GENITOURINARY SYSTEM Michelle Gardner NUR224 URINARY SYSTEM ASSESSMENT









 X- ray exam of abdomen")
 Urography Intravenous injection of radiopaque imaging")






















 Risk factors n Hypercalciuria/hypercalcemia, immobility, vit. D, urine intoxication, dehydration Management")



 15 -20 % of stones magnesium/ammonium/phosphate Risk Factors n UTIs, esp")









 § • § § § Age–related, nonmalignant enlargement of the")





 § Cardura - (doxazosin) § Hytrin – (terazosin)")


 § Low-wave radio frequency – to burn away")

 § Removal of inner prostate tissue §")











 Check stoma color– beefy red")














 n Chemotherapy/Radiation n")
 n Chemotherapy/Radiation n")
- Slides: 99
GENITOURINARY SYSTEM Michelle Gardner NUR-224
URINARY SYSTEM
ASSESSMENT OF THE URINARY SYSTEM Subjective Data a. Good communication skills b. Avoid medical terminology c. Anxiety/embarrassment – “forget/deny”--
ASSESSMENT DATA Past Health History a. Presence/history of diseases r/t urologic problems – DM, HTN b. Neurologic conditions – back injury, stroke, trauma c. Urinary problems – BPH, renal calculi, cancer, infection
ASSESSMENT DATA Medications a. b. c. d. Prescription / OTC / Herbs Nephrotoxic medications -- antibiotics Quantity & character of urine output – diuretic, anticholinergic, antihistamine Change in color – Pyridium, Macrodantin
ASSESSMENT DATA Surgery a. Previous hospitalizations r/t urologic disease b. Pelvic surgeries c. Urinary instrumentation d. Urinary problems during past pregnancies e. Radiation/chemotherapy
ASSESSMENT DATA n n n Pain Changes in voiding Affects of aging on the urinary system a. Decrease muscle tone b. Decrease bladder capacity c. Prostate enlargement d. Changes in metabolism
BLOOD CHEMISTRIES Blood Chemistries n Serum Creatinine: 0. 6 – 1. 2 mg/dl o End product of muscle & protein metabolism o Excellent indicator of kidney function o Renal disease results in increase creatinine
