CONGENITAL ANOMALIES OF NOSE AND PNS Embryology Nasal

CONGENITAL ANOMALIES OF NOSE AND PNS .

Embryology • Nasal cavity is first seen as nasal placode in the 4 th week of intrauterine life. • It is the thickening of ectoderm above the stomodeum. • Stomodeum is surrounded by superiorly – frontonasal prominence laterally – maxillary processes inferiorly – mandibular processes
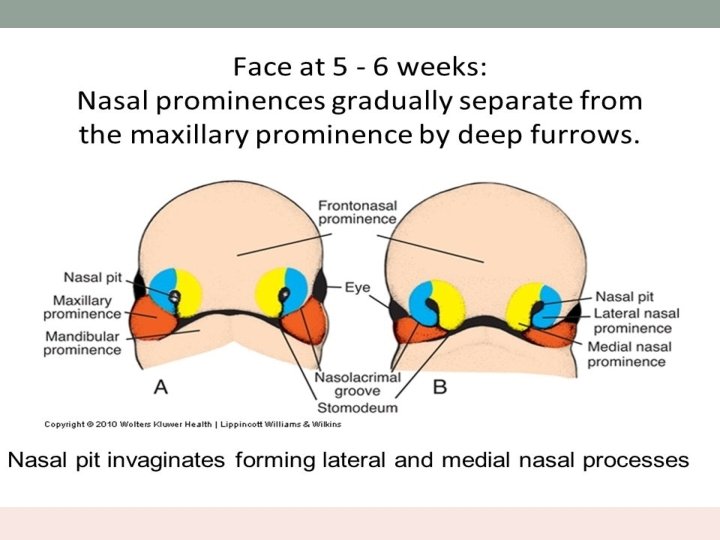

• The placode thickens and sinks into the mesenchymal tissue – olfactory pit. • Lies between the proliferating medial and lateral prominences of frontonasal process. • Medial prominences fuse to form central portion of upper lip, premaxilla and primitive nasal septum. • The primitive nasal cavity and mouth are separated by bucco nasal membrane.
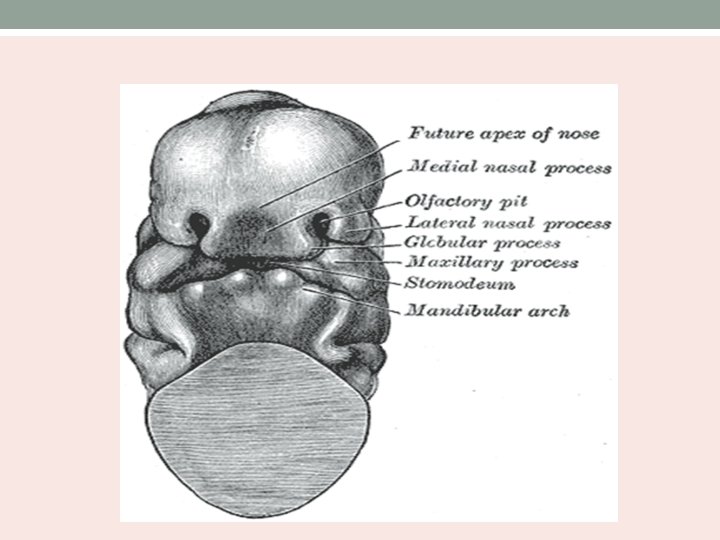


Maxillary process • It develops from the dorsal end of mandibular arch. • It joins the lateral nasal fold around the nasomaxillary groove. • Ectoderm in the region of nasomaxillary canalizes to form the nasolacrimal duct. • Lateral nasal fold of frontonasal process gives rise to nasal bones, upper lateral cartilages and lateral crura of lower lateral cartilages.

Nasal septum development • Begins with the fusion of maxillary and frontonasal processes. • Midline ridge develops from the posterior edge of frontonasal process in the roof of the oral cavity. • This ridge gives rise to nasal septum.

Development of Palate • Derived from lateral maxillary process. • These processes grow medially towards each other and nasal septum. • Initially the palatal processes lie lateral to the tongue. • Palatal processes swing medially and the fusion starts horizontally. • Fusion separates the nasal from oral cavity.

