UPDATE IN URINALYSIS Diane Gaspari SHASCP Division Manager
 Division Manager, Core Lab York Hospital, York, PA")








 – Puffiness around the eyes, especially in")









 urine samples")
 • In most cases, screening with urine dipsticks is acceptable")
 • Patients with a positive dipstick (1+ or greater): confirm")
 • Monitoring proteinuria in patients with CKD should be performed")
 • Children Without Diabetes: – Screen spot urine sample for")
 • Children With Diabetes: – Screening and monitoring of post-pubertal")





 • Diabetes and Chronic Kidney Disease –")
 • Diagnosis codes")












 – Reduced recovery rate of")














 Fluorescence High (FLH) Fluorescence Low")

 Large Fsc Small -")












 Enhanced detection of bacteria Dye Dye Forward Scatter 2) Staining")
















 • • • X’TAL: YLC: SRC: Path. CAST: MUCUS:")









 • ~15% volume increase since 2001")


- Slides: 111
UPDATE IN URINALYSIS Diane Gaspari, SH(ASCP) Division Manager, Core Lab York Hospital, York, PA ggaspari@wellspan. org
Program Objectives • Enhance knowledge of CKD and the NKF’s guidelines for laboratory diagnosis & monitoring of CKD. • Identify pre-analytic variables of urinalysis testing & analytic variables of manual urine sediment testing. • Understand the technology, software features, and flagging parameters of the Sysmex UF -1000 i automated urine sediment analyzer. • Identify the benefits of automated urine sediment analysis.
Did You Know. . . “Urinalysis is the most valuable single test of the anatomic integrity of the kidneys that is readily available to the clinician” Schreiner From J. Szwed, The Importance of Microscopic Examination of the Urinary Sediment, American Journal of Medical Technology, 48: 2, Feb. 1982
Functions of Kidney • Remove waste products & drugs from body. • Balance body’s fluid, release hormones to regulate blood pressure, and produce active vitamin D. • Regulation of body’s salt, potassium, & acid content
National Kidney Foundation • http: //www. kidney. org/kls/index/cfm • http: //www. kidney. org/professionals/kdo qi/guidelines • New Guidelines February 2002 • Addition to Guidelines in 2003, 2005, 2006, 2007, 2008, and 2012.
Incidence and Prevalence of End-Stage Renal Disease in the U. S.
CHRONIC KIDNEY DISEASE • CKD is a world-wide public health problem that is under-diagnosed and under-treated. • Early diagnosis is critical as kidney disease is often silent in the early stages. • Most common causes of CKD in North America is diabetes, hypertension, and glomerular disease.
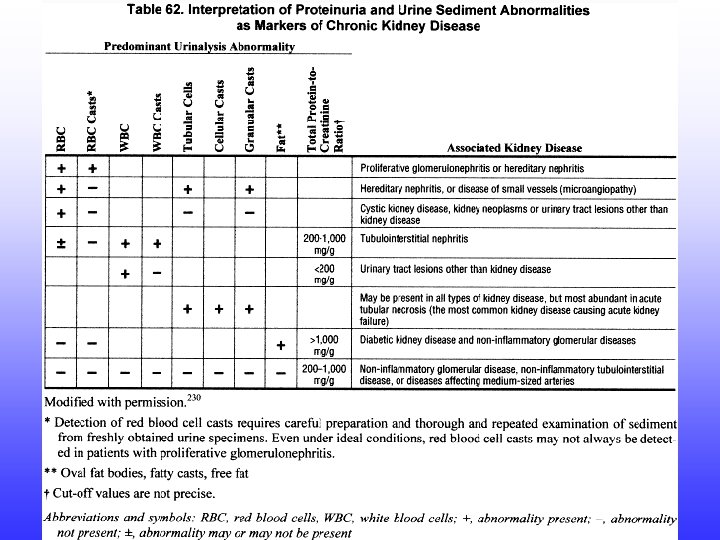
CHRONIC KIDNEY DISEASE • Presence of excessive amounts of urine protein is most common clinical sign of early kidney dysfunction. • Other markers of kidney damage – abnormal urine sediment – abnormal findings on imaging studies – abnormal blood & urine chemistry results that identify renal tubular syndromes
CHRONIC KIDNEY DISEASE • Symptoms – fatigue – difficulty concentrating – poor appetite – sleeplessness – muscle cramping at night – swollen feet and ankles
