Pharmacology Pharmacology Phase 2 a Pharmacology Ryad Chebbout

Pharmacology

Pharmacology Phase 2 a Pharmacology Ryad Chebbout 24/04/17 The Peer Teaching Society is not liable for false or misleading information…

Contents • • Pharmacokinetics Pharmacodynamics Autonomic nervous system Central nervous system Infection Cardiovascular system Endocrine system Poisoning The Peer Teaching Society is not liable for false or misleading information…
 • Enteric-coated (intestinal absorption, e. g. aspirin) • Extended-release")
Route of Administration Enteral (oral) • Enteric-coated (intestinal absorption, e. g. aspirin) • Extended-release (slower absorption, e. g. metformin) • Sublingual/Buccal (rapid absorption + avoids 1 st pass metabolism) Parenteral (systemic circulation) • Intravenous • Intramuscular (antipsychotics) • Subcutaneous (insulin) Other • Inhalation (oral, nasal) • Topical • Rectal

Pharmacokinetics Definition • What the body does to a drug Properties 1. Absorption (into plasma) 2. Distribution (to intra/extracellular fluid) 3. Metabolism (e. g. liver, kidney) 4. Elimination (e. g. urine, bile, faeces)
 • Passive diffusion • Facilitated diffusion •")
1. Absorption Mechanisms (e. g. GI mucosa) • Passive diffusion • Facilitated diffusion • Active transport • Endocytosis Variables of Absorption • p. H • Vascularity (e. g. shock reduces SC absorption) • Surface area • Contact time (e. g. with food = slower gastric emptying)

Bioavailability Definition • Rate and extent to which an administered drug reaches the systemic circulation (e. g. IV = 100%)
")
Bioavailability Factors • First Pass Hepatic Metabolism (hepatic transformation of drug to inactive metabolites) • Solubility • Chemical instability (e. g. GI enzyme destruction of insulin)

2. Distribution Definition • Drug reversibly leaves bloodstream and enters the extracellular fluid and tissues Factors • Blood flow (e. g. brain > muscles) • Capillary permeability • Plasma protein binding (e. g. albumin) • Tissue protein binding (e. g. cyclophosphamide accumulating in bladder leading to cystitis) • Lipophilicity (ability to cross cell membranes)

3. Metabolism Definition • Process of elimination, mainly through hepatic, renal and biliary routes Rates • First Order: catalysed by enzymes, rate of metabolism directly proportional to drug concentration • Zero Order: enzymes saturated by high drug doses, rate of metabolism is constant, e. g. ethanol, phenytoin Phase • 1 = polarise lipophilic drugs, reduction / oxidation / hydrolysis, catalysed by cytochrome P 450 system • 2 = conjugation, e. g. glucuronic acid, polarisation of drugs to be excreted by renal or biliary systems
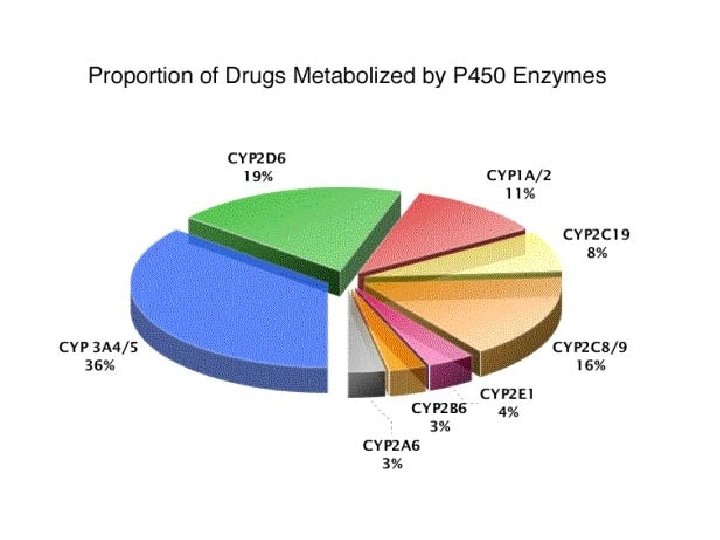

