Cardiology Cardiology Phase 2 a Revision Session Ryad





 • 95%")



 - Truncus Arteriosus - Transposition of Great")
 L->R Shunts - VSD - ASD - PDA Eisenmenger Syndrome")


 CVD RF’s AE •")




 Not Each Followed by QRS")


 • PR interval is constant and")

")
")
 Heart Block")
 Regular Irregular Atrial • Sinus tachycardia • Atrial flutter")





- Slides: 39
Cardiology
Cardiology Phase 2 a Revision Session Ryad Chebbout Abdullah Aamir 10/03/17 The Peer Teaching Society is not liable for false or misleading information…
Content • Hypertension • Heart Failure • Congenital Heart • Shock Disease • Limb Claudication / • Valvular Disease Ischaemia • Dysrhythmias • Ischaemic Heart Disease • Pericarditis
Cardiac Presentation Symptoms • Chest Pain • Shortness of Breath • Palpitations • Syncope • Cough Signs • Murmur • JVP • Peripheral oedema • Pulse changes • Lung base changes • Tachycardia, Bradycardia • Hypotension, Hypertension
Hypertension
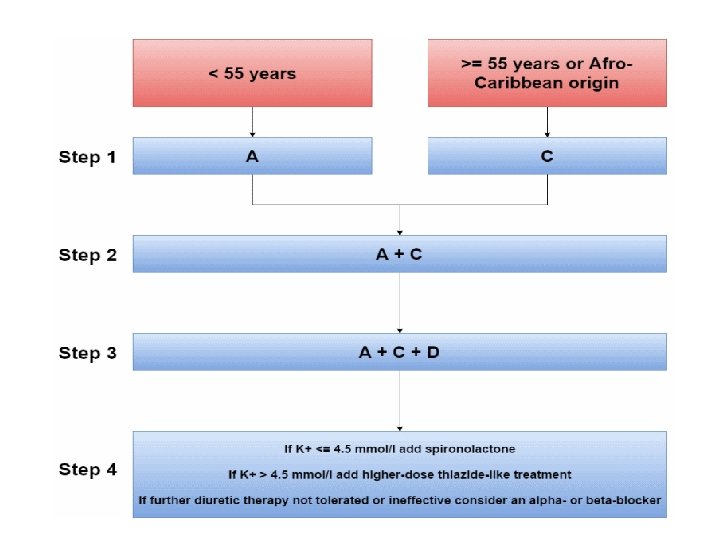
Hypertension • Modifiable CVD risk factor (e. g. IHD, ACS, CVE, PVD) • 95% = Essential HTN (unknown aetiology) • Exclude secondary causes (5%) • Check for end-organ damage (renal, endocrine, CVD, drugs) • Pharmacological management alongside managing other modifiable CVD risk factors (e. g. hyperlipidaemia, DM etc…)
Hypertensive Emergencies Crisis = >200/>120 • Emergency: High BP + Acute End-Organ Damage • Urgency: High BP (no end-organ damage) Symptoms of acute end-organ damage: • Neuro: headache, N+V, confusion, retinopathy, papilloedema, weakness • CVD: chest pain, SOB • Renal: oliguria/anuria Slowly reduce BP!!!
Congenital Heart Disease
Foetal Circulation
Congenital Heart Disease R->L Shunts (4 T’s) - Truncus Arteriosus - Transposition of Great Vessels - Tricuspid Atresia - Tetralogy of Fallot Early Cyanosis (blue babies) Urgent Surgical Correction/Maintenance of PDA