CHRONIC KIDNEY DISEASE • Symptoms (cont. ) – Puffiness around the eyes, especially in the morning – Dry, itchy skin – Frequent urination, especially at night
Complications of CKD • Result of reduction of GFR, disorder of tubular function, or reduction in endocrine function of the kidney – Hypertension – Malnutrition – Anemia – Low serum albumin and serum calcium
Complications of CKD – High serum phosphate concentration and high serum parathyroid hormone concentration – Reduced activities of daily living – Lower quality of life – Increased risk of cardiovascular disease and stroke
Laboratory Diagnosis and Monitoring of CKD • Definitive diagnosis of the type of kidney disease is based on biopsy or imaging studies – Biopsy and invasive imaging procedures are associated with a risk or serious complications and are usually avoided unless a definitive diagnosis would change treatment or prognosis
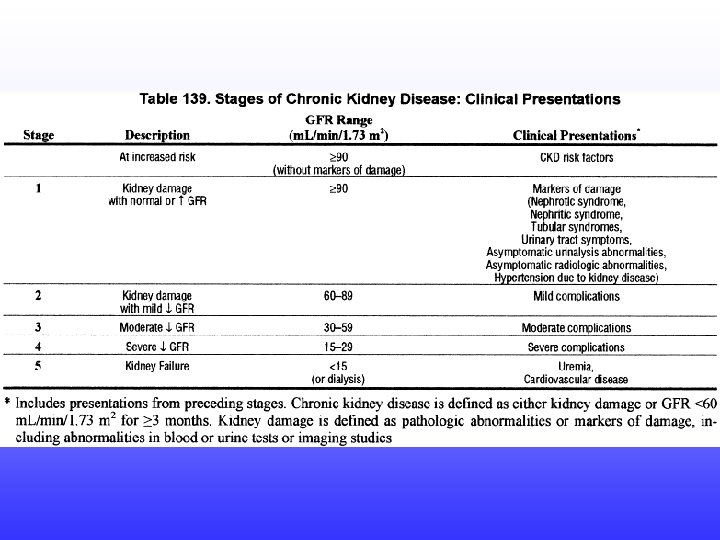
Laboratory Diagnosis and Monitoring of CKD • GFR is the best overall index of kidney function – Decreased GFR precedes the onset of kidney failure and persistently reduced GFR is a specific indicator of CKD. – Drug dosing in CKD is based on GFR levels
Laboratory Diagnosis and Monitoring of CKD • GFR cannot be measured directly – Serum creatinine is used to measure GFR in most cases • Use of an international standard or traceable standard for creatinine calibration is recommended. • Creatinine clearance is considered too inaccurate due to difficulties in obtaining a correctly timed specimen.
Laboratory Diagnosis and Monitoring of CKD • The NKF guidelines recommend that clinical labs report an estimate of GFR using the MDRD prediction equation in addition to the serum creatinine. • Variables that will affect the estimation of GFR include: age, sex, race, diet, body build, medication, and pregnancy. • If the variables are significant, use the creatinine clearance.
Laboratory Diagnosis and Monitoring of CKD • Serum creatinine is recommended at least yearly in patients with CKD. • The rate of decline in GFR can be used to estimate the interval until onset of kidney failure and facilitate planning for therapy, diet, or kidney replacement. • An acute decline in GFR may be superimposed on CKD and result in acute deterioration of kidney function.
Laboratory Diagnosis and Monitoring of CKD • Most common causes of deterioration of kidney function are: – Reduced blood flow to the kidney, usually related to volume depletion. – Toxic insult – Obstruction from tumors, stones, or blood. – Inflammation and infection
Cystatin C • 13 k. Da cysteine protease inhibitor constantly produced by all nucleated cells • Advantages over creatinine – Constant rate of production, freely filtered by the glomerulus – Unaffected by muscle mass, diet or gender – No renal tubular secretion – Good assay precision (~3% CV throughout assay range) – Assay unaffected by spectral interferences
NKF Guidelines for Adults and Children • Under most circumstances, untimed (“spot”) urine samples should be used to detect and monitor proteinuria. • First morning urines preferred but random specimens are acceptable. Timed urine collection (overnight or 24 hr) is not necessary.
