 15% of patients-myocardial blood flow can sustain myocardial function at rest or even during exercise Adult-Enlarged RCA and collaterals and significant retrograde flow into PA
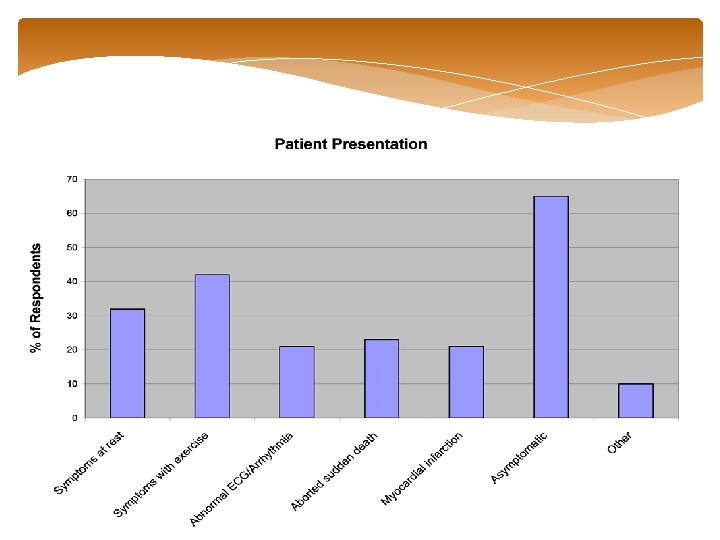
Clinical features Paroxysmal attacks of acute discomfort precipitated by feeding CHF at 2 to 3 month Physical examination-CHF, MR Abnormal Q waves in leads I, a. VL, and precordial leads V 4 to V 6 Older children and adults -may be asymptomatic or have dyspnea, syncope, or exertional angina Sudden death after exertion
Echo Abnormal origin of LCA Flow passes from RCA into PA Enlarged RCA RWMA and mitral regurgitation Aortic root angiography Dilated RCA large collaterals-filling of LCA and passage of contrast material to MPA
Treatment Ligation of LCA at its origin Direct reimplantation of origin of LCA into aorta (with a button of PA around the origin) Ligation of origin of LCA and reconstitution of flow through it with subclavian arterial or SVG Takeuchi procedure- aortopulmonary window is created and a tunnel fashioned that directs blood from aorta to LCA
Anomalous Origination of RCA, LAD or Cx Artery From PA Benign condition Typically recognized by atypical angina, systolic heart murmur , abnormal stress test or angiography In absence of major clinical manifestations not an indication for surgery
Anomalies of origination and course Coronary ostium at improper sinus (ACAOS) a. RCA from left anterior sinus b. LAD from right anterior sinus c. Cx from right anterior sinus d. LCA from right anterior sinus ARCA~ 6 times more prevalent than ALCA has a higher risk of SCD
Anomalies of origination and course Sudden cardiac death associated with four risk factors • Slit-like coronary orifice • Acute angle of take-off from aorta • Presence of aortic intramural coronary arteries • Inter-arterial course between aorta and PA
Echo Difficult by angiography MRI or CT is more sensitive
Abnormal crossing pathways Retrocardiac Path is behind mitral and tricuspid valves in posterior AV groove Retrocardiac Angelini et al
Retroaortic Most common Specifically involve origination of Cx artery from right sinus of Valsalva Incidence in general population range from 0. 1 to 0. 9% No clinical consequences
Preaortic Between the aorta and PA Osial abnormalities are usual intramural course within the aortic root and adherent to it for about 1. 5 cm Rarely systolic compression lead to SCD
Intraseptal(supracristal) Located in upper anterior IVS(Derived from conal septum) Recogonised by systolic phasic narrowing during CAG Septal perforators
Prepulmonary (precardiac) Common in TOF
RCA from left anterior sinus, with anomalous course(ARCA) (1) Posterior AV groove or retrocardiac (2) Retroaortic (3) Between aorta PA (Most common, 30% mortality) (4) Intraseptal (5) Anterior to pulmonary outflow (6) Posteroanterior interventricular groove (wraparound)
LCA from right anterior sinus, with anomalous course (1) Between aorta and PA (2) Anterior to PA (3) Retroaortic (4) Intraseptal (5) Posterior AV groove (6) Postero-anterior interventricular groove
Angiographic appearace RAO
LAD from right anterior sinus, with anomalous course (1) Anterior to PA (2) Intraseptal (3) Between aorta and PA (4) Posteroanterior interventricular groove (wraparound)
Cx that arises from right anterior sinus, with anomalous course (1) Posterior AV groove (2) Retroaortic Angiography Long LMCA segment Small cx branch RAO view shows dot of retro aortic course
Current recommendations Symptomatic patients Unroofing Reimplantation Asymptomatic patient Demonstrable ischemia: repair No demonstrable ischemia ALCA: repair ARCA: observe
Anomalies of origination and course Single coronary artery Incidence 0. 024% Single ostium with absence of an ostium in opposite sinus No other coronary artery from an ectopic site 40% associated with cardiac malformations(TGA, TOF, TA, coronary-cameral fistulas, and BAV)
Less tangential origin or ostial ridge pathology than ectopic CA with independent ostia Coronary blood flow is not affected Incidence of atherosclerotic disease not increased Ostial obstruction (large guiding catheter or directional atherectomy device) -poorly tolerated Angioplasty of common trunk is absolutely contraindicated