BLOOD CHEMISTRIES n o o BUN/Blood Urea Nitrogen: 7 -18 mg/dl Used to identify renal problems Nonrenal factors may increase BUN a. Fever b. Dehydration c. High protein diet d. Athletic activity e. Drugs and vitamins (acetaminophen, ibuprofen, vitamin D)
DIAGNOSTIC STUDIES n o o KUB (kidneys, ureters, bladder) X- ray exam of abdomen & pelvis Used to detect abnormalities o o Urinary calculi Cysts Tumors Hydronephrosis
DIAGNOSTIC STUDIES n o o IVP (INTRAVENOUS PYLEOGRAM) Urography Intravenous injection of radiopaque imaging dye X-ray imaging of dye through upper and lower urinary system
INTRAVENOUS UROGRAPHY
INTRAVENOUS UROGRAPHY n o o o Patient preparation: Consent form Cathartic/enema the night before Identify allergies – shellfish, iodine Pre-medicate–antihistamine (Benadryl) NPO 8 hr. before procedure Transitory effects – contrast medium
INTRAVENOUS UROGRAPHY n o o Post-procedure Monitor vital signs Assess for s/s anaphylactic reactions Monitor urine output Force fluids
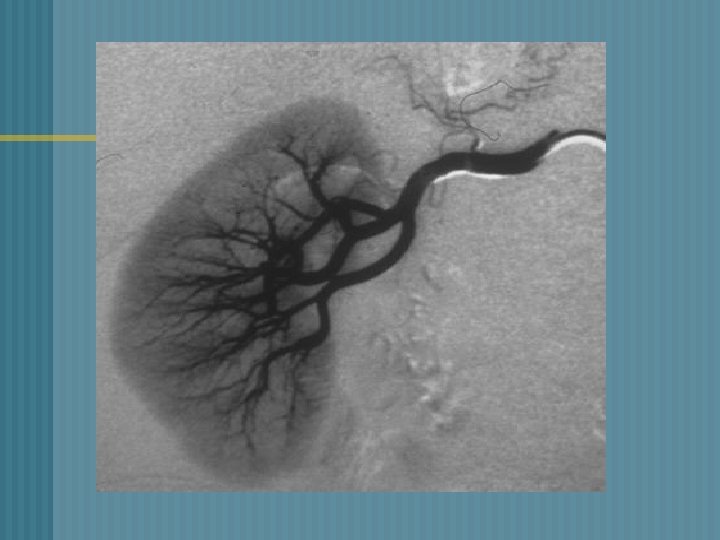
RENAL ANGIOGRAPHY n o o o § 1. 2. 3. RENAL ANGIOGRAM: Catheter inserted into femoral artery Contrast material injected through the catheter Visualize renal blood vessels Findings : Renal artery stenosis Differentiate renal cysts from tumors Evaluate hypertension
RENAL ANGIOGRAPHY n o o Patient preparation Consent form Cathartic/enema the evening before Assess allergic reaction Mark peripheral pulses
RENAL ANGIOGRAPHY n o o o Post-Procedure Monitor vital signs Pressure dressing over insertion site Assess insertion site Bedrest with affected leg straight Palpate peripheral pulses
RENAL BIOPSY n o o Done as a needle biopsy with needle insertion into lower lobe of the kidney OR open biopsy via small flank incision Obtain renal tissue to determine type of renal disease Kidneys are vascular organs – hemorrhage/complication
RENAL BIOPSY Patient preparation o Consent form signed o NPO status 8 hrs. prior to test o Assess baseline coagulation status o Medications that may alter clotting function
RENAL BIOPSY