NKF Guidelines (cont. ) • In most cases, screening with urine dipsticks is acceptable for detecting proteinuria – Standard urine dipsticks are acceptable for detecting increased total urine protein. – Albumin-specific dipsticks are acceptable for detecting albuminuria
NKF Guidelines (cont. ) • Patients with a positive dipstick (1+ or greater): confirm proteinuria by a quantitative measurement (protein-tocreatinine ratio >200 mg/g or albumin-tocreatinine ratio >30 mg/g) within 3 mos. • Patients with 2 or more positive quantitative tests temporally spaced by 1 -2 weeks: diagnosed as persistent proteinuria; further evaluation needed
NKF Guidelines (cont. ) • Monitoring proteinuria in patients with CKD should be performed using quantitative measurements. • Children Without Diabetes: – orthostatic proteinuria must be excluded by repeat measurement on a first morning specimen if the initial proteinuria was obtained on a random specimen.
NKF Guidelines (cont. ) • Children Without Diabetes: – Screen spot urine sample for total urine protein using either: standard urine dipstick or total protein-to-creatinine ratio – When monitoring proteinuria for CKD, total protein-to-creatinine ratio should be measured in spot urine specimens.
NKF Guidelines (cont. ) • Children With Diabetes: – Screening and monitoring of post-pubertal children with diabetes of 5+ years duration should follow the adult guidelines. – Screening and monitoring other children with diabetes should follow the guidelines for children without diabetes.
2005 Additions to NKF Guidelines • Bone Metabolism & Disease in Children with Chronic Kidney Disease: 10/05 – Warns that bone disease begins early in the course of CKD in children & calcium balance must be in order for growth & cardiovascular development – Physicians need to place greater emphasis on vitamin D nutrition, levels of parathyroid hormone, & excesses of calcium intake which can lead to development of vascular calcifications.
2005 Additions to NKF Guidelines • Cardiovascular Disease in Dialysis Patients: 4/05 – Warns that CVD is leading cause of death among dialysis patients but treatment is not as effective as in general population – Dialysis patients are more prone to sideeffects of treatment – More research is needed to better manage CVD in dialysis patients
2006 Additions to NKF Guidelines • Treatment of Anemia in Chronic Kidney Disease: 5/06 – Patients with all stages of CKD should be evaluated for anemia – Definition of anemia is <13. 5 g/d. L for males & <12. 0 g/d. L for females – Treat patients with ESA(erythropoiesis stimulating agent) &/or iron when Hgb is <11 g/d. L
2007 Additions to NKF Guidelines • Chronic Kidney Disease and Diabetes: 2/07 – Emphasizes diabetes prevention, screening & management of kidney disease – New term: diabetic kidney disease (DKD)
2012 Additions to NKF Guidelines • Diabetes and Chronic Kidney Disease – Target Hb. A 1 c of ~7. 0% to prevent or delay progression of microvascular complications of diabetes, including DKD. – Lipid-lowering treatment with statins suggested for patients with diabetes and CKD, including kidney transplant recipients
2012 Additions to NKF Guidelines (cont. ) • Diabetes and Chronic Kidney Disease – Withholding statin treatment initiation in dialysis patients is suggested. – Treatment of normotensive patients with diabetes & elevated levels of albuminuria by ACE inhibitors or angiotensin receptor blockers (ARB). – Statin combination therapy reduces risk of CVD events.
International Classification of Diseases, 9 th Revision Clinical Modification (ICD-9 -CM) • Diagnosis codes for CKD to be based on NKF’s KDOQI Guidelines – Codes allow medical professionals to clearly note the stage of kidney disease – Ability to identify CKD patients who are kidney transplant recipients – Ability to link specific treatments to appropriate CKD stage
Legislative Mandate for Labs to Report e. GFR • States with laws requiring reporting of e. GFR – New Jersey, Tennessee, Michigan, Louisiana, Connecticut, and Pennsylvania • PA General Assembly House Bill 2639 – Passed into PA state law in November, 2006 – e. GFR must be calculated for serum creatinine for patients > 18 years – All labs had to comply within 2 years of passage
Facts of Kidney Disease • More than 26 million Americans have CKD. More than 20 million more at increased risk for developing kidney disease and most do not know it. • At the end of 2010, there were 651, 000 Americans receiving treatment for kidney failure (end stage renal disease or ESRD).
Facts of Kidney Disease • Each year, more than 70, 000 Americans die from causes related to kidney failure. • Every month, the number of Americans waiting for kidney transplants increases. Approximately 96, 292 patients are awaiting kidney transplants and >2, 500 are waiting for kidney-pancreas transplants.
