Outcomes At the end of the lecture you


: -This is a small")


 The foregut lies caudal")






























- Slides: 62
Outcomes: At the end of the lecture you should be able to: • Describe the process of formation of the three parts of the gut and list their final derivatives. • Describe the development of the stomach and intestine. • Explain the common congenital anomalies of the gut (congenital umbilical hernia, oesophageal stenosis, congenital hypertrophic pyloric stenosis, atresia and stenosis of intestine, intestinal diverticula and persistence of vitellointestinal duct)
YOLK SAC 1. Primary yolk sac (it is the earliest): -This is a small cavity - Its roof is formed by the primary endoderm. 2. Secondary yolk sac: The primary yolk sac is converted into the secondary yolk sac - It is completely lined with endoderm. Endoderm
YOLK SAC After folding 3. Definitive yolk sac: It is the last stage and is formed after folding. As a result of folding a part of the yolk sac is enclosed within the embryo to from the gut. - The part inside the head fold is called Foregut The part inside the tail fold is called hind gut. - The part between the two lateral folds is called midgut. The part of the yolk sac which remains outside the embryo is called definitive yolk sac. * The definitive yolk sac is connected to the midgut by the vitello-intestinal duct.
Oral membrane Amniotic cavity Foregut Midgut Hindgut Gut Cloacal membrane Before folding Stomodeum Yolk sac Vitellointestinal duct FOLDING Allantois Cloacal membran e stalk Connecting After folding It is the process of transformation of the early disc-shaped structure into an embryo acquire a definite shape. It starts at the end of the 3 rd week. The embryo folded upon itself ventrally forming a head fold at the cephalic end, a tail fold at the caudal end and right and left lateral folds at the sides.
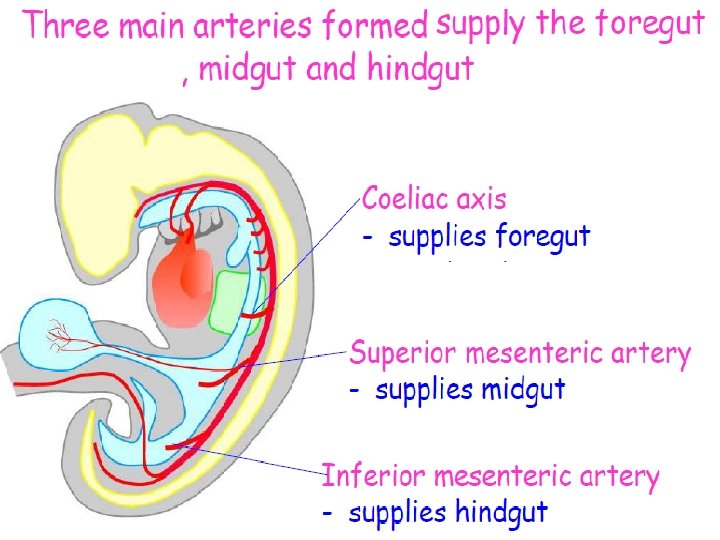
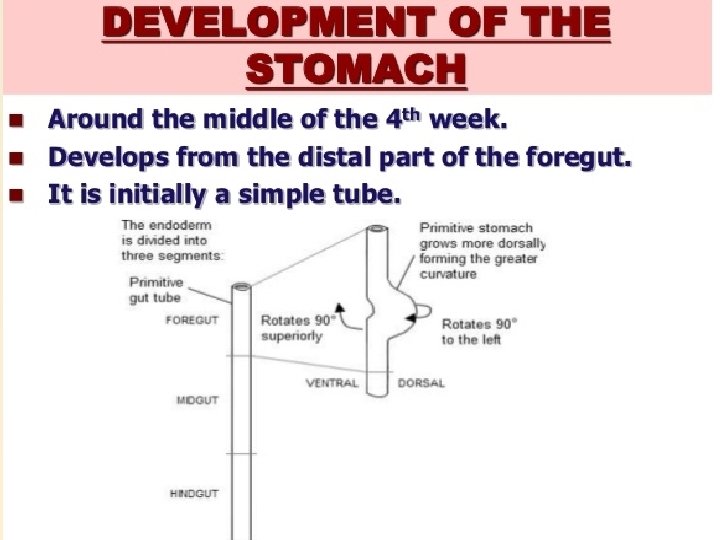
Development of the primitive gut and its derivatives has: (a) The foregut lies caudal to the pharyngeal tube and extends as far caudally as the liver outgrowth. (b) The midgut begins caudal to the liver bud and extends to the junction of the right two-thirds and left third of the transverse colon in the adult. (c) The hindgut extends from the left third of the transverse colon to the cloacal membrane
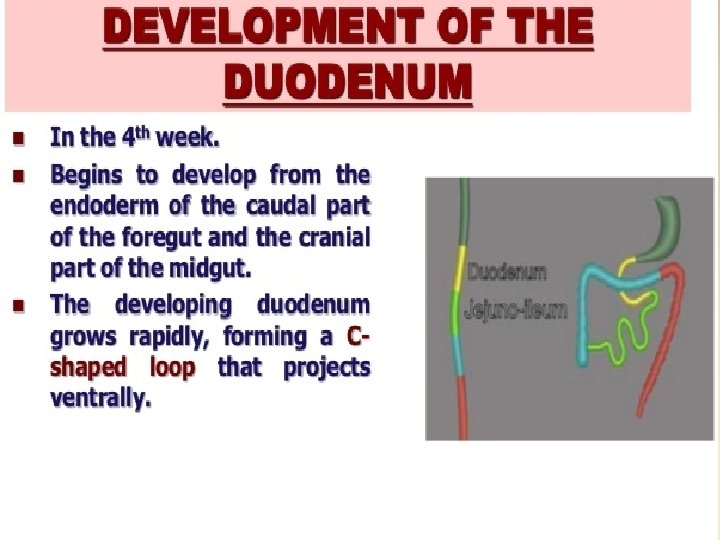
A-Foregut
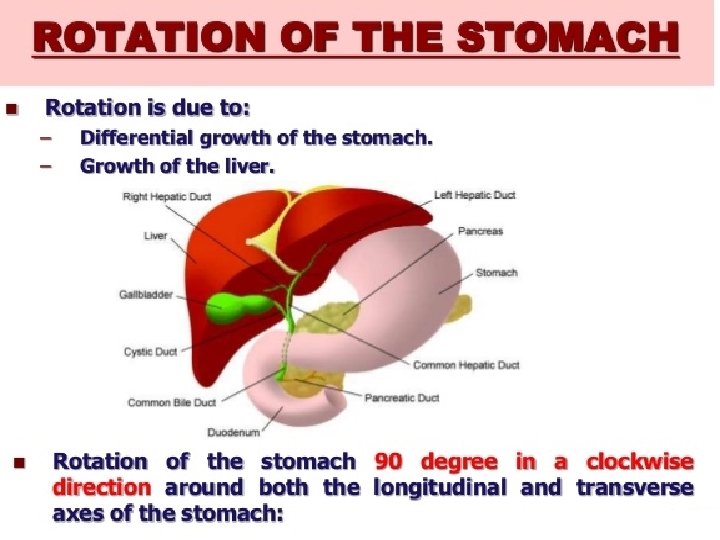
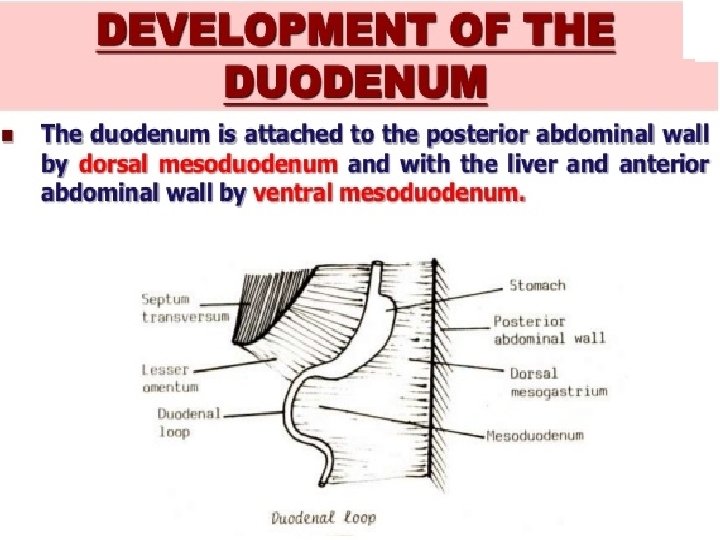
Since the stomach is attached to the ventral body wall by the ventral mesogastrium and to the dorsal body wall by the dorsal mesogastrium , its rotation pulls the dorsal mesogastrium to the left, creating a space behind the stomach called the lesser sac This rotation also pulls the ventral mesogastrium to the right.