Development of PNS • At 25 weeks – 3 medial projections arise from lateral wall of nose. • Diverticula occurs between these projections towards choana. • Anterior most projection – agger nasi. • Inferior projection (maxilloturbinate) – inferior turbinate - maxillary sinus
– superior turbinate - middle turbinate - ethmoidal air cells •")
• Superior projection(ethmoidoturbinate)– superior turbinate - middle turbinate - ethmoidal air cells • Middle meatus develops between inferior and middle turbinates.

Development of maxillary sinus • First sinus to appear. • 7 to 10 weeks. • Shallow groove expanding from primitive infundibulum to the maxilla • Enlarges by absorption and expansion. • Grows till 17 years of life.

Development of ethmoid sinus • 9 to 10 weeks of gestation. • 6 to 7 folds separated by grooves appear on the lateral wall of nose. • These folds fuse to form 3 -4 crests. • They have anterior ascending and posterior descending portions. • Reach adult size by 12 years.

Development of sphenoid sinus • Arise from within the nasal capsule of embryonic nose. • Remain undeveloped until 3 years. • Reaches sella turcica by the age of 7 years • Dorsum sellae – by late teens • Basisphenoid by adult age.

Development of frontal sinus • Direct continuation of infundibulum and frontal recess. • Invades frontal bone at 4 years • First radiologic evidence is at 6 years. • Right and left frontal sinuses develop independently – asymmetry.

Errors at the anterior neuropore • Corresponds to the opening of the embryonic neural tube in the anterior portion of prosencephalon. • Foramen cecum forms a defect in the anterior skull base. • Closed by its fusion with fonticulus frontalis. • As the foramen closes, diverticulum of dura detaches. • Faulty closure – persistence of neural tissue in the nasal cavity.

Encephaloceles • Extracranial herniations of cranial contents through a defect in the skull. • Meningocele – meninges only • Meningoencephalocele – both brain and meninges • 3 types: occipital sincipital basal

Sincipital encephaloceles Type Course Clinical features Nasofrontal Through bone defect between orbits and forward between nasal and frontal bones to the area superficial to the nasal bones • Glabellar mass • Telecanthus • Inferior displacement of nasal bones. Naso ethmoidal Through foramen cecum deep to the nasal bones turning superficially at the cephalic end of the upper lateral cartilage. • Mass on the nasal dorsum • Superior displacement of nasal bones • Inferior displacement of alar cartilages. Naso orbital Through the foramen cecum deep to the • Orbital mass nasal and frontal bones through a • Proptosis lateral defect in the medial orbital wall • Visual changes

Basal encephaloceles Type Course Clinical features Transethmoidal Through the cribriform plate into the superior meatus • • Nasal obstruction Hypertelorism Broad nasal vault Unilateral nasal mass Spheno ethmoidal Passes through a bony defect between the posterior ethmoid cells and sphenoid. • • Nasal obstruction Hypertelorism Broad nasal vault Unilateral nasal mass

Type Course Clinical features Trans sphenoidal Through a patent craniopharyngeal canal into the nasopharynx • Nasopharyngeal mass • Nasal obstruction • Associated with cleft palate Spheno orbital Through the superior orbital fissure and out of the inferior orbital fissure into the sphenopalatine fossa. • Unilateral exopthalmos • Visual changes

• Soft, cystic, bluish, compressible and translucent mass • Positive Furstenberg test. • Investigation – HRCT with contrast enhanced axial and coronal images. MRI to identify intracranial connection.

Management • Early surgical intervention • Aim – complete resection of lesion and closure of the defect. • Small lesions – managed endoscopically. • Large lesions – craniotomy to resect the lesion and endonasal removal of residual nasal tumour. • Skull base defect – reconstructed using pericranial flap

Complications • CSF leak • Meningitis • Hydrocephalus • Recurrence rate is 4 -10%

Glioma • Heterotopic glial tissue that lacks a patent CSF communication to the subarachnoid space. • Common in males (3: 2 ) • Manifest as – extranasal (60%) - intranasal (30%) - combined (10%)

• Extranasal – smooth, firm, non-compressible, occur along the side of the nose, glabella or nasomaxillary suture line. • Intranasal - pale mass within the nasal cavity with protrusion from the nostril and nasal obstruction. • Arises from the lateral nasal wall near the middle turbinate. • Do not change in size with crying or straining and do not transilluminate.