RENAL BIOPSY Post-Procedure o Pressure dressing applied o Check puncture site – swelling/tenderness o Prone position for 30 -60 minutes o Monitor vital signs o Observe for gross bleeding o Assess for flank pain, Hgb. /Hct. levels o Avoid lifting heavy object/strenuous activity – 7 days
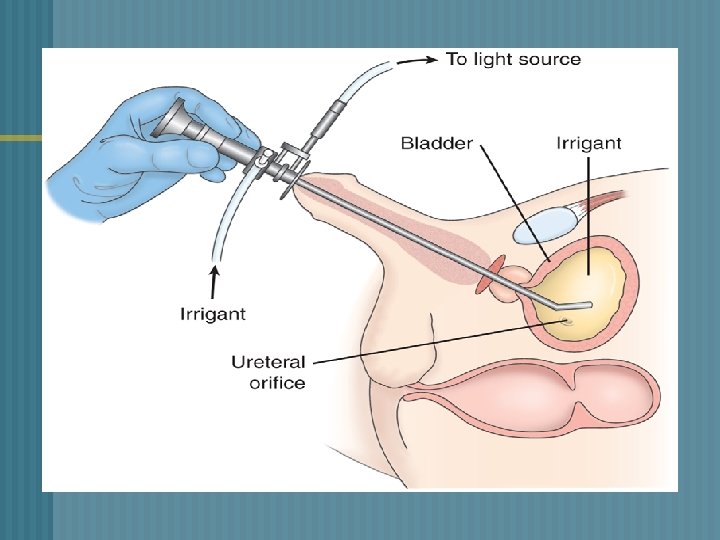
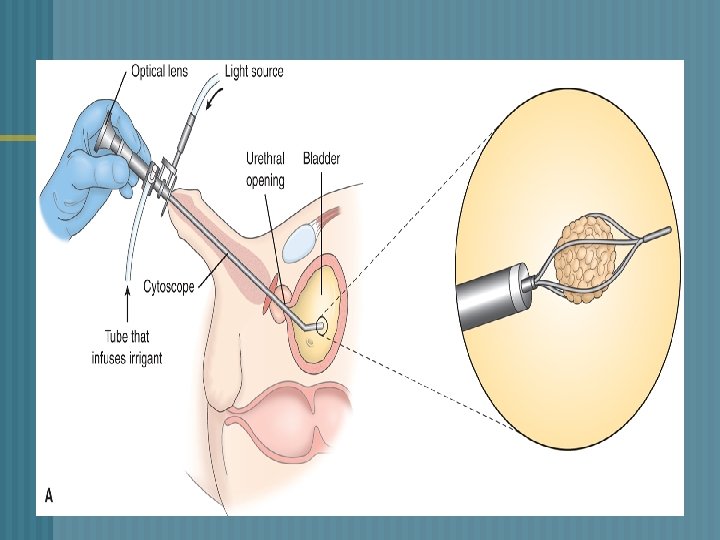
UROLOGIC ENDOSCOPIC PROCEDURES o o a. b. c. d. Visualize/inspect the interior of the urethra and bladder with a tubular lighted scope (cystoscope) Used to: Treat bleeding lesions Insert ureteral catheters Remove calculi Obtain biopsy specimens
CYSTOSCOPY n o o Patient preparation Signed consent form NPO prior to the procedure Local topical anesthetic Lithotomy position – leg cramps
CYSTOSCOPY n o o Post-procedure Expected side effects - burning on urination, blood-tinged urine, urinary frequency Encourage increased fluids Warm sitz bath Mild analgesics
RENAL CALCULI
UROLITHIASIS/ NEPHROLITHIASIS n n n 500, 000 people in the U. S. have kidney stone disease Incidence is highest in Southern & Midwest states. Occurs between the 3 rd-5 th decade of life. Recurrence of stones – 50% of pts. More common in men than in women
RENAL CALCULI Risk Factors n n n Family history of stone formation Dehydration increase urine concentrations Excess dietary intake of calcium, oxalate, or proteins Sedentary lifestyle/immobility Genetic predisposition
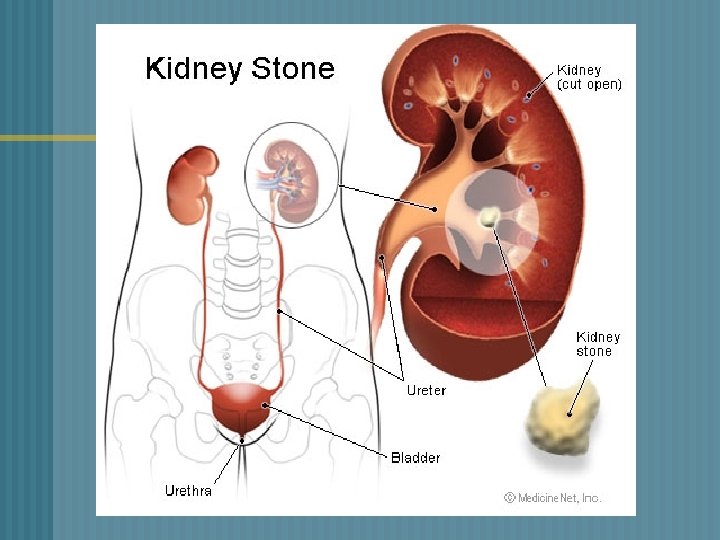
RENAL CALCULI o o o Stones can be found anywhere from kidney to bladder Vary in size Factors that contribute to urolithiasis * supersaturation * nucleation
RENAL CALCULI Pathophysiology n Concentration of an insoluble salt is high in the urine supersaturation n Crystals form from supersaturated urine n Growth continues by aggregation to form larger particles – stone formation
RENAL CALCULI
RENAL CALCULI n 1. 2. 3. 4. 4 Major Categories of Stones Calcium Oxalate Uric acid Cystine