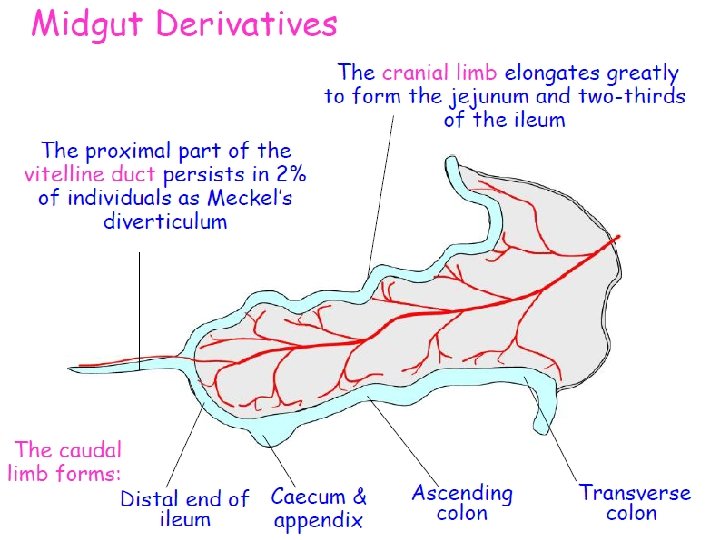
B-Midgut at 5 weeks consists of a simple loop communicates with the yolk sac through the vitelline duct swelling in the caudal limb marks the future caecum supplied by the superior mesenteric artery suspended by dorsal mesentery
Midgut Herniation At 6 weeks the midgutloop elongates rapidly and the liver enlarges. The abdominal cavity becomes relatively small and part of the intestine herniates into the extra-embryonic coelom, through the coelomic opening next to the umbilical cord. Midgut Retraction During the 10 thweek the abdomen enlarges and the intestine returns into the abdominal cavity. As this occurs, the midgut loop rotates so that the different parts of the intestine acquire their definitve positions in the abdominal cavity. Midgut Retraction
Ø Umbilical herniation occurs because there is not enough room in the abdomen for the rapidly growing midgut Ø The shortage of space is caused mainly by the relatively massive liver and two sets of kidneys during this stage of development Ø The midgut loop has a cranial limb and a caudal limb Ø Yolk stalk is attached to the apex of the midgut loop where the two limbs join ØThe cranial limb grows rapidly and forms small intestinal loops ØThe caudal limb undergoes very little change except for development of cecal diverticulum which is a primordium of the cecum and appendix
Rotation of Midgut Loop Ø While it is in the umbilical cord the midgut loop rotates 90º counterclockwise around the axis of superior mesenteric artery Ø This brings cranial limb to the right and the caudal limb to the left Ø During rotation the midgut elongates and forms intestinal loops e. g. Jejunum and ileum
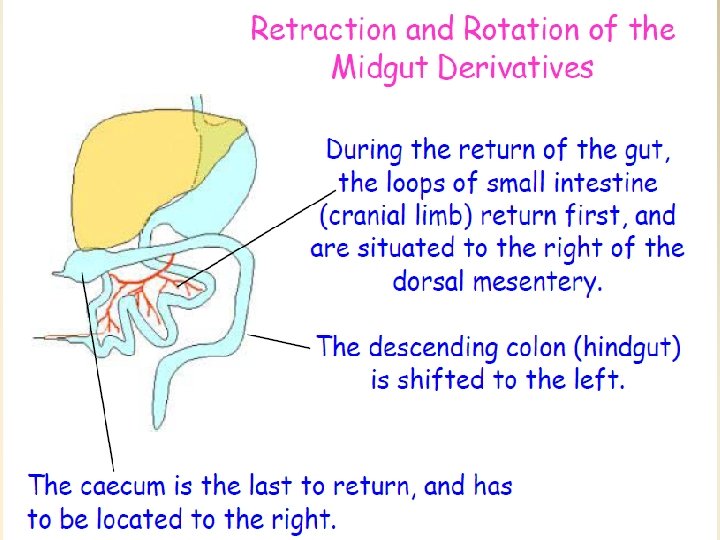
Return of Midgut Loop to Abdomen Ø During the 10 th week the intestines return to the abdomen Ø What causes the return of the intestine is not known Ø The decrease in the size of the liver and kidneys and the enlargement of the abdominal cavity are important factors Ø This process is called reduction of the physiological midgut hernia
Return of Midgut Loop to Abdomen Ø The small intestine formed from cranial limb returns first Ø It passes posterior to the superior mesenteric artery and occupies the central part of the abdomen Ø As the large intestine returns, it undergoes further 180º counterclockwise rotation Ø Later it comes to occupy the right side of the abdomen
Cecum and Appendix Ø The primordium of cecum and appendix, the cecal diverticulum appears in the 6 th week as a swelling on the antimesenteric border of the caudal limb of the midgut Ø The apex of the cecal diverticulum does not grow as rapidly as the rest of it Ø The appendix is initially a small diverticulum of cecum
C-Hindgut The hindgut gives rise to the distal third of the transverse colon, the descending colon, the sigmoid, the rectum, and the upper part of the anal canal. The endoderm of the hindgut also forms the internal lining of the bladder and urethra The terminal portion of the hindgut enters into the posterior region of the cloaca, the primitive anorectal canal; .
