Hypertension Cardiovascular Risk Factors Final Year Cardiology Teaching



 1990 Rank Cause 2020 % Rank Cause")



































 or -blocker Calcium antagonist C")




- Slides: 56
Hypertension & Cardiovascular Risk Factors Final Year Cardiology Teaching 2003 -4
Outline • Global burden of cardiovascular disease • Epidemiology of cardiovascular disease • Hypertension – Epidemiology – Clinical features – Investigation • Cardiovascular risk assessment
The Global Burden of Disease The scope of the problem
Leading Causes of Death and Disability (DALY’s) 1990 Rank Cause 2020 % Rank Cause % 1 Lower respiratory infections 8. 2 1 Ischemic heart disease 5. 9 2 Diarrhoeal diseases 7. 2 2 Major depression 5. 7 3 Perinatal conditions 6. 7 3 Road traffic accidents 5. 1 4 Major depression 3. 7 4 Cerebrovascular disease 4. 4 5 Ischemic heart disease 3. 4 5 COPD 4. 2 6 Cerebrovascular disease 2. 8 6 Lower respiratory infections 3. 1 7 Tuberculosis 2. 8 7 Tuberculosis 3. 0 8 Measles 2. 7 8 War 3. 0 9 Road traffic accidents 2. 5 9 Diarrhoeal diseases 2. 7 10 Congenital abnormalities 2. 4 10 HIV 2. 6 Global Burden of Disease Study, 1996
Mortality due to leading global risk factors * ** * World Health Report 2002
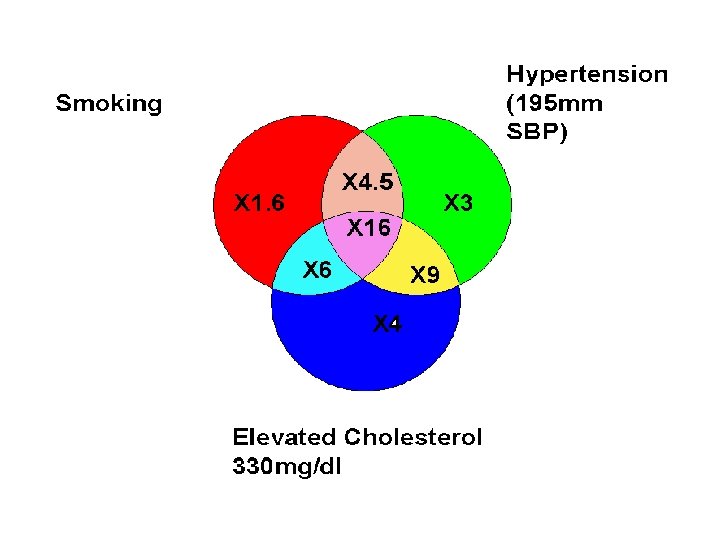
Cardiovascular risk factors Blood pressure Lipids Diabetes Smoking
BP and relative risk of stroke and CHD Stroke CHD 4. 00 2. 00 1. 00 0. 50 0. 25 123 76 136 84 148 91 162 98 175 105 Approximate mean usual BP 123 76 136 148 84 91 162 175 98 105 Approximate mean usual BP Brit Med Bull 1994; 50: 272 -98
Average annual rate/ 10, 000 Blood Pressure and Risk of Congestive Heart Failure: the Framingham Study Normotensive BP <140/90 mm. Hg Hypertensive BP >160/95 mm. Hg Age at examination Kannel et al. 1972
Incidence / 100, 000 person years Systolic BP as a risk factor for renal failure Systolic BP, mm. Hg MRFIT ‘screenees’ Klag MJ, JAMA ‘ 97; 277: 1293
Cholesterol and risk of CHD & cardiovascular death 4. 00 Coronary Heart Disease Cardiovascular Death (51652 participants, 310 events) (9 studies, 49296 participants, 938 events) 4. 00 (51652 participants, 310 events) Relative Risk 2. 00 1. 00 0. 50 0. 25 4. 0 4. 5 5. 0 5. 5 6. 0 Approximate mean usual cholesterol (mmol/l) Eastern Stroke & Coronary Heart Disease Project
Relative risk Association between cholesterol and ischemic stroke 4. 0 4. 5 5. 0 5. 5 6. 0 Approximate mean usual cholesterol concentration (mmol/L) Asia Pacific Cohort Studies Collaboration
Worldwide Prevalence of Diabetes 1997
Risks of death in diabetics and non-diabetics All cause Non-CVD All CVD Other CVD CHF CHD Stroke Non-diabetics Diabetics Asia-Pacific Cohort Studies Collaboration
Smoking
Premature Deaths From Tobacco Use Preventable if adults quit (halving global cigarette consumption by 2020) Preventable if young adults do not start (halving global uptake by 2020) Other premature deaths from tobacco-related causes 2000 -2024 2025 -2049 The World Health Report, 1999: Making a Difference
Blood Pressure or Hypertension?
