Introduction to pediatric cardiology Diseases in pediatric cardiology

 cardiomyopathies inflammatory diseases (endo/myo/peri)")




 Ø warm Ø decreased sat. O 2 in arterial")










 in precordial leads in a")





 - „rib")





 • Iodine contrast material –")






 Iodium contrast agent High spatial resolution 0,")
 2) 3) 4) 5) 6) 7) 8) regularity rhythm frequency Electric")
- Slides: 45
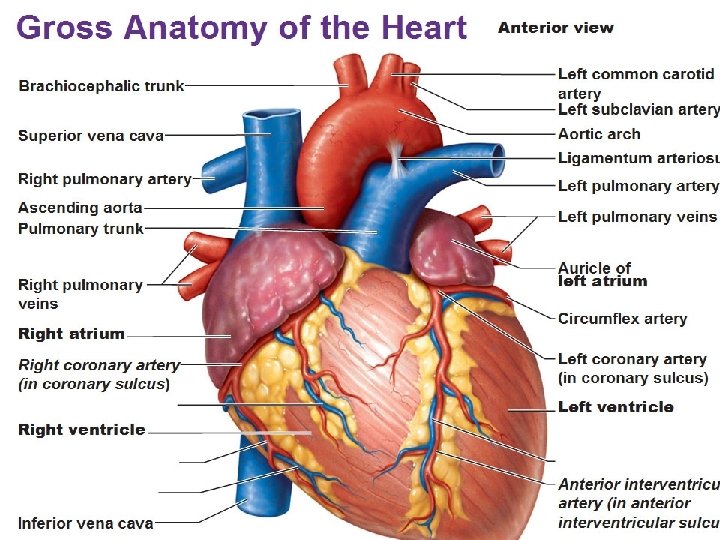
Introduction to pediatric cardiology
Diseases in pediatric cardiology • • VCC (vitium cordis congenitum) cardiomyopathies inflammatory diseases (endo/myo/peri) arrhythmias systemic arterial hypertension pulmonary hypertension cardiac tumors
Pathological clinical signs in pediatric cardiology • • Organic murmurs Central / peripheral cyanosis Dyspnoe, tachypnoe Failure to thrive Pathological hepatomegaly Syncopes (cardiac are associated with physical excercise) Arrhythmias Chest pain (cardiac are associated with physical excercise cardiac cause is very rare)
Heart auscultation !!! Auscultation also at the back: murmur in Co. A / propagation of systolic murmur in pulmonary valvular stenosis
Murmurs • AS • AR • Pericard friction rub • Classification Ø organic (5 -10%) a innocent (90 -95%) Ø systolic, diastolic a continual 1) 2) 3) 4) timing (systoly/diastoly) punctum maximum intensity – Levin scale of intensity propagation
Innocent murmur • • Always systolic Max 3/6 No thrilling Changing with body position No other clinical symptoms No ECG changes Not associated with VCC
Cyanosis • Central (cyanotic VCC) Ø warm Ø decreased sat. O 2 in arterial blood Ø blue tongue and mucouse membranes Ø polyglobulia clubbing, tromboembolism • Peripheral (heart failure) Ø cold Ø low CO a other shocks Ø sat. O 2 in arterial blood normal Ø decresed venous sat. O 2 Ø akrocyanosis
Peripheral cyanosis Central cyanosis Clubbing
Clinical signs of cardiac failure in babies • Pathological hepathomegaly • Oedemas in gluteal and perigenital regions • Failure to thrive • Cold periphery • Compensational sinus tachycardia • Dyspnoe / tachypnoe