Cecum and Appendix Ø The appendix increases rapidly in length so that at birth it is a relatively long tube arising from the distal end of the cecum Ø After birth the wall of the cecum grows unequally with the result that appendix comes to enter the medial side Ø Appendix is considerably variant in position, retrocecal, retrocolic and pelvic appendix
Hindgut The derivatives of the hindgut are: The left one-half of the transverse colon Ø Descending and sigmoid colons Ø Rectum and the superior part of the anal Ø canal The epithelium of the urinary bladder and Ø most of the urethra
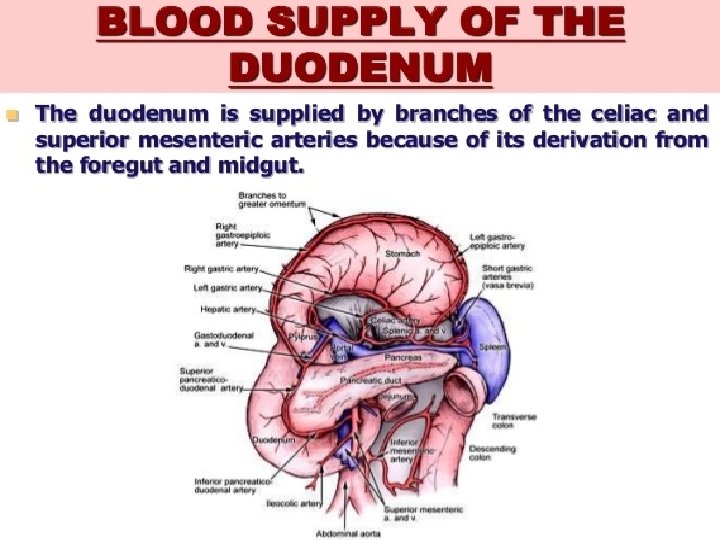
Hindgut All hindgut derivatives are supplied by the Ø inferior mesenteric artery The junction between the segment of Ø transverse colon derived from the midgut and that originated from the hindgut is indicated by the change in blood supply Superior mesenteric artery is the midgut Ø artery Inferior mesenteric artery is the hindgut Ø artery
Hindgut The descending colon becomes Ø retroperitoneal as its mesentery fuses with the peritoneum on the left posterior abdominal wall and then disappears The mesentery of the sigmoid colon Ø is retained but it is shorter than in the embryo
Cloaca This terminal part of the hindgut is Ø an endoderm-lined chamber that is in contact with the surface ectoderm at the cloacal membrane This membrane is composed of Ø endoderm of the cloaca and ectoderm of the proctodeum or anal pit
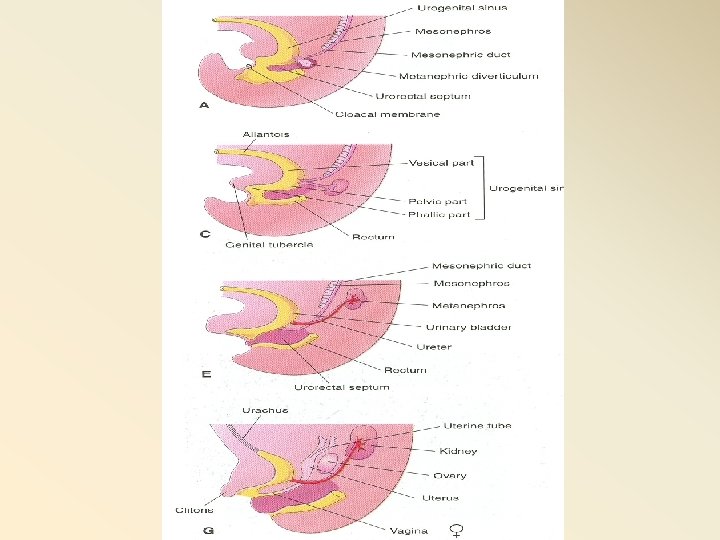
Partitioning of Cloaca The cloaca is divided into dorsal and Ø ventral parts by a wedge of mesenchyme, the urorectal septum It develops in the angle between the Ø allantois and hindgut As the septum grows toward the cloacal Ø membrane , it develops forklike extensions that produce infoldings of the lateral walls of the cloaca
Partitioning of Cloaca These folds grow toward each other Ø and fuse to form a partition that divides the cloaca into two parts The rectum and cranial part of the Ø anal canal dorsally The urogenital sinus ventrally Ø
appears at about 16 days as a small diverticulum projecting from the caudal end of the yolk sac into the connecting stalk The urorectal septum separates the hindgut from the allantois. It grows towards the cloacal membrane. It is derived from mesoderm at the junction between the connecting stalk and yolk sac.