Calcium Calculi n n High concentration of calcium in the blood/urine 70 -80% of kidney stones are calcium stones Smaller stones maybe trapped in the ureter Seen more in men
Calcium Calculi (Oxalate) Risk factors n Hypercalciuria/hypercalcemia, immobility, vit. D, urine intoxication, dehydration Management n Thiazide diuretics n Limit foods that acidify urine n Hydration/exercise
Uric Acid Stones
Uric Acid Calculi Urine concentration of uric acid is high o Common in men Causes: 1. Gout 2. Increased dietary intake of purine 3. Acid urine o 1. 2. 3. Reduce dietary purines– sardines, mussels, organ meats, aged cheese Administer allopurinol (Zyloprim) Reduce urinary concentration of uric acid
Struvite Calculi
Struvite Calculi (Staghorn) 15 -20 % of stones magnesium/ammonium/phosphate Risk Factors n UTIs, esp Proteus infections n Stones are large fill renal pelvis Management n Antibiotics n Surgical intervention/lithotripsy n
Cystine Calculi o o o Make up 1 -2% of all stones Caused by genetic defect Tend to form in acid urine Stones appear during childhood / adolescence Rare in adults o o Increase hydration Low-protein diet
RENAL CALCULI n o o o Clinical Manifestations: Severe flank pain / renal colic Abdominal pain Hematuria Oliguria/anuria Nausea /Vomiting/Diarrhea
RENAL CALCULI Diagnostic Studies: o Urinalysis o 24 hr urinary measurement for calcium, uric acid o X-ray - KUB o Renal Ultrasonography o CT Scan
RENAL CALCULI Management Pain management o Opiod analgesics – Morphine o NSAID Toradal o Comfort measures o Increase fluid intake (oral/intravenous)
RENAL CALCULI Stones may pass spontaneously § Stones larger than 4 mm are unlikely to pass through the ureter § Chemical analysis of the stone to determine the composition of the stone v STRAIN ALL URINE §
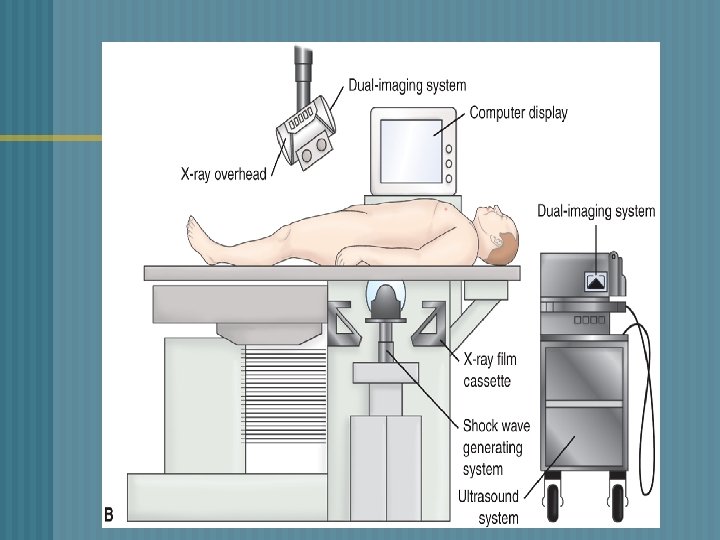
RENAL CALCULI q § o o o o THERAPUETIC INTERVENTIONS ESWL-Extracorporeal shock-wave lithotripsy Non-invasive procedure External shock-waves break up the stone No damage to surrounding tissue Stones are fragmented into fine sand Fragments are excreted in the urine All urine is strained -- chemical analysis Anesthesia is necessary