Cytochrome P 450 Inducers Inhibitors Anti-epileptics: phenytoin, carbamazepine Abx: ciproflaxacin, erythromycin Rifampicin Isoniazid St Johns Wort Amiodarone Chronic Alcohol intake Allopurinol Smokers (CYP 1 A 2) Anti-fungal: ketoconazole, fluconazole SSRI: fluoxetine, sertraline Sodium Valproate Acute Alcohol
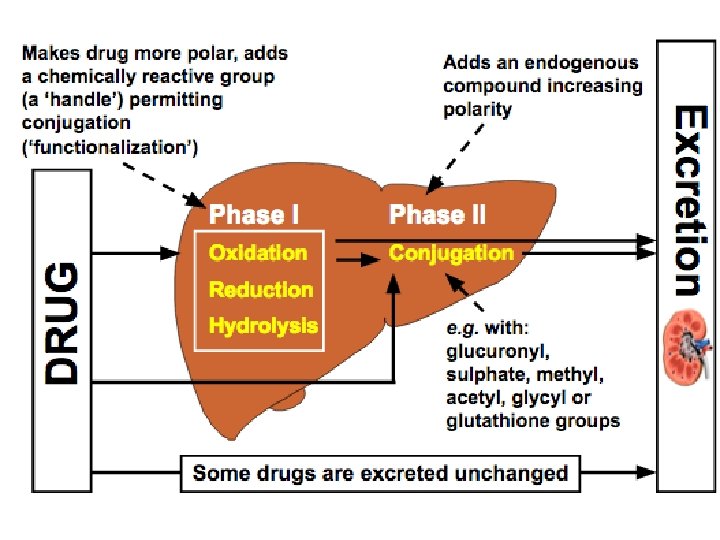

4. Elimination Renal • Excretion via urine • Must be sufficiently polar (role of phase 2) • Renal dysfunction = drug accumulation Other Routes • Intestines (faecal) • Bile • Lungs • Breast milk

Pharmacodynamics Definition • What the drug does to the body • It’s effect on cellular receptors via signal transduction Signal Transduction • Binding of drug to extracellular or intracellular receptor • Via a variety of receptors: ligand-gated ion channels, G protein-coupled receptors etc… • Leads to amplification or down -regulation of signals Intrinsic Effect • Agonist: full (equivalent to endogenous agonist), partial • Antagonist: competitive (reversibly prevents endogenous agonist binding), irreversible (covalent bond), allosteric (binds to other site, irreversible)

Dose-Response Relationship Factors of Drug Effect • Drug concentration (dose of drug + pharmacokinetic profile) • Receptor availability (maximal effect once receptors are saturated, irrelevant of increasing dose)