Dyspnoe a tachypnoe • dyspnoe • tachypnoe Ø age of patient !!!!
Fetoplacentar circulation: right ventricle volume and pressure overload, high pulmonary vascular resistance Fetal circulation After the birth: slow decrease of pulmonary vascular resistance = regression of right ventricle hypertrophy Physiological dominance (hypertrophy) of left ventricle since 1 year of age (It is determined by 5 to 10 – times higher systemic vascular resistance in comparison to pulmonary vascular resistance
Investigation methods in pediatric cardiology ECG Chest X-ray ECHOcardiography Cathetrizational angiography CT-angiography Cardiac MRI Blood pressure 24 -hours Holter monitoring Spiroergometry Lab. Paramethers: NT-pro. BNP, Troponin-T
Electrocardiography – detects electric myocardial potencials
ECG • Electric potentials detection Types of ECG detection • 12 -lead ECG • ECG 24 -hours Holter • event recorder
ECG Electrodes
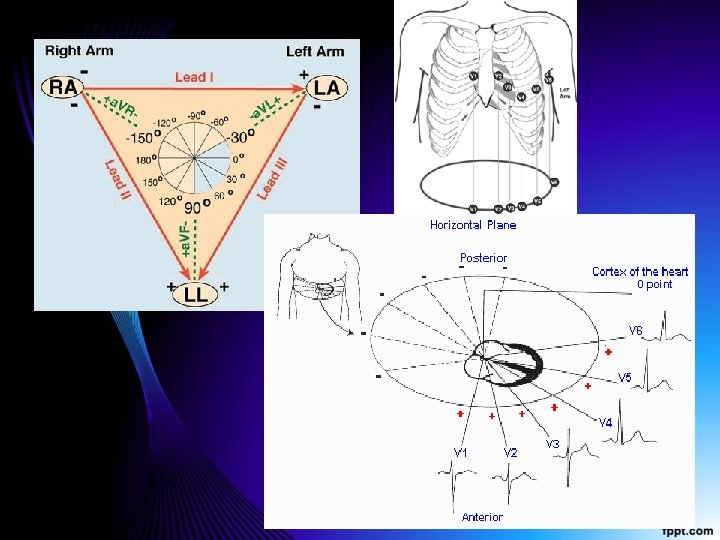
Myocardial electric axis determination • Can be obtained from bipolar leads I. and a. VF (perpendicular leads) • We evaluate the dominancy of either R wave or S wave in both leads
Myocardial electric axis in a neonate is cca +120 st. (determined by physiological right ventricle hypertrophy) Myocardial electric axis in an adolescent is cca +60 st. (determined by physiological left ventricle hypertrophy)
High R waves over right precordium (V 1, 2) in precordial leads in a neonate (determined by physiological right ventricle hypertrophy) and low R waves over left precordium (V 5, 6) Deep S waves and low R waves over right precordium (V 1, 2) in precordial leads in a 8 -years old child and high R waves over left precordium (V 5, 6) (determined by physiological left ventricle hypertrophy)
Sinus tachycardia and bradycardia in children • The age have to be into account!!! • Newborn normal values: 100 -160 pulzov / min • Adolescent normal values: 60 -100 pulzov / min • Various ethiology • On ECG: P wave positive in leads I. , II. , a. VF and negative in leads a. VR sinus rhythm!