RENAL CALCULI o o o Cystoscopy passed – removes stones located in the ureter close to the bladder Stone removed -- grasping basket, forceps Stent may be placed Foley catheter -- facilitate passage stone fragments Minimal complications
RENAL CALCULI After episode of urolithiasis a. Increase fluid intake – 3000 ml/day b. High urine output – 2 L/day c. Water is the preferred fluid d. Avoid tea, coffee, colas e. Limit foods high in oxalate, calcium, & purines STRAIN ALL URINE q
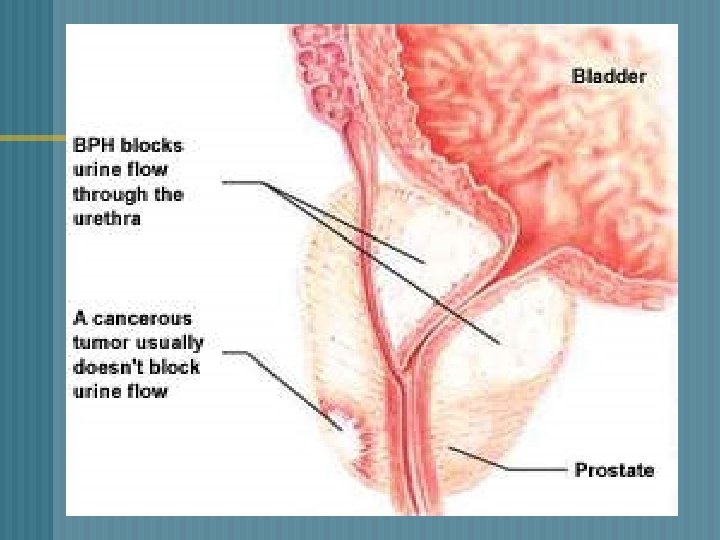
BENIGN PROSTATIC HYPERPLASIA (BPH) § • § § § Age–related, nonmalignant enlargement of the prostate gland Enlargement of the prostate gland -compress the urethra/bladder This impedes the normal flow of urine Begins at the age of 40 and continues slowly throughout the rest of life Symptoms appear slightly earlier in Afro. American men
BPH Begins with small layers in the periuretheral gland n Prostate enlarges through formation /growth of nodules and enlargement of glandular cells n Enlargement compresses against the urethra urologic symptoms n Changes occur over a long period of time n
BPH Clinical Manifestations § Difficulty starting urinary stream § Urinary frequency § Nocturia § Leakage or dribbling of urine § Urgency
BPH Complications § Urinary retention § Urinary tract infections § Bladder stones
BPH Diagnostic Studies § History & physical exam § Urinalysis/ C&S § Digital rectal exam (DRE) § Prostatic Specific Antigen(PSA) -- R/O Prostate Cancer § Serum Creatinine
MEDICATION THERAPY ALPHA-ADRENERGIC BLOCKERS § • • Relax the smooth muscle of the bladder neck and prostate Improves urine flow Relax smooth muscle of the prostate
BPH ALPHA-ADRENERGIC BLOCKERS § Flomax- (tamsulosin) § Cardura - (doxazosin) § Hytrin – (terazosin) § Uroxatral – (alfuzosin) Side effect § § orthostatic hypotension dizziness