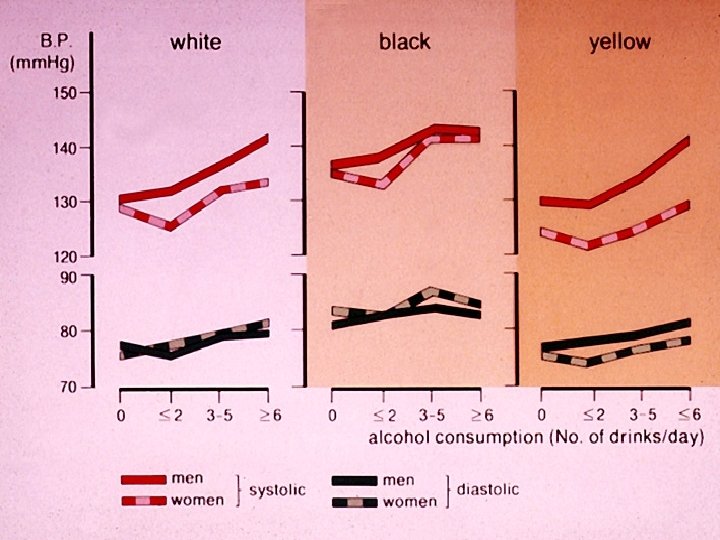
Hypertension and alcohol C. Lian, French army physician, 1915 30 % hypertensive 25 20 15 10 5 0 Sobres Moyens Buveurs Grands Buveurs Sobres Moyens buveurs: Grands buveurs: Tres grands buveurs: Tres Grands Buveurs <1 litre wine/ day 1 -1. 5 litres wine/ day 2 -2. 5 litres wine/ day 3 litres wine/ day + 4 -6 aperitifs
Blood Pressure or Hypertension?
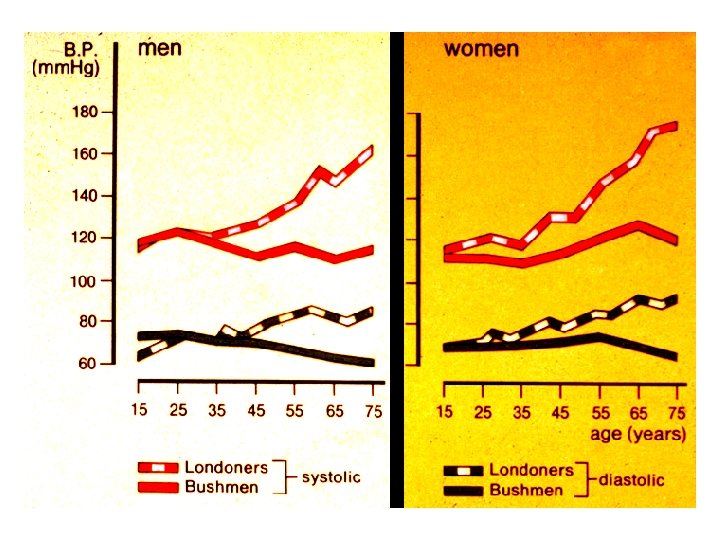
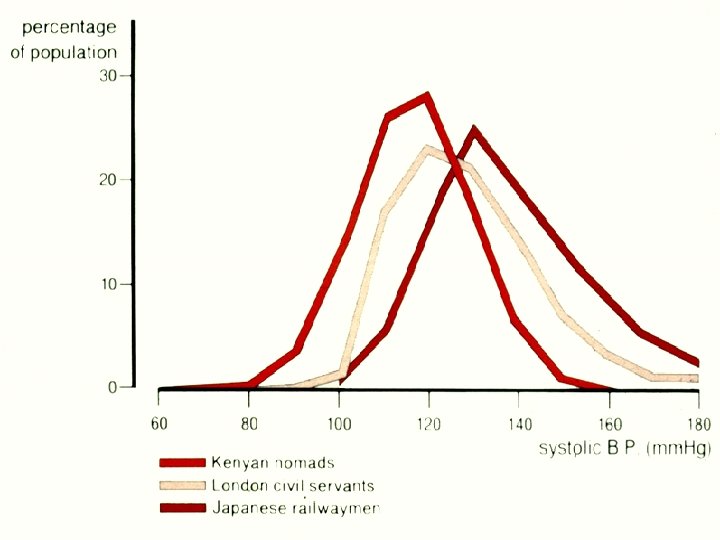
% of screened population The ‘normal’ distribution of diastolic BP within a population 50 60 70 80 90 100 Diastolic BP, mm. Hg 110 120 130
Hypertension: a practical definition That level of blood pressure at which investigation and treatment do less harm than good Rose
Assessment of the Hypertensive Patient
Hypertension risk factors Weight Family history Salt, Alcohol, Stress Concurrent conditions Clues to 2 o HT Asthma Gout Pregnancy Symptoms Drugs Signs History + Examination Other CV risk factors Target organ damage Lipids Smoking Diabetes Exercise Heart Brain Eyes Kidneys
Investigations • Urine • Blood • ECG ? Specialised investigations • • • Renal USS 24 -hour ABPM Echocardiography Angiography Hormone assays CT / MRI scanning
Indications for further investigations • • Clinical features of an underlying cause Early onset (< 30 y) Rapid progression Proteinuria, haematuria, glycosuria Severe hypertension, difficult to control Vascular disease: peripheral, coronary, carotid Heart failure, ‘flash’ pulmonary oedema Lack of nocturnal dip on ABPM
Secondary causes of hypertension… …. comprise a small proportion of overall cases, probably < 5%