Respiratory arrhythmia = increase of heart frequency during inspiration / decrease of heart frequency during expiration = physiological finding
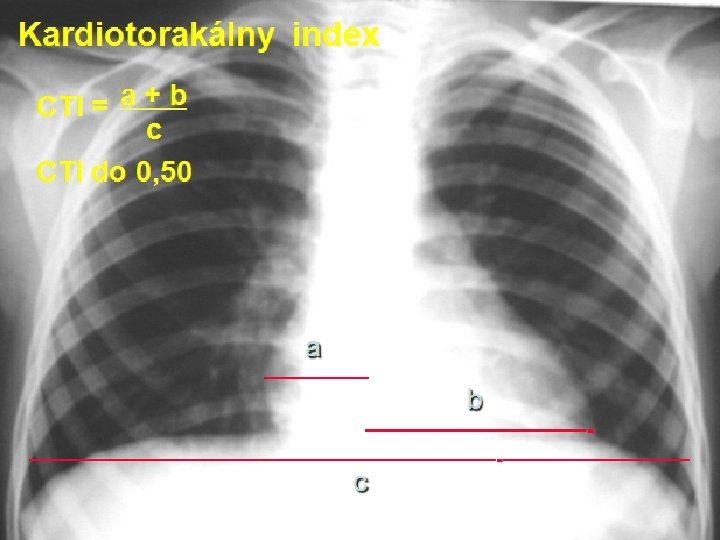
Chest X-ray – shadows of of each heart parts
Normal heart size – CTI 0, 45 Cardiomegalu – increased CTI 0, 8
Chest X-ray – atypical shape of the heart – typical for Tetralogy of Fallot = Heart apex is elevated and shifted to the left (yellow arrows), bilateral decreased pulmonary lung perfusion determined by pulmonary stenosis
Chest X ray – typical „three“ sign in aortic coarctation (Co. A) - „rib notching“ sign in Co. A (detemined by compression of developing ribs by arterial collaterals)
Chest X-ray „cor bovinum“ in dilated cardiomyopathy pericardial effusion
Echocardiography – dominant imaging modality • • probes 1 -10 MHz Higher fr. = lower penetration newborns 7 -10 MHz adolescents 3 -4 MHz
Transthoracic ECHO
ECHO - D-transposition of great arteries
Catheterizational angiography – invasive method (imaging of cardiovascular system) • Iodine contrast material – applied in cardiovascular system after cannullation of central venous cathether in femoral vein or artery • !!!! RTG radiation
Cathetrizational angiography
CT-angiography
Cardiac CT-angiography 3 D-virtual reconstruction 2 D - Frontálnyview
CT angiography Multiplanar reconstruction
Cardiac MRI Image of 3 -leaflet aortic valve
MR kardio Image of hypertrophied left ventricle in valvular aortic stenosis
CT • • Radiation Fast aquisition (seconds) Iodium contrast agent High spatial resolution 0, 5 mm slice thickness • Better available • Cheaper • Pacemakers/ICD: OK MR • • No radiation Slow aquisition (min – 1 hour) Gad contrast agent +/Lower spatial resolution 1 -3 mm slice thickness Evaluation: chamber volumes, systolic function, valves, flows tissue characterization Low available More expensive Pacemakers/ICD: contraindic.
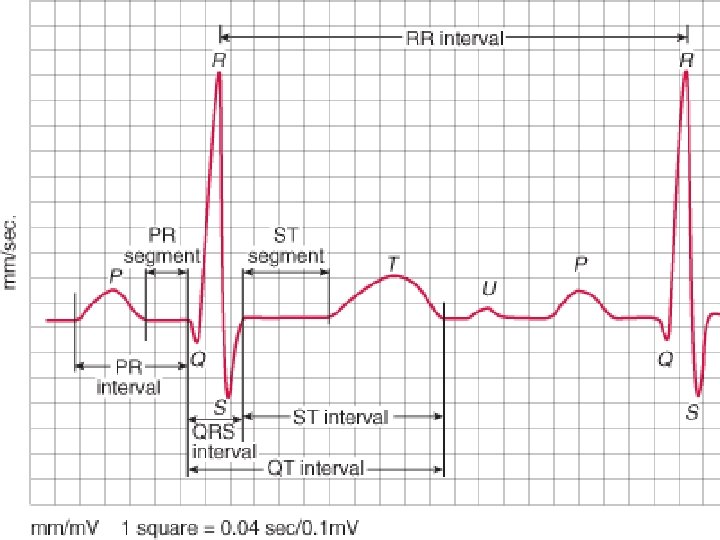
ECG evaluation 1) 2) 3) 4) 5) 6) 7) 8) regularity rhythm frequency Electric axis intervals – PQ, QRS, QT Morfology and QRS voltage ST segments changes T waves