Investigation • CT scan to assess the bony anatomy of skull base. • MRI – soft tissue connection to brain. • Nasal endoscopy – to assess the location, extent and origin.

Management • Early surgical intervention • Extranasal – lateral rhinotomy, external rhinoplasty. • Intranasal – removed endoscopically

Nasal dermoids • Frontonasal inclusion cysts/tracts. • Most common congenital midline mass. Associated with following congenital anomalies: • Aural atresia • Pinna deformity • Mental retardation • Hydrocephalus • Branchial arch anomalies • Cleft lip and palate • Hypertelorism • Hemifacial microsomia

Clinical features • Manifests as midline pit or mass • Widened nasal bridge • Dimple at the rhinion • Mass lesions are firm, lobulated and noncompressible. • Sinus opening with intermittent caseous discharge • Occasionally, protruding hair present. • Do not enlarge with crying or straining. • Do not transilluminate.
. • MRI – contrast enhanced –")
Imaging • CT scans with contrast (3 mm). • MRI – contrast enhanced – distinguishes the nonenhancing dermoid from enhancing lesions such as hemangiomas and teratomas.

Management • Complete surgical removal. • Extracranial approach should fulfill following criteria: - Excellent access to midline - Access to the base of skull - Adequate exposure for reconstruction of the nasal dorsum - Acceptable scar.

• External rhinoplasty incision – widely used approach. • Gives access to the skull base and allows exposure of nasal dorsum • Lateral rhinotomy and midline vertical incision. • Lesions extending into the cranial cavity – frontal craniotomy.

Midface developmental errors • For normal development of nose and paranasal sinuses the following should take place: - Development of nasal pits and their development into choanae - Fusion of palatal shelves - Growth of nasal septum and soft palate - Development of lateral nasal wall and primitive sinuses.

Arhinia • Congenital absence of external nose, nasal cavities and olfactory apparatus. • Associated with anomalies of ocular and CNS. • Nasal placode fails to canalize and form nasal passages.

Clinical presentation • Ranges from hyporhinia to arhinia. • At birth, only depresion present between the eyes. • Respiratory distress and cyanosis while feeding. • Underdeveloped maxilla and high arched palate. • Hypertelorism • Hypernasal speech

Management • Nutrition – gastrostomy tube • Prosthetic nose • Vertical distraction osteogenesis represents a modality for elongation of the mid face. • Re-establishing the nasal passageway – removing the incisors, creating an airway through the maxilla and releasing the high arched palate.

Polyrhinia and Supernumerary nostril • Double nose with accessory nostril. • Associated with pseudohypertelorism.

• Due to incomplete development of frontonasal process. • Medial nasal processes and septum are duplicated. • Anterior septal duplication with duplicated nasal passageways and postnasal defects like choanal atresia.

Management • Correction of choanal atresia • Medial portions of each nasal passage is removed and lateral portions are anastomosed. • Gives rise to a broad flat nose with a depression in the midline.

Proboscis Lateralis • Congenital tubular nose. • External nose fails to develop on one side. • Tubular structure emanating from the medial canthus. • Fusion of maxillary process with the contralateral nasal process.