BPH 5 ALPHA-REDUCTASE INHIBITORS § Decreases the size of the prostate gland § Proscar (finasteride) § Avodart – (dutasteride) n Side effect *decreases libido, *erectile dysfunction
BPH Minimally Invasive Therapy § § § used when medication not effective relieves the manifestations of BPH less invasive than traditional surgery
BPH v Transuretheral Needle Ablation (TUNA) § Low-wave radio frequency – to burn away a region of the enlarged prostate Improves the flow of urine 70% of pt. show marked improvement Little pain Early return to regular activities § §
TUNA
BPH Transuretheral Resection of the Prostate (TURP) § Removal of inner prostate tissue § Most common procedure Advantages 1. No external incision made 2. Shorter hospitalization 3. Complications – clot retention, hemorrhage, infection, catheter obstruction
TURP
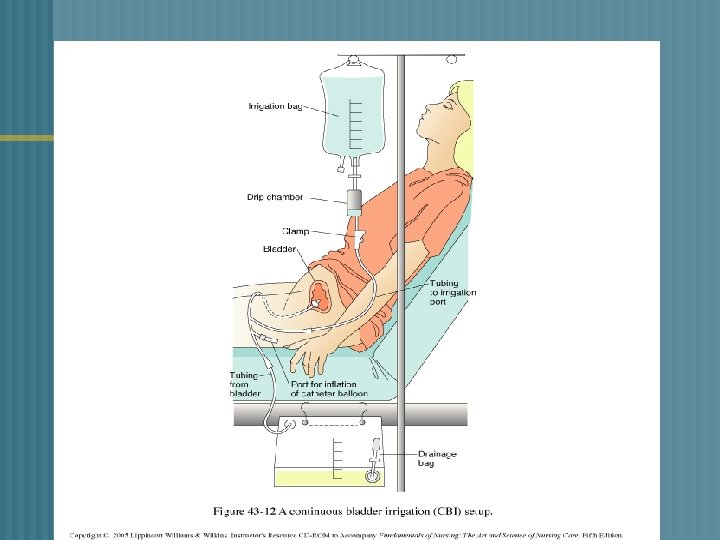
CONTINOUS BLADDER IRRIGATION n n n 3 - way drainage system- useful in irrigating the bladder & preventing clot formation 3000 ml sterile normal saline Irrigation -- consist of continuous inflow & outflow of solution & drainage Maintain patency of catheter & tubing Urine drainage – light pink Blood clots are expected 1 st 24 -36 hrs. after surgery
CBI Catheter removal – n assess amount, color and consistency of urine n may experience burning on urination, dribbling is common
BPH Complications n Hemorrhage n Obstructed catheter n Urinary incontinence
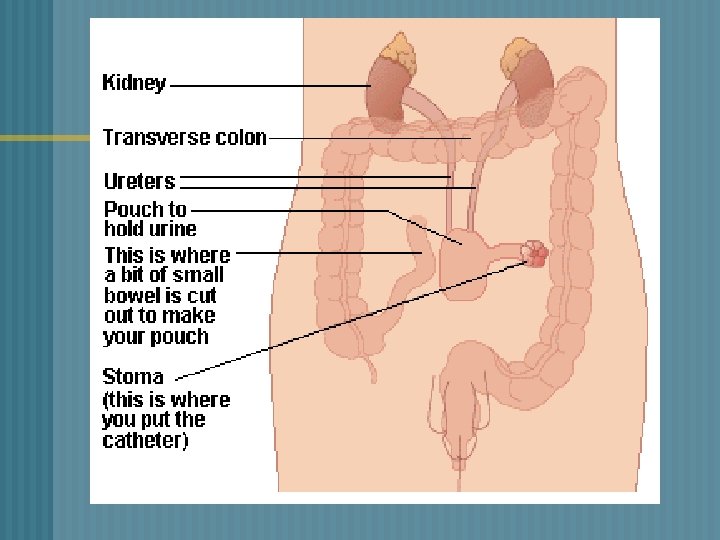
URINARY DIVERSIONS ¬ Procedure performed to divert urine from the bladder to a new exit site – STOMA ¬ Used to treat a. Cancer of the bladder b. Congenital anomalies c. Trauma to the bladder d. Neurogenic bladder
URINARY DIVERSIONS n 1. 2. 2 CATERGORIES Incontinent urinary diversion Continent urinary diversion
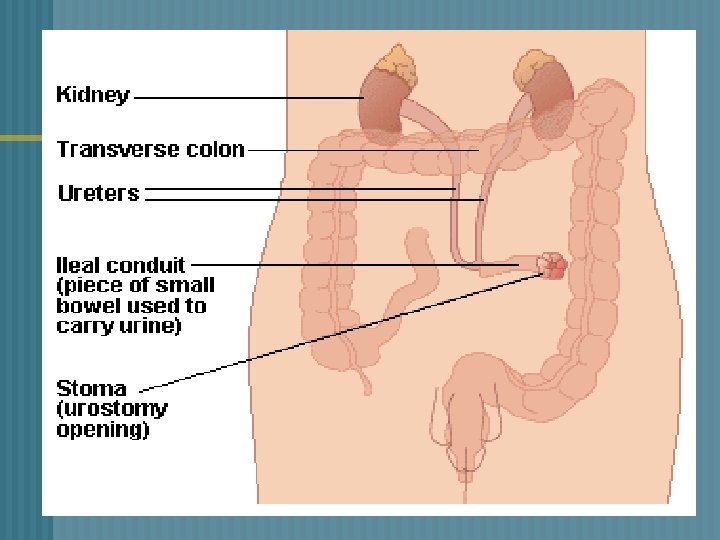
URINARY DIVERSIONS ¬ INCONTINENT • • • DIVERSION Urine drains through an opening created in the abdominal wall An appliance is needed Most common – Ileal Conduit