The terminal portion of the hindgut enters into the posterior region of the cloaca, the primitive anorectal canal; the allantois enters into the anterior portion, the primitive urogenital sinus. The urorectal septum, separates the region between the allantois and hindgut.
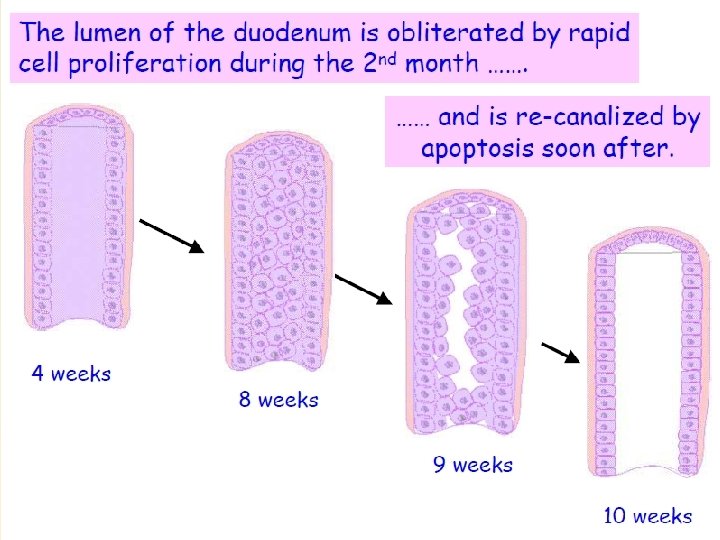
The Anal Canal • At the end of the 8 thweek, after rupture of the cloacal membrane, proliferation of ectoderm occludes the anal opening. • During the 9 thweek the opening is recanalized. • Thus the terminal part of the anal canal is ectodermal in origin and supplied by the inferior rectal artery. • The junction between ectoderm and endoderm is the pectinate line.
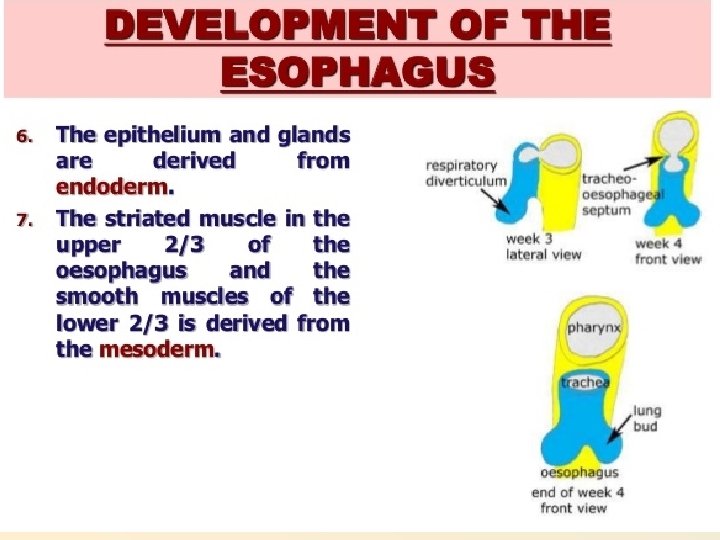
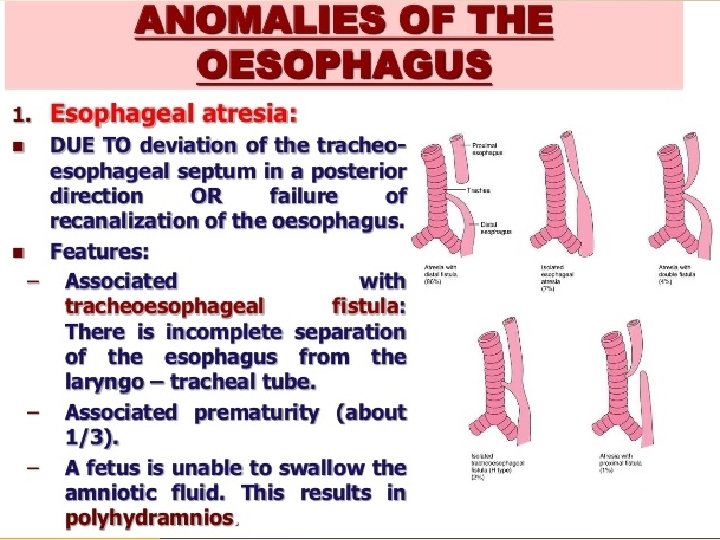
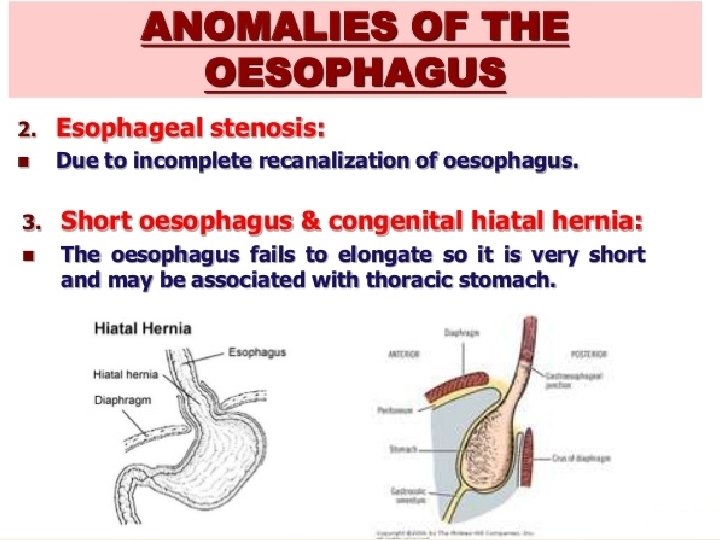
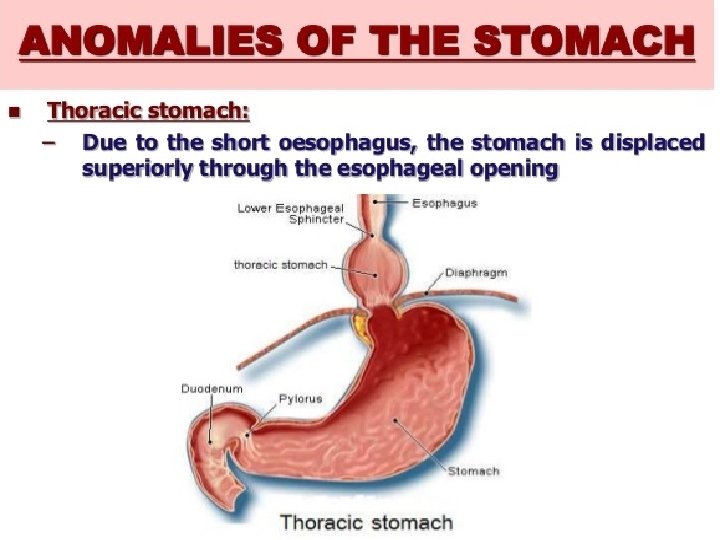
CLINICALCORRELATES Esophageal Abnormalities Esophageal atresia and/or tracheoesophageal fistula results either from spontaneous posterior deviation of the tracheoesophageal septum esophageal stenosis, . Stenosis may be caused by incomplete recanalization,
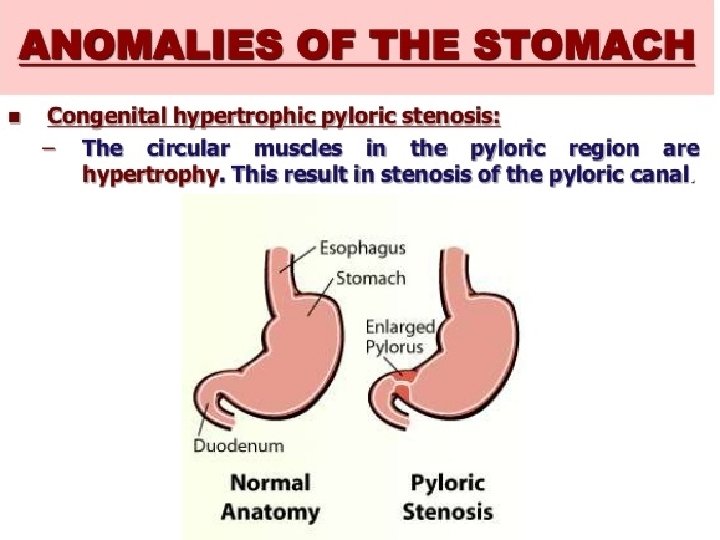
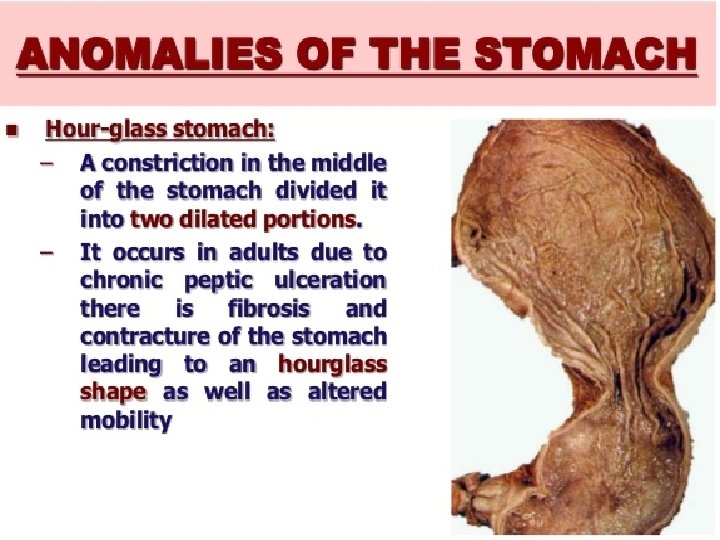