Facts of Kidney Disease • Shortage of organ donations is major contributing factor to the growing number of people on the waiting list. A new name is added every 12 minutes and eighteen people die daily while waiting. • CKD has a disproportionate impact on minority populations, especially African Americans, Hispanics, Asians, and American Indians.
Facts of Kidney Disease • Diabetes is the leading cause of kidney failure: 51% of new cases and 45% of all cases of kidney failure in U. S. • Uncontrolled or poorly controlled high blood pressure is the second leading cause of kidney failure in U. S: 28% of new cases and 25% of kidney failure in U. S.
Facts of Kidney Disease • Third & fourth leading causes of kidney failure in U. S. are glomerulonephritis and polycystic kidney disease: 8. 2% and 2. 2% of new cases in U. S. • Kidney and urologic diseases continue to be major causes of work loss, physician visits, and hospitalizations among men and women.
Laboratory’s Involvement With NKF Guidelines • Good creatinine calibration • Add GFR prediction equation to report • Understand limits of urine test strip protein • Add urine test with good low end sensitivity to urine albumin (microalbumin) • Improve urine sediment testing
Preventing Kidney Disease • • Blood glucose & blood pressure checks Regular physician check-ups Taking medications as prescribed by physician Regular exercise; lose weight if overweight; low -fat diet • Avoid tobacco use; moderate alcohol consumption • Cholesterol levels in target range
Siemens Clinitek Microalbumin 2 Reagent Strips • Provide albumin, creatinine, and albumin to creatinine ratio results in 1 minute • Can be used by POC or physicians’ offices • Use with Clinitek 50 or Clinitek Status analyzers – Sensitivity as low as 2 mg/d. L for urine protein – More reliable; less affected by interferences (e. g. specific gravity and p. H)
Siemens Clinitek Microalbumin 9 Reagent Strips • Provide albumin, blood, creatinine, glucose, ketone, leukocyte, nitrite, p. H, & protein and albumin to creatinine ratio & protein to creatinine ratio • Use with Clinitek Status or Advantis analyzers – Random sample; no timed or 24 hr urine sample required – Accurate identification of microalbuminuria
Urinalysis Testing • Pre-analytic variables – Specimen collection: need written or clearcut oral instructions on specimen collection – Type of specimen collection (random, clean catch, cath) – Delay in specimen delivery – Specimen storage conditions
Manual Urine Sediment Analysis • Analytic variables – Mixing of samples by inversion, not swirling – Standardized volume for centrifugation; note volume if less than 12 m. L – Time and G force for centrifugation; do not use brake – Inconsistent decantation and re-suspension steps after centrifugation