Angiographic classification Lipton et al
Coronary artery atresia Characterized by ostial dimple in left or right aortic sinus terminates in a cordlike fibrotic structure without a patent lumen Proximal occluded segments have larger diameter Collaterals Stress testing demonstrate myocardial ischemia Seen in PA with intact IVS
Coronary artery isolation Variant of ostial atresia Juxtaposition of abnormal aortic cusp with aortic sinus wall lead to obliteration of underlying coronary ostium
Anomalies of intrinsic anatomy Coronary hypoplasia Angiographic appearance -small diameter(usually <1 mm) with respect to apparent area of dependent myocardium Myocardial fibrosis and segmental hypokinasia are frequent Local reversible ischemia during stress testing with myocardial nuclear scintigraphy Terminology is incorrect when dependent myocardial bed is actually served by alternative sources (unusual coronary patterns) or coronary spasm or diffuse disease
Anomalies of intrinsic anatomy Absent coronary artery Misnomer On angiographic grounds, the most frequent reason are Coronary ectopia (misdiagnosed) Coronary occlusion with lack of demonstrable collateral filling Alternative coronary artery tree pattern not recognized on angiography
Anomalies of intrinsic anatomy Coronary ectasia or aneurysm Localized dilations in a normal sized coronary artery Coronary segment diameter >50% with respect to normal Doppler coronary wire blood flow velocity - significant reduction in peak flow velocity Streamlining and slow runoff contrast media in angiography Acquired stenosis Mural thrombosis with distal embolization Aneurysmal rupture
Intramural coronary artery (muscular bridge) More than 1% of incidence Most commonly associated with ventricular hypertrophy Coronary artery segment of variable length covered by myocardial fibers Angiographic recognition of systolic narrowing Phasic narrowing of a coronary aftery may also occur in ventricular aneurysms or pericardial fibrous bands Intracoronary nitroglycerin in a 100 - to 300/microg bolus facilitates
U sign- Artery's accentuated descent from its subepicaardial location Most commonly involve proximal LAD Systolic stenosis is unlikely to cause coronary flow reduction Rare reports of spasm, thrombus and atherosclerotic change
Anomalies of intrinsic anatomy Subendocardial coronary course Coronary crossing Anomalous origination of posterior descending artery from anterior descending branch or a septal penetrating branch
Anomalies of intrinsic anatomy Split RCA a. Proximal+distal PDAs that both arise from RCA b. Proximal PDA that arises from RCA, distal PDA arises from LAD c. Parallel PDAs (arising from RCA, Cx) or “codominant”
Anomalies of intrinsic anatomy Split LAD Duplication of LAD < 1 % Population a. LAD+first large septal branch b. LAD, double (parallel LADs) c. LAD+large diagonal d. Highly dominant RCA+LAD
Anomalies of intrinsic anatomy Ectopic origination of first septal branch a. RCA b. Right sinus c. Diagonal d. Ramus e. Cx
Anomalies of coronary termination Coronary fistulas A sizable communication between a coronary artery and a cardiac cavity or any segment of systemic or pulmonary circulation
Anomalies of coronary termination Fistulas from RCA, LCA, or infundibular artery to RV, RA, CS , SVC, PA, PV, LA, LV, Multiple(right+left ventricles) Originate from left coronary artery system (50 -60%), right coronary artery system (30 -40%), or both (2 -5%) Most fistulas (90%) drain into right heart
Functional coronary fistula Definite signs of fistulous flow-feeding vessel diameter >50% expected diameter Angiographically prompt visualization of receiving structure with step up in concentration of injected substance Evidence of volume overload in affected cardiac chambers Evidence of steal involving myocardial nutrient blood flow
Use large-lumened catheters with side holes (NIH or Gensini ) or guide catheter kept in position by a 0. 014 -inch guidewire Mechanical injector Diagnose coronary fistula Identify receiving chamber or vessel Complete visualization of nutrient myocardial branches Absence of nutrient coronary branches arising from a fistulous tract should suggest alternative diagnosis-RSOV