Stomach Abnormalities Hypertrophic Pyloric Stenosis Pyloric stenosis is characterized by hypertrophy of the pyloric musculature, leading to a mechanical obstruction of the gastric outlet in the affected infant. Thus, hypertrophied pyloric antral muscle fibres protrude distally into the duodenal lumen, producing a reflection of duodenal mucosa. Infants with pyloric stenosis usually present with a gradual onset of worsening nonbilious vomiting, beginning between 3 to 6 weeks of age. The pattern of vomiting can vary, but often it progresses to the characteristic “projectile” vomiting.
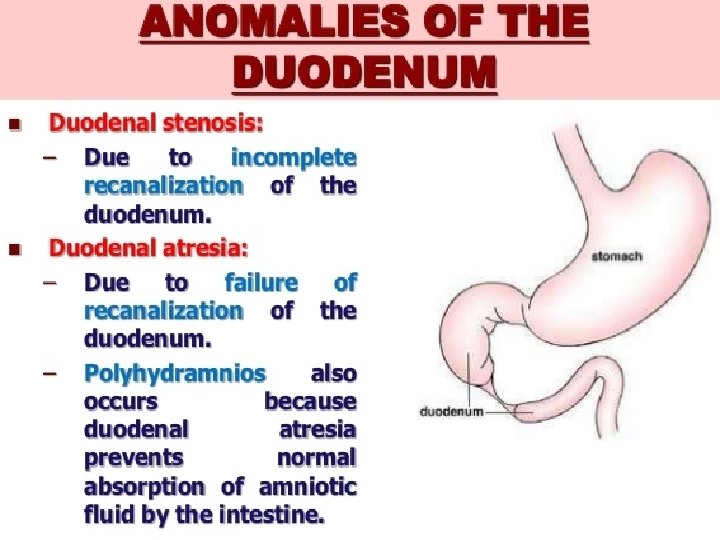
Intestinal Atresia and Stenosis Duodenal Atresia and Stenosis Most cases of duodenal atresia result from incomplete recanalizationof the lumen distal to the duodenal papilla. Clinical Features: • repeated bile-stained vomiting on first day postnatal • double bubble in stomach and bubble in dilated part of the duodenum separated by the air-free pyloric canal. • no intestinal gas shadows • relieved by resection of obstructed segment. About 25% of cases are associated with Down syndrome