Manual Urine Sediment Analysis • Analytical variables (cont. ) – Reduced recovery rate of urine elements after centrifugation – Variability in concentration ratio • • Supernatant removal Mixing of suspension Filling of chamber; technique-dependent Distributional errors
Manual Urine Sediment Analysis • Commercial slide systems – Provide some standardization – Technique-dependent – Vary in concentration ratios: 1: 5 to 1: 48 – Addition of drop of stain also varies concentration ratio – Low & high power fields of view are microscope dependent; reporting unit inequity
Manual Urine Sediment Microscopy • • Subjective element identification Poor reproducibility Lack of standardization Time consuming/labor intensive
Sysmex UF-1000 i
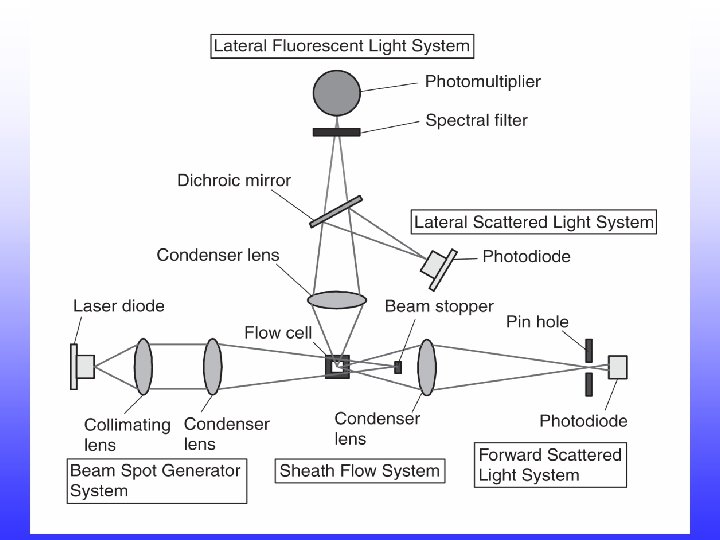
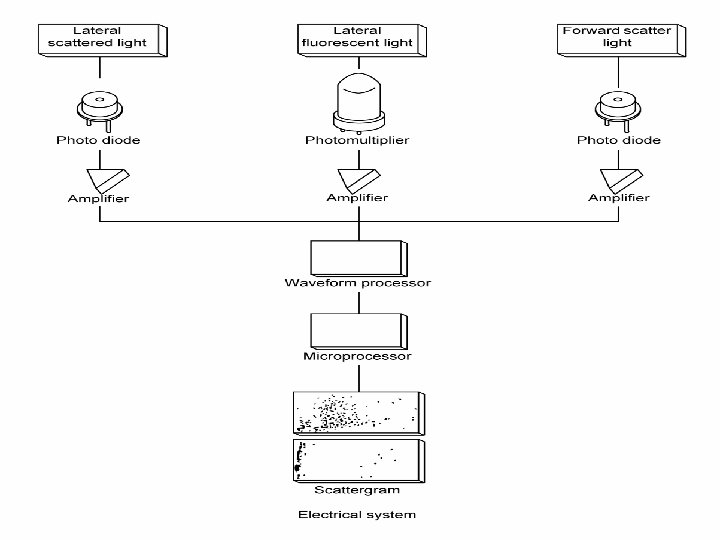
Sysmex UF-1000 i • Laser-based flow cytometer utilizing 2 stains with fluorescent dyes to stain cellular elements • Separate bacteria channel for improved discrimination • Forward scatter, hydrodynamic focusing, forward fluorescent light, conductivity measurements, and adaptive cluster analysis
Sysmex UF-1000 i System Components • Main unit with integrated pneumatic unit • IPU (information processing unit) Windows XP operating system • Sampler unit with tube rotator unit • Bar code reader • Laser Jet graphic printer/line printer (1 device, 2 settings) • Handheld bar code reader
UF-1000 i Tube Rotator
UF-1000 i Reagents UFII PACK™-BAC UFII SHEATH™ UFII PACK™-SED UFII SEARCH™ -BAC UFII SEARCH™-SED
UF II PACK-SED / UF II SEARCH-SED • UF II PACK-SED – Removal of amorphous salts together with heating (up to 35°C) • UF II SEARCH-SED – Polymethine dye – Chromogen chain with electron donor and acceptor group – Stains parts of nucleus, parts of cytoplasm and membranes – Excitation wavelength is 635 nm – Emission wavelength is over 660 nm
UF II PACK-BAC / UF II SEARCH-BAC • UF II PACK-BAC – UF II PACK-BAC (e. g. its p. H value) together with heating to >40°C suppresses non-specific staining of particles other than bacteria • UF II SEARCH-BAC – Polymethine dye – Distinctively stains nucleic acid elements in bacteria
UF-1000 i Sample Volumes • Minimum sample volume: – Manual mode: 1 m. L – Sampler mode: 4 m. L • Aspiration volume: – Manual mode: 800 µL – Sampler mode: 1, 200 µL • Processed sample volume (SRV) in sampler and manual mode: – 150 µL for the sediment analysis – 62. 5 µL for the bacteria analysis
UF-1000 i Manual Sample Page
Sample Volumes and Dilution • Addition of reagent leads to a dilution of the urine – for the SED analysis exactly by the factor 4: • 150 µL sample plus 435 µL diluent plus 15 µL dye equals 600 µL – for the BAC analysis exactly by the factor 8: • 62. 5 µL sample plus 425 µL diluent plus 12. 5 µL stain equals 500 µL
Sample Incubation • Incubation time at certain temperature ranges needed for staining – for the SED analysis: • 10 seconds at 35°C – for the BAC analysis: • 20 seconds at 42°C