Congenital Heart Disease (2) L->R Shunts - VSD - ASD - PDA Eisenmenger Syndrome (VSD/ASD/PDA) L->R Shunt = Increased Pulmonary Pressure = PAH = RVH = R->L Shunt Late Cyanosis (blue kids) Surgery
Valvular Heart Disease
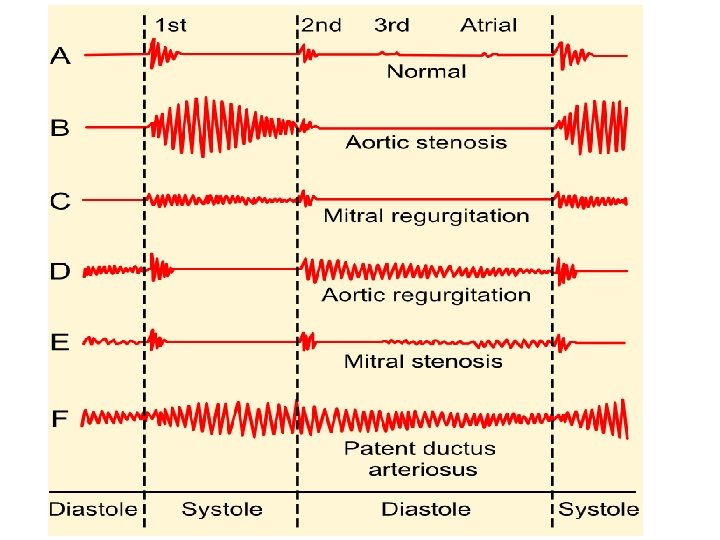
Mitral Regurgitation PATH • MR = LA Dilatation = P. Venous HTN = P. HTN • MR = LV Dilatation = LV Hypertrophy = LVF (vol. overload) AE • IHD (Post-MI) • Annular Calcification (degenerative) • RF/IE SYM • SOB • Fatigue SIG • Murmur • Displaced Hyperdynamic Apex • AF INV • ECG (AF, P-mitrale, LVH) • CXR • Echo Mx • None • Surgery
Aortic Stenosis AE • LV Hypertrophy = LVF (pressure overload) CVD RF’s AE • Calcification (degenerative) • Congenital (bicuspid) • RF SYM • Syncope • Angina • SOB SIG • Murmur • Pulsus Tardus et Parvus (slowrising) INV • ECG (P-mitrale, LVH, LAD) • CXR • Echo Mx • None • Surgery
Rheumatic Fever
Infective Endocarditis
Dysrhythmias
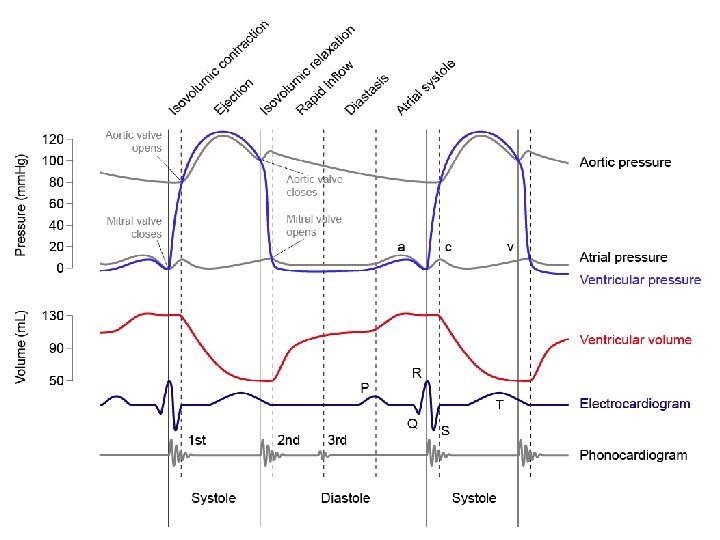
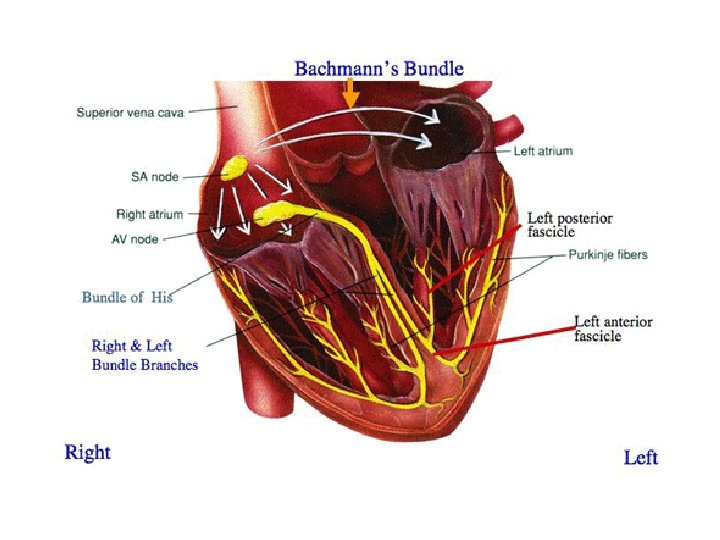
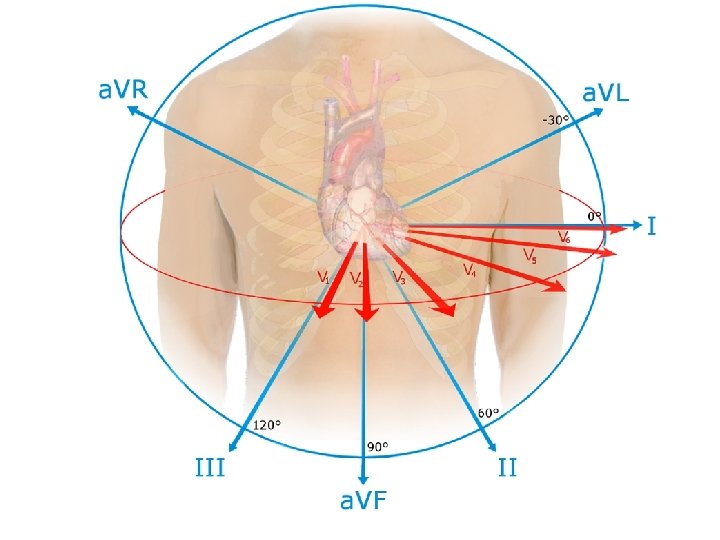
Normal Adult ECG
Bradycardia P Waves Each Followed by QRS (SAN dysfunction) Not Each Followed by QRS (AVN dysfunction) • Sinus bradycardia • 2 nd Heart block • Sick sinus syndrome • 3 rd Heart block (1 st Heart block)
Sinus Bradycardia
AVN/Heart Block 1 st Degree • Benign and asymptomatic. No treatment required. AE • Increased vagal tone (athletes) • Inferior MI • Mitral valve surgery • AVN blocking drugs (betablockers, CCB, digoxin) 2 nd Degree (Mobitz type 1) • Progressive lengthening of PR interval until beat is “dropped” (excitation completely feels to pass through AVN/bundle of His) AE • AVN blocking drugs (betablockers, CCB, digoxin) • Increased vagal tone • Inferior MI
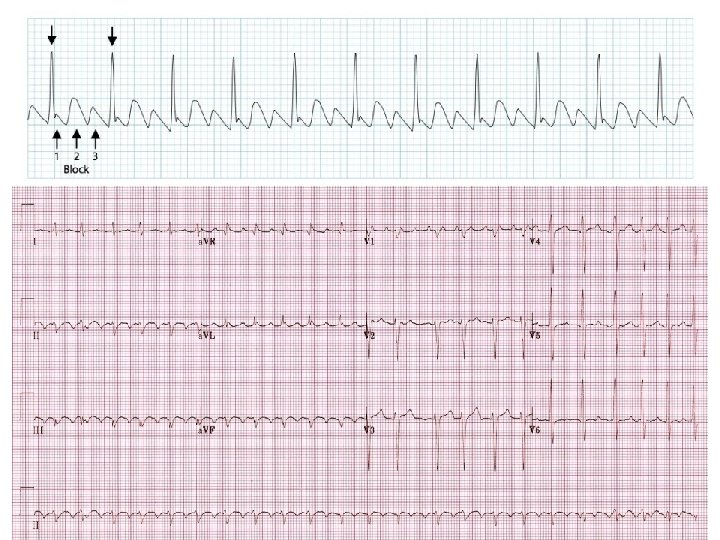