Atresia of the Jejunum, Ileum and Colon • Atresias of the small intestine and colon are rare • most cases are segmental rather than localized. ie. they involve a long segment of the jejunum or ileum • some cases involve a large segment of the midgutloop derivatives –termed “apple peel” atresiabecause a short segment of intestine distal to the atresia is coiled around the superior mesenteric artery remnant. Atresiasof the jejunum, ileum or colon, unlike duodenal atresia, result fromarterial occlusionrather than failure of recanalization Most cases present as intestinal obstruction a few days after birth
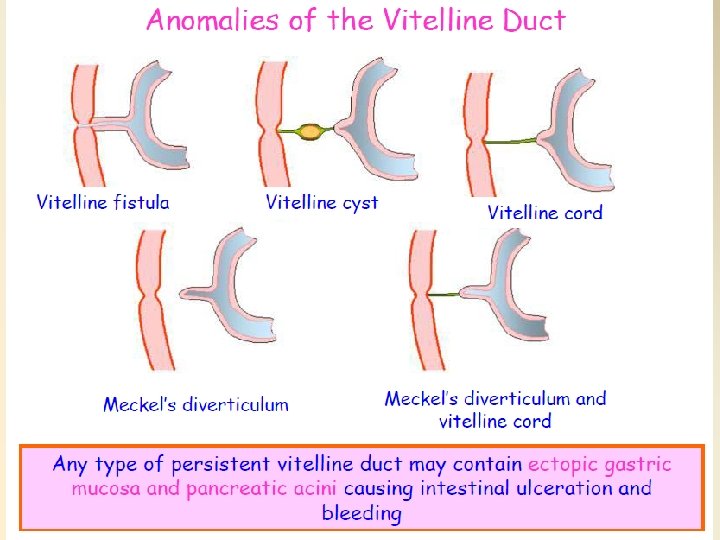
Vitelline Duct Abnormalities Meckel’s diverticulum or ileal diverticulum In the adult, this diverticulum, approximately 40 to 60 cm from the ileocecal valve on the antimesenteric border of the ileum, enterocystoma, or vitelline cyst. Since the fibrous cords traverse the peritoneal cavity, intestinal loops may twist around the fibrous strands and become obstructed, causing strangulation or volvulus. In another variation the vitelline duct remains patent over its entire length, forming a direct communication between the umbilicus and the intestinal tract. Umbilical fistula, or vitelline fistula. A fecal discharge may then be found at the umbilicus.