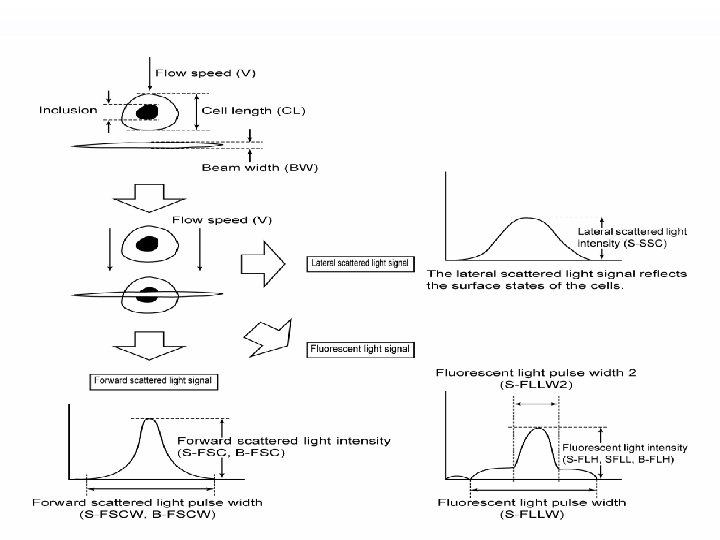
Laminar Flow Laser light Scattered light Flow cell particles Sheath nozzle Sheath reagent
UF-1000 i Scattergram Information • • Forward Scatter (FSC) Fluorescence High (FLH) Fluorescence Low (FLL) Fluorescence Low Width 2 (FLLW 2) Fluorescence Low Width (FLLW) Side Scatter (SSC) Forward Scatter Width (FSCW)
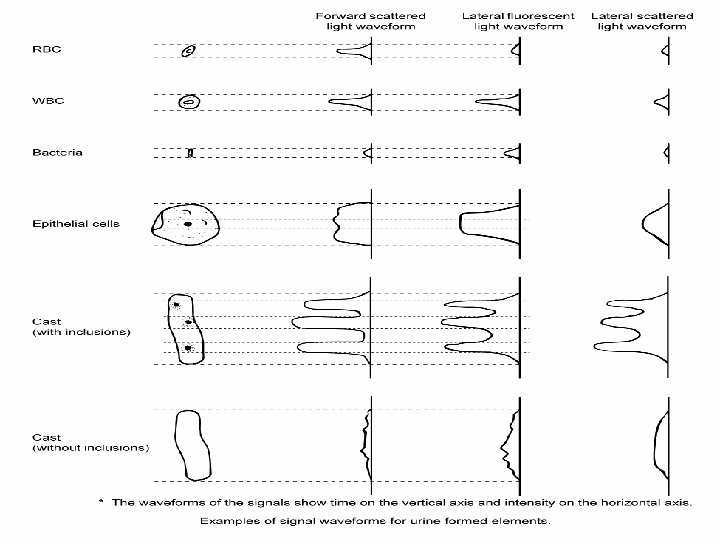
UF-1000 i Detection Parameters Enumerated Parameters Flagged Parameters RBC Pathological Casts WBC Crystals Epithelial Cells Small Round Cells Hyaline Casts Yeast Bacteria Mucus Sperm
S 1: FLH / Fsc Scattergram S_Fsc Size (sectional area) Large Fsc Small - large size X’TAL Fl WBC no fluorescence Fsc Small - medium size Fsc Medium - large size Fl Low fluorescence Fsc Fl C YL Low to medium fluorescence Fl RBC Fsc Small Bacteria Fl Low Medium - high fluorescence Small size Sperm Fsc Very small size Low fluorescence Fl Fluorescence Small size Medium fluorescence High S_FLH
S 2: FLL / Fsc - Scattergram S_Fsc Medium – very large size Size (sectional area) Large Medium - high fluorescence Fsc Small - medium size Fl Low fluorescence C L Y RBC Fl Fsc Small Bacteria Low Fsc WBC Fl EC Fsc Medium - large size Fl Medium - high fluorescence Small size Low to medium fluorescence Sperm Fsc Small size Very small size Fl Low fluorescence Fl Fluorescence Medium fluorescence High S_FLL
S 3: FLLW 2 / FLLW Scattergram S_FLLW 2 Length of stained inclusions Large FLLW 2 Little to more stainable inclusions FLLW Short – medium length of inclusions SRC Small WBC Short ls l e c l a Length of stained inclusions Path. casts No to little inclusions FLLW i el E th i p More stainable inclusions FLLW 2 Casts (no inclusions) Mucus Length of stained particle FLLW 2 No inclusions Long FLLW Long S_FLLW
B 1: Fsc / FLH - Scattergram B_FSC Large FSC Size of particles Small to big size FLH Debris No fluorescence BACT Fsc Fl. H Small size Weak fluorescence Small Low Stainability of particles High B_FLH
UF-1000 i Sediment 1
UF-1000 i Sediment 2
UF-1000 i Sediment 3
UF-1000 i Sediment 4
UF-1000 i Sediment 5
UF-1000 i Bacteria 1
UF-1000 i Bacteria 2
UF-1000 i Bacteria 3
UF-1000 i Technology Improved determination of bacteria Diluents Sediments Bacteria Incubation Detection unit Red semiconductor laser • Down sizing • Long life • Reduced power consumption Sediments Bacteria Stain Two chambers for stain and dilution
UF-1000 i Technology 1) Enhanced detection of bacteria Dye Dye Forward Scatter 2) Staining bacteria nuclei Dye Dye Dye Non-specific staining with debris Specific stain for Nucleic Acid Polymethine dye Stain DNA/RNA Fluorescence