AVN/Heart Block 2 nd Degree (Mobits type 2) • PR interval is constant and QRS complex dropped • Failure of conduction through His-Purkinje system • ASSOC: LBBB, bifascicular block • May be symptomatic (syncope) 3 rd Degree / Complete Heart Block • Complete absence of AV conduction • Rhythm is maintained by junctional or ventricular escape rhythm • May be ventricular standstill = syncope / sudden cardiac death AE • Anterior MI • Mitral valve surgery • SLE, RF, Lyme AE • Inferior MI • AVN blocking drugs (CCB, beta-blockers, digoxin)
1 st Degree Heart Block
2 nd Degree Heart Block (Mobitz type I)
2 nd Degree Heart Block (Mobitz type II)
3 rd Degree (Complete) Heart Block
Tachycardia – Narrow Complex (SVT) Regular Irregular Atrial • Sinus tachycardia • Atrial flutter • Atrial fibrillation • Atrial flutter with variable block • Multifocal atrial tachycardia Atrioventricular • AV re-entry tachycardia (AVRT) • AV nodal re-entry tachycardia (AVNRT) • Automatic junctional tachycardia
Sinus Tachycardia
Atrial Flutter PATH • A type of SVT caused by a re-entrant circuit within the right atrium AE • Idiopathic, IHD, atrial dilatation (septal defect, PE, mitral/tricuspid disease) ECG • Regular atrial rate of ~300 bpm (200 -400 bpm, depends on size of right atrium) • Ventricular rate determined by the AV conduction ratio: 2: 1 (commonest), 3: 1, 4: 1, variable rate • ‘Sawtooth’ pattern, best seen in II/III/VF, narrow complex QRS
AVNRT/AVRT
Atrial Fibrillation PATH • AVN bombarded with depolarisation waves of varying strength, and only conducts in ‘all or non fashion’ • Initiating event (e. g. PAC) + Substrate for maintenance (e. g. dilated left atrium) • First Episode, Recurrent (>2 episodes), Paroxysmal (self-terminates <7 d), Persistent (>7 d), Permanent (>1 yr) AE • • • IHD HTN PE Hyperthyroidism Mitral Valve Disease PRES • Asymptomatic • Chest Pain, Palpitations, SOB Mx • (acute) Cardioversion (electrical / amiodarone) • • (Chronic) Rate Control: Beta-Blocker / CCB / Digoxin (HF) Rhythm Control: Cardioversion (electrical / amiodarone) Anticoagulation: Warfarin (post. TIA/Stroke) COMP • CVE
Atrial Fibrillation