The Heinz guide to hypertension Renal artery stenosis Pyelonephritis Obstruct nephropathy Vesico-ureteric reflux Ask-Upmark kidney Renal dysplasia Renin JGA tumor Glomerulonephritis Polycystic disease Analgesic kidney Systemic sclerosis ITT purpura Haemolytic uremic 1 o Aldosteronism Cushing’s syndrome Phaeochromocytoma DOC excess Cong adrenal h’plasia Gluc remediable Diabetes Amyloidosis Carbenoxalone Obstruct sleep apnoea Alcohol MAO-I inhibitors Pre-eclampsia Liquorice Sympathomimetics Chronic renal failure Poliomyelitis 11 - OH-St dehyd def Porphyria Acromegaly Aortic coarctation intracranial pressure Oral contraceptive Endothelinoma Lead poisoning Corticosteroids
Secondary causes of hypertension Renal artery stenosis
Secondary causes of hypertension Polycystic kidney Phaeochromocytoma
Phaeochromocytoma MIBG scan
Target Organ Damage & Complications of Hypertension
Target organ damage: left ventricular hypertrophy
Target organ damage: hypertensive retinopathy
Grade 4 hypertensive retinopathy
Complications of hypertension Intra-cerebral haemorrhage Myocardial infarction in hypertrophied left ventricle
Management of Hypertension Non-pharmacological/ lifestyle Pharmacological
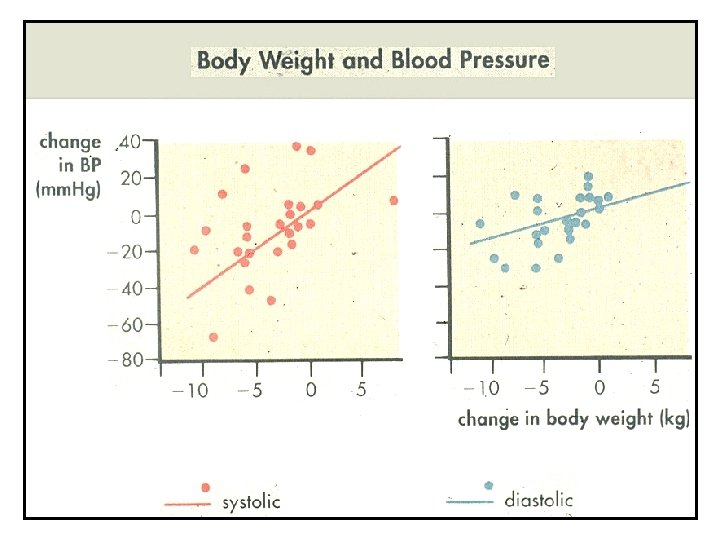
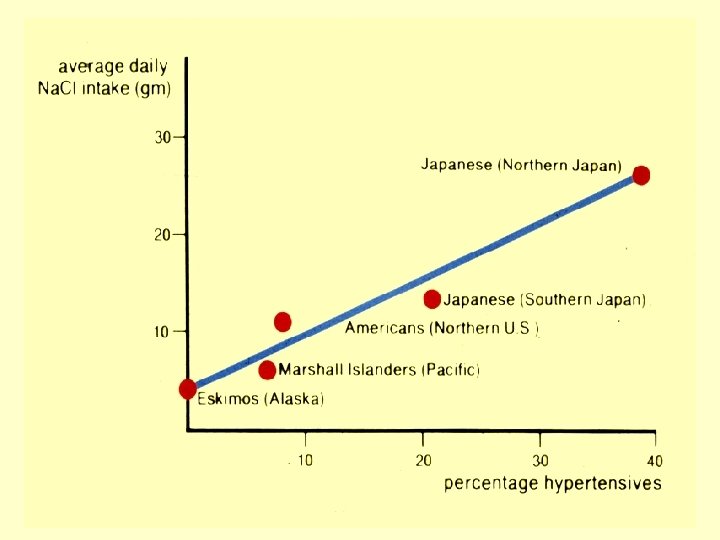
Non-pharmacological interventions Measures that lower blood pressure: l l l weight salt intake alcohol consumption physical exercise fruit & vegetable consumption Measures to reduce cardiovascular risk: l l Stop smoking saturated fat, poly- & mono-unsaturates oily fish consumption total fat intake BHS Guidelines 1999
The Mediterranean Diet
BP lowering treatment and cardiovascular risk Total number of individuals affected 1200 Non-fatal events Fatal events 1000 T 800 T=treatment C=control C T C 600 400 T T C C 200 % reduction in odds Stroke CHD 38% SD 4 16% SD 4 All vascular deaths All other deaths Brit Med Bull 1994; 50: 272 -98