URINARY DIVERSIONS ¬ INCONTINENT • • DIVERSIONS – ileal conduit Ureters are excised from the bladder & resected to a part of the ileum Proximal end is sewn closed Distal end created to form a stoma Remaining intestinal segments – anatomosed
URINARY DIVERSIONS ¬ INCONTINENT DIVERSIONS • Stents -- prevent occlusion from post-surgical edema Disadvantages: • Requires a external collection device • Visible stoma
URINARY DIVERSIONS INCONTINENT DIVERSIONS Pre-op Management • Discuss social aspects of living with a stoma 1. Clothing 2. Changes in body image 3. Odor 4. Sexuality 5. Exercise ¬
URINARY DIVERSIONS INCONTINENT DIVERSIONS Post-op Management • Assess for complications a. Paralytic ileus/SBO • Make sure urinary stents are draining • U/O < 30 cc/hr – dehydration/obstruction • Hematuria – 1 st 24 -48 hours • Mucous threads in urine – normal occurrence ¬
URINARY DIVERSIONS ¬ Post-op • • • management (cont’d) Check stoma color– beefy red Increase fld. intake Empty pouch when 1/3 full/q 2 -3 hr. Meticulous skin care Avoid foods that give strong odor– cheese, eggs, asparagus
URINARY DIVERSIONS ¬ CONTINENT • • • DIVERSIONS Intra-abdominal urinary reservoir Self catheterize every 4 -6 hours No need external attachments Reservoirs constructed from different parts of the ileum/colon Kock, Indiana, Charleston pouch
URINARY DIVERSION ¬ CONTINENT DIVERSIONS Post-op Management • Teach patient to catheterize pouch • Irrigate pouch • Adhere to strict catheterization schedule • Enterostomal therapy nurse
QUESTION A patient returns to the unit following a TURP. His urinary drainage bag is filled with dark red fluid with obvious bloods clots. And he is having bladder spasms. What would you do first? a. Assess his intake/output since surgery b. Administer pain medication as ordered c. Report your assessment to the urologist d. Nothing, these are manifestations that are expected following a TURP