• Characterized by absence of nasal cavity and PNS on one side. • Nasolacrimal duct ends blindly. • Associated with microphthalmus, coloboma and arachnoid cysts. • Rerouting of nasolacrimal duct and excision of tubular deformity


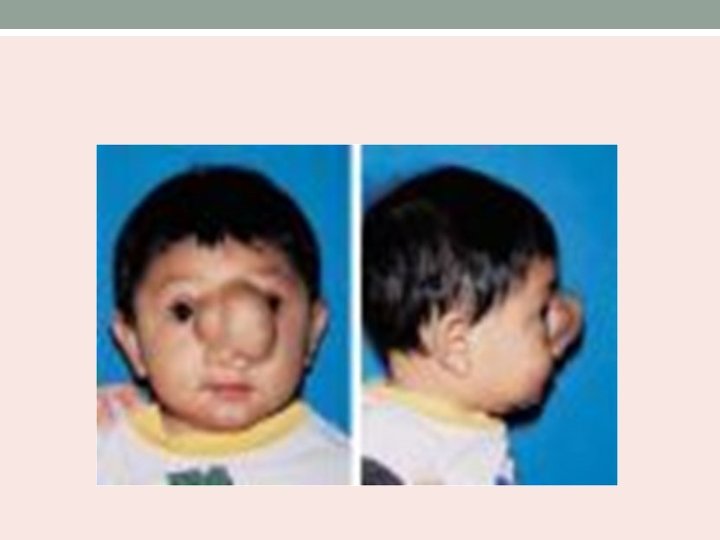
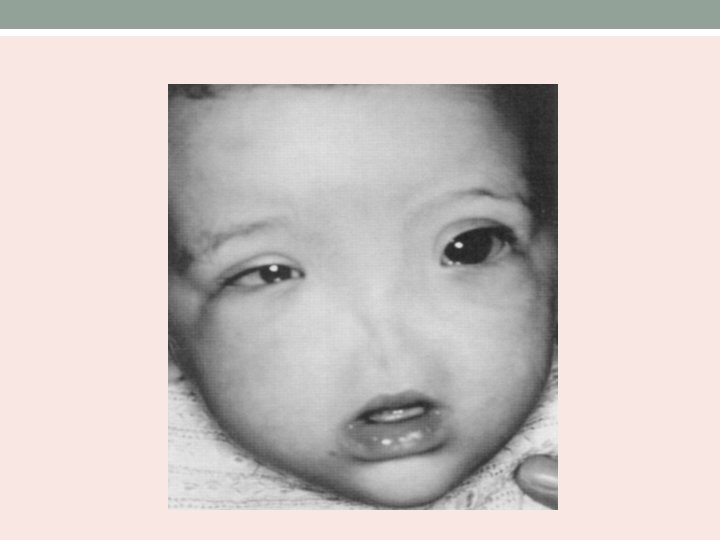
Craniofacial clefts • Ocular hypertelorism • Broad nasal root • Lack of formation of nasal tip • Anterior cranium bifidum occultum • Median clefting of nose, lip and palate. • Unilateral orbital clefting

Cleft lip nasal deformity • Complete cleft lip extends upto the floor of the nose. • Incomplete cleft lip extend only partway through the upper lip. • Children with bilateral cleft lip have flattened nasal tip and a shortened columella. • Associated maxillary hypoplasia with prognathism.

Congenital nasal pyriform aperture stenosis • Occurs secondary to bony overgrowth of the nasal process of maxilla. • Pyriform aperture – narrowest part of nasal cavity. • Small changes in this area affect by increasing nasal airway resistance.

May be associated with presence of central mega incisor and holoprocencephaly.

• CT scan of nose and PNS – cross sectional area of pyriform aperture, nasal cavity and choana reduced. • Distance between the medial aspects of the maxillae at the level of inferior meatus – 12 mm. • Management : Nasal tubes and topical vasoconstrictive drops. • Sublabial approach exposing the lateral pyriform aperture.


Nasolacrimal duct cysts • Dacrocystoceles. • U/L or B/L • If no lumen at both ends of NLD system – fluid built up – cyst formation. • Nasal obstruction, respiratory distress and epiphora. • Aspiration and feeding difficulties. • Diagnosis – anterior rhinoscopy or nasal endoscopy – cystic mass in the inferior meatus. • CT scan- dilated nasal lacrimal duct, an intranasal cyst and cystic dilatation of sac.

Management • Cyst is marsupalized endoscopically into the inferior meatus. • Lesion is opened with curette or microsurgical debrider.