Drug treatment of hypertension Diuretic Calcium-channel blocker Beta-blocker l l ACE-inhibitor Angiotensin receptor blocker (Alpha-blocker) Most hypertensives will need 2 drugs to control BP Drug combinations may be synergistic
How to choose anti-hypertensive therapy ACE inhibitor (AII antagonist) or -blocker Calcium antagonist C A B Diuretic One drug: Younger, non-black A or B Older, black C or D Two drugs: (A or B) + (C or D) Three drugs: (A or B) + C + D D
Target blood pressure < 140/90 mm. Hg …. except in those with diabetes or chronic renal disease < 130/80 mm. Hg
Cholesterol & cardiovascular disease
“Large randomised trials demonstrate lowering LDLcholesterol by 1 mmol/l reduces non-fatal MI and fatal CHD by about 25% ( about half the effect predicted from epidemiological studies for a similar reduction in long term cholesterol lowering in people without vascular disease ) “ Collins 2002 With greater reductions in cholesterol there are correspondingly larger reductions in CHD endpoints.
Landmark Statin Trials: LDL-C Levels vs Events at 5 Years Follow-up Percentage with CHD event 4 S-P 25 20 15 10 5 0 4 S-S HPSh-P LIPID-P CARE-P HPSh-S CARE-S HPSl-S LIPID-S WOSCOPS-P ASCOT-P* ASCOT-S* AFCAPS-S 2. 3 (90) Secondary prevention Primary prevention Simvastatin Pravastatin 2. 8 (110) 3. 4 (130) HPSl-P WOSCOPS-S Atorvastatin AFCAPS-P 3. 9 (150) 4. 4 (170) LDL-C, mmol/L (mg/d. L) S=statin treated; P=placebo treated * Extrapolated to 5 Years Modified from Kastelein JJP. Atherosclerosis. 1999; 143(suppl 1): S 17 -S 21. Lovastatin 4. 9 (190) 5. 4 (210)