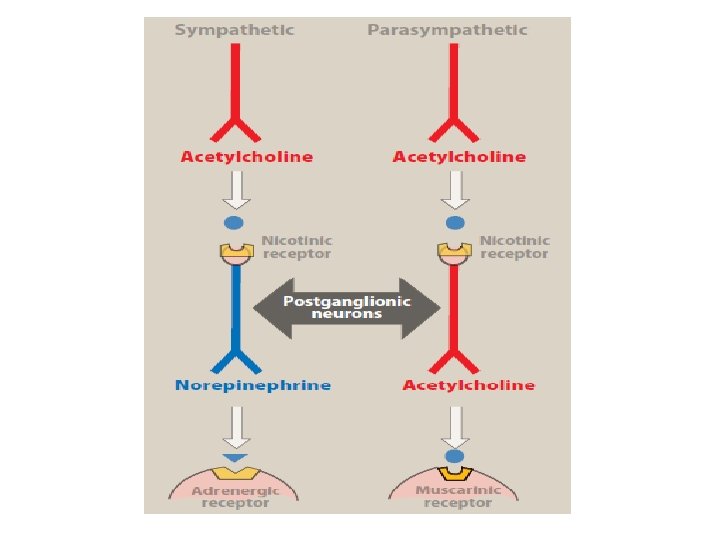
Autonomic Nervous System
 • Tamsulosin • Doxazosin Alpha-2")
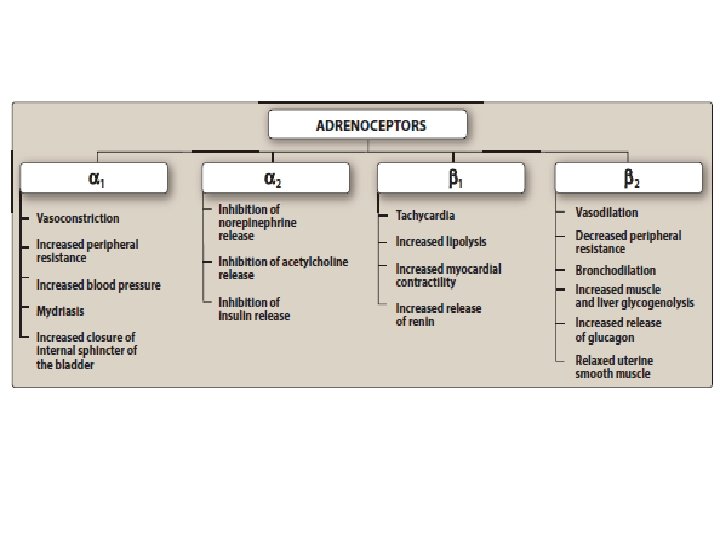
Sympathetic Adrenergic Receptors Agonist Antagonist Alpha-1 • Decongestants (phenylephrine) • Tamsulosin • Doxazosin Alpha-2 glaucoma Beta-1 • Inotropes (epinephrine, dopamine, dobutamine) • Selective/Nonselective betablockers Beta-2 • SABA/LABA • Non-selective betablockers Indirect • Cocaine • Amphetamine
 •")
Parasympathetic Muscarinic Receptor Agonist glaucoma Antagonist • Atropine • SAMA/LAMA • Oxybutynin (indirect) • Donepezil, Galantamine • Rivastigmine, Pyridostigmine, (indirect) Neostigmine • Rocuronium, Vecuronium

CNS Receptors Dopamine GABA Histamine-1 Histamine-2 Agonist • Ropinirole, Bromocriptine Antagonist • Anti-psychotics • Metoclopramide, Domperidone • Benzodiazepine • Loratidine, Cetirizine • Ranitidine

Antibiotics

Common Infections and Abx CAP • Amoxicillin +/Clarithromycin Atypical CAP • Clarithromycin IECOPD • Amoxicillin / Clarithromycin / Doxycline HAP • Co-Amoxiclav / Cefuroxime / Tazocin TB • RIPE Cellulitis • Flucloxacillin UTI • Trimethoprim / Nitrofurantoin Acute Pyelonephritis • Co-Amoxiclav / Ciprofloxacin
 + Azithromycin (PO) Chlamydia • Doxycycline")
Common Infections and Abx Gonorrhoea • Ceftriaxone (IM) + Azithromycin (PO) Chlamydia • Doxycycline / Azithromycin (PO) Syphilis • Benzathine benzylpenicillin Gastroenteritis • (Campylobacter) Clarithromycin • (Salmonella/Shigella) Ciprofloxacin C. Difficile • 1 st: Metronidazole • 2 nd: Vancomycin Acute Abdominal Infections (e. g. appendicitis) • Cef + Met

Cardiovascular - NSAID • NSAID = non-selective competitive reversible COX inhibition • Aspirin = irreversible COX (1>2) inhibition

Cardiovascular - Anti-platelet

Cardiovascular – Anti-coagulants
, short half-life.")
Cardiovascular – Anti-coagulants Heparin • Activates Antithrombin (decreased thrombin and factor Xa), short half-life. • LMWH (dalteparin): activates antithrombin (decreased factor Xa) and have longer half-life • Increased APPT, Monitor using anti-factor Xa assay • SE: Bleeding, thrombocytopenia (heparininduced thrombocytopenia), osteoporosis Warfarin • Anti-Vitamin K = Decreased FII (prothrombin)/VII/IX/X and Protein C/S • Increased PT/INR • SE: Bleeding, Skin/Tissue Necrosis, Teratogenic • Reversal = Vitamin K Direct Factor Xa Inhibitors • e. g. Apixaban, Rivaroxaban • Directly inhibit FXa • SE: Bleeding (no reversal agent) Thrombolytics • e. g. Alteplase/Tenecteplase (t. PA), Streptokinase • Activate Plasminogen -> Plasmin, Increased PT/APPT • SE: Bleeding