UF-1000 i Technology Method Comparison UF-1000 i Parameters Parameter Correlation r Regression r 2 Regression Equation Range RBC 0. 9921 0. 9842 y = 0. 9544 x – 3. 0009 0. 0 – 4628. 1 WBC 0. 9669 0. 9348 y = 0. 8622 x – 1. 6818 0. 0 – 2557. 5 EC 0. 9777 0. 9558 y = 0. 864 x – 0. 1134 0. 0 – 176. 5 CAST 0. 9558 0. 9136 y = 0. 6125 x + 0. 0629 0. 00 – 28. 04 BACTERIA 0. 4831 0. 2334 y = 0. 1465 x – 51. 865 0. 0 – 9383. 4 The sediment parameters, RBC, WBC, EC and CAST, demonstrate excellent correlation with the UF-100 system. Source: Clinical Data for FDA submission
UF-1000 i Technology Method Comparison Percent Agreement 83. 22% Positive Predictive Value 91. 66% Negative Predictive Value 84. 30% A comparison of the data was performed to determine the percent agreement (bacteria count) of the samples based upon the different reference intervals listed below. UF-1000: ~1200/µL The bacteria reference intervals for the UF-1000 i were significantly lower than the UF 100. UF-100: ~ 2800/µL Source: Clinical Data for FDA submission
UF-1000 i Technology N=120 UF-1000 i REVIEW rate: 2. 6% RBC/X’TAL discrimination error 0 0. 0% RBC/BACT、DEBRIS discrimination error 2 1. 7% RBC/YLC discrimination error 0 0. 0% Conductivity error 1 0. 9% CARRYOVER 0 0. 0% Source: SCJ R&D Study UF-100 REVIEW rate: 6. 0% Total count error 2 1. 7% Discrimination error 0 0. 0% Conductivity error 1 0. 9% SRC* 5 4. 3% P. CAST* 1 0. 9% * Review setting is default
UF-1000 i Technology Scattergram UF-1000 i UF-100 Reduction of false-positive by X’TAL interference to RBC false-positive by X’TAL interference S-FSC Microscopy : RBC 5. 6/µL X’TAL (2+) The more complex the surface or inner construction, the more intensive SSC signal is. UF-1000 i: RBC 3. 3/µL X’TAL 102. 7/µL UF-100 : RBC 119. 8/µL X’TAL 0. 0 /µL
UF-1000 i Technology UF-1000 i Scattergram Microscopy: EC 24. 5/µL Reduced false positive EC with high positive WBC UF-100 WBC is accurately classified by SSC signals. SSC parameters can help UF to distinguish WBC and EC. UF-1000 i: EC 18. 2/µL WBC cluster can be detected as EC. It is false positive of EC. UF-100 : EC 83. 4/µL
UF-1000 i Data Storage • HDD with minimum 20 GB for data storage including graphics • Sample Explorer/Data Browser: 10, 000 samples measurement data including histograms & scattergrams • Work List: 3, 000 orders • Patient information: 5, 000 patients data • 100 reagent logs & error logs • Doctor & ward master
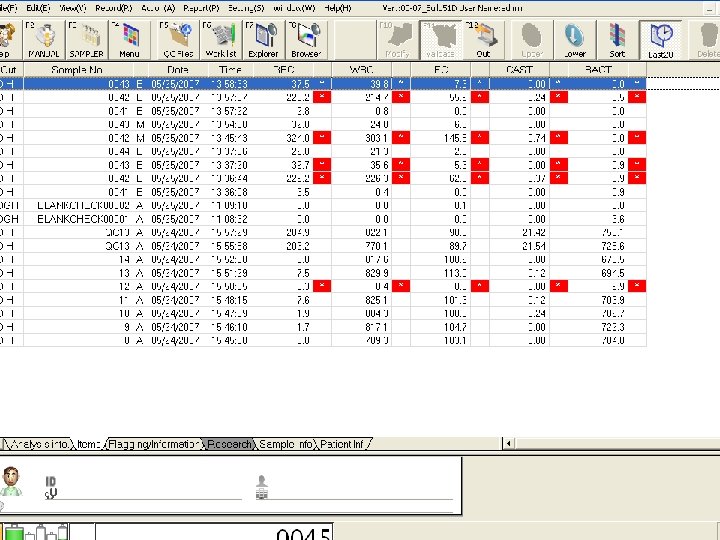
UF-1000 i Sample with No Flagging
UF-1000 i Sample with Flagging
UF-1000 i “Cumulative” screen
UF-1000 i “Service 1” screen
UF-1000 i “Service 2” screen
UF-1000 i Anti-Carryover Action • Trigger: bacteria count only • Sequential mode: – If the bacteria count exceeds the cut-offs preset in the anti-carry-over settings, additional autorinse cycles are performed before the next sample is aspirated. • Overlapping mode: – If the bacteria count exceeds the cut-offs preset in the anti-carry-over settings, additional autorinse cycles are performed. The next sample will be aspirated twice.