QUESTION n a. b. c. d. The nurse evaluates her teaching as effective when a patient with a newly continent ileal diversion is able to do which of the following? Demonstrate care for the collection device State the importance of reporting cloudy urine to the physician Demonstrate self-catherization of the stoma Identify factors that contribute to this
Urinary Tract Cancers Prostate Cancer of the Bladder
Cancer of the Prostate Most common cancer among men after skin cancer n Highest incidence in African. American men n Risk Factors n increases rapidly after age 50 n Family history n High intake of red meat and high fat dairy products n
Cancer of the Prostate Signs and Symptoms Often asymptomatic n As malignancy enlarges, may have symptoms of urinary obstruction n Blood in urine, semen and painful ejaculation may occur n C/O back and hip pain, weight loss, anemia, oliguria may indicate metastases n
Cancer of the Prostate Assessment and Diagnosis Screening tools n DRE n PSA n n Normal: 0 -4 ng/m. L Transrectal Ultrasound (TRUS) n Biopsy n
Cancer of the Prostate Treatment n n Surgical removal of the prostate n TURP n Laproscopic radical prostatectomy Radiation n Teletherapy n Brachytherapy Hormone Therapy n Casodex n DES Chemotherapy
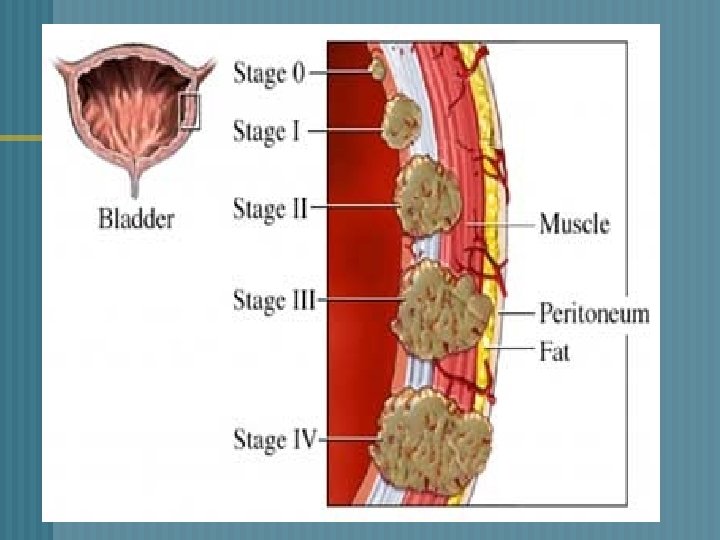
Cancer of the Bladder n Most commonly seen in ages 50 -70 Transitional-cell carcinoma of the bladder n Papilillomatous growths in the bladder n n Risk factors Cigarette smoking (twice as much) n Environmental carcinogens n Frequent/recurrent bacterial infections n History of urogenital cancers n
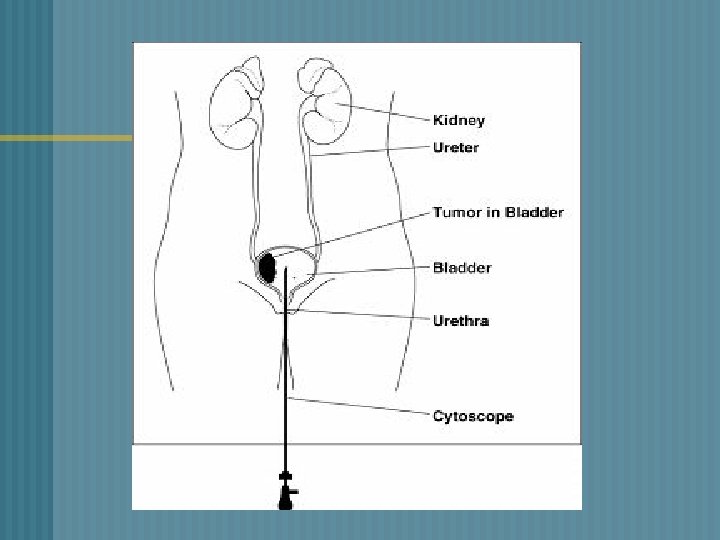
Cancer of the Bladder Assessment and Diagnosis Hematuria n Bladder irritability n Pelvic or back pain n Diagnostic tests: n Cystoscopy n Ultrasound/CT n Biopsies n
Cancer of the Bladder Treatment Transurethral Resection of Bladder Tumor (TURBT) n Chemotherapy/Radiation n BCG n Methotrexate/5 -FU/ vinblastin/Adriamycin n n Cystectomy
Cancer of the Bladder Treatment Transurethral Resection of Bladder Tumor (TURBT) n Chemotherapy/Radiation n BCG n Methotrexate/5 -FU/ vinblastin/Adriamycin/cisplatin n n Cystectomy Partial n Radical n