Gut Rotation Defects Abnormal rotation of the intestinal loop Volvulus is a rotation of an intestinal loop around a branch of the superior mesenteric artery -it may cause intestinal obstruction or even gangrene –some cases correct spontaneously but surgical intervention is usually performed Intussusception is the invagination of a segment of intestine in itself, causing obstruction
Reversed rotation of the intestinal loop occurs when the primary loop rotates 90◦ clockwise. Duplications of intestinal loops and cysts may occur anywhere along the length of the gut tube.
Hindgut Abnormalities • Rectoanal atresias, and fistulas, • Imperforate anus, there is no anal opening. This defect occurs because of a lack of recanalization of the lower portion of the anal canal • Urorectal fistula
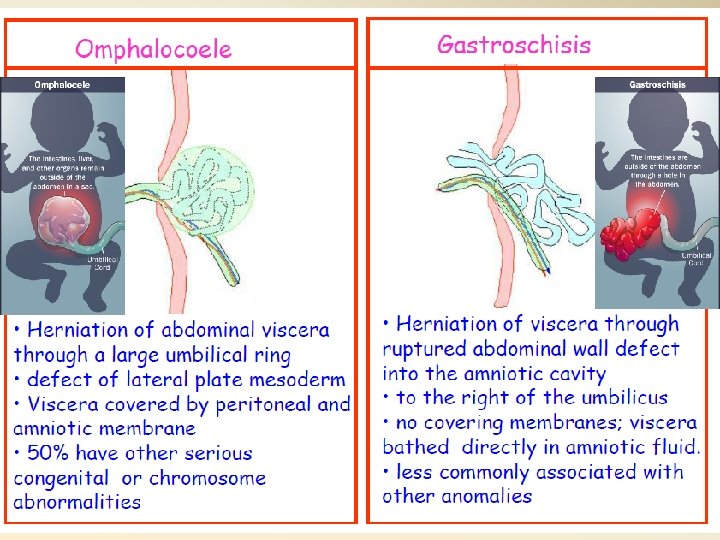
Gastroschisis is a herniation of abdominal contents through the body wall directly into the amniotic cavity.
Body Wall Defects Omphalocele : herniation of abdominal viscera through an enlarged umbilical ring.