UF-1000 i Anti-Carryover
UF-1000 i Quality Control • UF II Control: two level commercial controls containing particles representing RBC, WBC, EC, casts, and bacteria • Controls also monitor conductivity plus the high level monitors sensitivity parameters-FSC, FSCW, FLH, FLLW, SSC. • Levy Jennings & Radar Charts
UF-1000 i 24 Control Files
UF-1000 i QC Charts L-J Charts Radar Charts 300 data points
UF-1000 i Flagging (Review Settings) • • • X’TAL: YLC: SRC: Path. CAST: MUCUS: SPERM: 25. 0/u. L 10. 0/u. L 1. 5/u. L 10. 0/u. L
UF-1000 i Q-Flags
UF-1000 i Factory Defined Review Flags • • • RBC/X’TAL Abn. Cls. : RBC/BACT Abn. Cls. : RBC/YLC Abn. Cls. : Debris High? : Abn. DC Sensitivity: • Carryover? : RBC*, BACT* RBC* BACT* ≤ 3. 0 or ≥ 39. 0 m. S/cm BACT*
UF-1000 i Linearity • • • RBC: 1. 0 -5000. 0/u. L WBC: 1. 0 -5000. 0/u. L EC: 1. 0 -200. 0/u. L Casts: 1. 0 -30. 0/u. L Bacteria: -5. 0 -10, 000. 0/u. L
UF-1000 i Reference Intervals • • • RBC: ≤ 23. 0/u. L WBC: ≤ 28. 0/u. L EC: ≤ 31. 0/u. L Casts: ≤ 1. 00/u. L Bacteria: ≤ 358. 0/u. L
UF-1000 i Maintenance • Daily – Perform shutdown – Check for fluid in trap chamber of Pneumatic Unit & empty if needed • Monthly or every 9000 cycles – Clean the sample rotor valve (SRV) • As Needed – Clean or replace sample filter if clogged or aspiration is affected – Empty waste container if not connected to floor drain
UF-1000 i • • Walk-away system Uses uncentrifuged urine sample No interference with amorphous urates Results in 1 minute; cells reported/u. L or /HPF or /LPF • Review only by exception; no image review
Benefits of Automated Urine Microscopy • Objective, analytical measurements • Reduction of subjective identification of elements • Reduction of tech to tech variability • Improved accuracy and reproducibility • Improved workflow, productivity, efficiency, turnaround time • Decreased labor expense
YH Urinalysis Automation Objectives • Annual UA volume: 58, 000; 78% microscopics • Automated dipstick analysis with Clinitek Atlas system (sample tray) in 8/95. • Updated to Clinitek Atlas Rack system in 4/03. • Decision to automate urine sediment analysis with the Sysmex UF-100. “Live date” June 4, 2001. UF-1000 i installed 12/07.
YH Benefits Using Automated Sediment Analysis • Reduced manual microscopic review rate to ~11% • Reduced turnaround time to <30 minutes from >60 minutes • Reduction of 1 FTE through attrition • Improved workflow: can operate Urinalysis Department with ~1. 5 FTE instead of 3. 0 FTE • Reduction in number of urine cultures • Culture criteria: WBC >28/u. L, bacteria >358/u. L, & positive urine nitrite
YH Benefits Using Automated Sediment Analysis (cont. ) • ~15% volume increase since 2001 with no additional staffing required; current fiscal year-no volume increase • Minimal maintenance • >99% uptime • Smooth transition; very few physician concerns or questions
Thank You!
Questions?