Complications Aneurysm formation Intimal ulceration Medial degeneration Intimal rupture Atherosclerotic deposition Calcification Side branch (nutrient) obstruction Mural thrombosis Coronary rupture
Treatment Amount of dilation of fistulous vessel is more relevant than fistulous flow, symptoms and signs of myocardial ischemia Catheter based or surgical intervention at an early age(gianturco coils, double umbrella, gifca vascular closure device) Large fistulas-risk of rupture and mural clotting Reversibility of ectasia is consistently reported in pediatric age Optimal time for correction -fifth to fifteenth year of life
Incidence of Coronary Anomalies and Patterns VARIATION (%) Coronary anomalies (total) 110 (5. 64) Split RCA 24(1. 23) Ectopic RCA (right sinus) 22 (1. 13) Ectopic RCA (left sinus) 18 (0. 92) Fistulas 17(0. 87) Absent left main coronary artery 13 (0. 67) Circumflex arising from right sinus 13 (0. 67) LCA arising from right sinus 3 (0. 15) Low origination of RCA 2 (0. 1) Other anomalies 3(0. 27) Angelini P et al
FUNCTIONAL CLASSIFICATION Myocardial ischemia, primary (fixed /episodic) Ostial atresia Ostial stenosis ALCAPA Coronary fistula (rare) Muscular bridge (rare) Myocardial ischemia, secondary (episodic) ACAOS-Tangential origin, intramural course Myocardial bridge - spasm and/or clot Coronary ectasia - mural clot Coronary fistula - mural clot
Increased risk of fixed coronary atherosclerotic disease Coronary fistula ALCAPA Coronary ectasia Muscular bridge (proximal ) Secondary aortic valve disease Coronary aneurysm (ostial) Coronary fistula ALCAPA
Increased risk of bacterial endocarditis- Coronary fistula Ischemic cardiomyopathy (hibernation) ALCAPA , LCA atresia, rarely in cases of LCA origin from RCS Volume overload Coronary fistula, ALCAPA
Misdiagnosis “Missing” coronary artery “Hypoplastic” coronary artery Unusual technical difficulties during coronary angiography or angioplasty Ectopic ostia (tangential) Split left coronary artery Coronary fistula
Clinical Management: ACC/AHA Guidelines J. Am. Coll. Cardiol. 2008; 52; e 1 -e 121
Coronary Artery Patterns with Congenital Heart Defects
D-TGA Important to identify before switch Sx Facing sinuses -Sinuses adjacent to PA Nomenclature of facing sinuses depends on relationship of great vessels VSD or side-by-side GVs more associated with coronary anomalies Almost all coronaries arise from facing sinuses In 60% coronary arteries come from appropriate sinuses and branch normally Seen often with aorta anterior and to right of PA
D-TGA LCX arising from RCA and coursing posterior to PA - 20% of patients Usually with side-by-side great vessels Completely inverted-RCA arising from a left anterior sinus and LCA arising from right posterior sinus Partially inverted- LCX arising from right posterior sinus and LAD arising with RCA from left anterior sinus Various single coronary anomalies Intramural coursing
TOF 40% -abnormally long, large conus artery supplies a significant mass of myocardium 4% - LAD from RCA and passes across RVOT Occasionally single coronary artery Major arteries cross RVOT-Surgery with transannular incision more difficult Can be detected by echocardiography If anatomy is uncertain-aortic root angiography or selective coronary arteriography before Sx
L-TGA Aorta is anterior and to left of PA Coronary arteries come from facing sinuses Anterior sinus is usually noncoronary sinus LCA supplies LV but arises in right facing sinus Passes in front of PA and divides into LAD and Cx , passing in front of RAA in AV groove. RCA arises from left facing sinus and runs in AV groove in front of LAA to terminate as PDA Most common variant is SCA coming from right facing sinus.
Referances Moss and Adams' Heart Disease in Infants, Children, and Adolescents: Including the Fetus and Young Adults, 7 th Edition Myung k Park 5 th edition Hurst, s 13 th edition Morton J Kern 5 th edition Coronary Artery Anomalies: A Comprehensive Approach, edited by P. Angelini. Lippincott Williams & Wilkins, Philadelphia 1999 Coronary Anomalies: Incidence, Pathophysiology, and Clinical Relevance Paolo Angelini, MD; José Antonio Velasco, MD; Scott Flamm, MD Circulation May 21, 2002