Cardiovascular - RAAS

Cardiovascular - RAAS JG cells release renin in response to: • Decrease BP detected by baroreceptors in afferent vascular walls • Decrease Na+ delivery to macula densa cells • Increase sympathetic stimulation (Beta-1) ACE functions: • Catalyses conversion of angiotensin I to angiotensin II • Degraded by bradykinin Angiotensin II effects: • Systemic arteriole vasoconstriction • Kidney efferent>afferent constriction = Increase Glomerular Pressure = Maintain GFR despite lowered overall kidney blood flow • Kidney proximal tubule/thick ascending limb Na+/H+ exchanger stimulation = Increased Na+/HCO 3/H 20 reabsorption • Adrenal cortex = Aldosterone release • Posterior Pituitary = ADH release

Cardiovascular - Diuretics
 • Inhibit Na/K/Cl cotransporter of thick ascending")
Cardiovascular - Diuretics Loop Diuretics (furosemide, bumetanide) • Inhibit Na/K/Cl cotransporter of thick ascending limb • IND: Oedematous States (HF, Cirrhosis, Nephrotic Syndrome, Pulmonary Oedema), HTN, Hypercalcaemia • SE: ototoxicity, hypokalaemia, dehydration, AKI, gout Thiazide Diuretics (bendroflumethiazide) • Inhibit Na/Cl cotransporter of distal tubule • IND: HTN, HF, Nephrogenic DI • SE: hypokalaemic metabolic alkalosis, hyponatraemia, hyperglycaemia, hypercalcaemia, hyperuricaemia Spironolactone • Spironolactone = competitive aldosterone receptor antagonists in collecting tubules • IND: HF, Hyperaldosteronism, Hypokalaemia • SE: hyperkalaemia, antiandrogen effects, e. g. gynaecomastia, loss of libido, erectile dysfunction

Endocrine System - Corticosteroids

Endocrine System - Corticosteroids

Endocrine System - Corticosteroids

Endocrine System Immunosuppressants

Endocrine System - T 2 DM

Endocrine System – T 2 DM Class Example Mechanism SE Biguanide Metformin • Increase insulin sensitivity • Decrease hepatic gluconeogenesis • GI disturbance • Lactic acidosis Sulphonylurea Gliclazide • Increase insulin secretion • Hypoglycaemia • Weight gain • SIADH Gliptin (DPP-4 inhibitor) Sitagliptine • Decrease glucagon secretion Thiazolidinediones Pioglitazone • Increase adipogenesis • Weight gain • Fluid retention • CI: HF, bladder Ca, hepatic impairment

Poisoning – Drug Monitoring Drug Parameters Details Statins LFT Baseline, 3 m, 12 m ACEi U&E Baseline, Annually Amiodarone CXR, LFT, TFT Baseline, every 6 m (not CXR) Methotrexate CXR, FBC, LFT, U&E Baseline, every 2 -3 m (not CXR) Azathioprine FBC, LFT Baseline, every 3 m Sodium Valproate LFT Baseline, 6 m Pioglitazone LFT Baseline

Poisoning - Therapeutic Ratio Narrow • Increased risk of toxicity, decreased chance of effective dose e. g. • Digoxin • Theophylline • Lithium • Phenytoin • Gentamicin, Vancomycin

Poisoning - Overdose Management <1 hr following ingestion • PO Activated Charcoal Digoxin • Digoxin-specific antibody fragments Salicylate (aspirin) • Haemodialysis Carbon Monoxide • 100% Oxygen Opiate/Opioid • Naloxone Organophosphate Insecticides • Atropine

Poisoning – Paracetamol Overdose Pathology • Phase 2 conjugation pathway saturated • Alternative pathway used = NAPQI = glutathione depletion • Glutathione depletion = liver/renal necrosis Risk Factors • Psychiatric Hx • Elderly, Low weight • P 450 inducers Investigation • Serum paracetamol level • U&E, LFT, Glucose, Clotting, ABG Management • IV N-acetylcysteine - On/above nomogram line - Staggered overdose - Doubt over ingestion time • Liver transplant

Poisoning – Paracetamol Overdose

Poisoning – Paracetamol Overdose

- Slides: 46