Developmental errors of the nasobuccal membrane • Failure of the bucconasal membrane to rupture between the 5 th and 6 th week of development results in choanal atresia. • U/l or b/l obstruction of posterior choanae. • Postnasal space fails to communicate with nasopharynx. • In bilateral choanal atresia, child is in acute respiratory distress which improves when the child starts crying. • Bilateral choanal atresia – airway emergency.

Other anomolies associated with choanal atresia CHARGE syndrome • Coloboma • Heart defects • Atretic choana • Retardation of growth and development • Genitourinary disorders • Ear abnormalities

Anatomic features • Narrow nasal cavity • Lateral bony obstruction by the pterygoid plates • Medial obstruction caused by thickened vomer • Bony or membranous.

Diagnosis • Failure to pass a 8 F catheter through the nose into the nasopharynx. • Endoscopic examination

Absence of fogging

Investigations • Rhinography - administration of radiopaque dye into the nasal cavity. • CT scan -Confirm the diagnosis of choanal atresia (unilateral or bilateral). -Evaluate choanal atresia (vomer bone width). -Exclude other possible nasal sites of obstruction. -Determine the degree of bony, membranous, or mixed atresia. -Other abnormalities in the nasal cavity and nasopharynx.

Choanal atresia: Rhinogram demonstrating blockage of radiopaque dye at the posterior choanae.
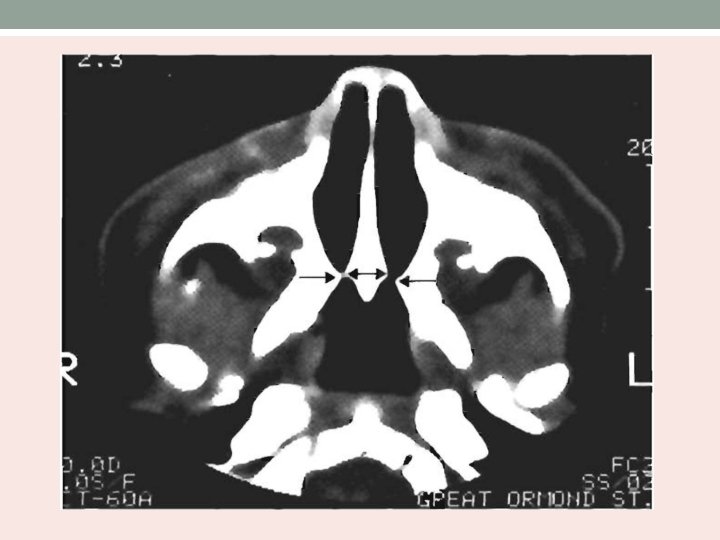

Investigations • Axial view of CT scan nose/paranasal sinus showing bony choanal atresia • CT scan – thickness of atresia

Management • Oropharyngeal or orotracheal airway and gastric feeding • Mcgovern’s nipple • Tracheostommy Definitive • Transnasal approach • Transpalatal approach

ENDOSCOPIC TRANSNASAL APPROACH

TRANSPALATAL APPROACH • An incision is made around summit of the alveolar ridge or at the gingivopalatal margin if teeth are present. • The mucous membrane of hard palate is elevated, using Cottle septal elevator. • Flap is developed posteriorly, until edge of hard palate is reached.

• The nasopharynx is entered. • Using cutting burs of suitable size, the posterior end of the hard palate removed to expose the bony atresia. • Continuity of the nasal cavity restored by drilling away the obstructing bone, the posterior end of the vomer being removed at the same time. • Bilateral nasal stent placed.

Maxillary hypoplasia • Underdevelopment of the maxillary sinus. • Categories are : - Isolated hypoplasia - Regional developmental anomalies – facial dystosis • Developmental abnormality of the uncinate process – helps in aeration.

Bolger’s MSH Classification • Based on the degree of pneumatization and lateral nasal wall abnormalities. Type Uncinate process MSH I normal mild II Absent severe III Absent Cleft-like

Bilateral type I MSH well developed infundibular passage with mild MSH

Type II MSH, hypoplastic uncinate process and pathologic infundibular passage with significant MSH.

Type III MSH, slit-like maxillary sinus.

THANK YOU
- Slides: 71