FEMORAL SHAFT FRACTURE IN ADULTS Students presentation seminars




")












 classification reflects the observation that the degrees of")



 and lateral views are usually adequate in demonstrating the")






 fractures in children; (2) contraindications to anaesthesia; and")
 require skeletal")

 traction")


 fractures at either end of")






 treatment of")

")






























- Slides: 81
FEMORAL SHAFT FRACTURE IN ADULTS Students presentation seminars in orthopedic trauma Badr D. badr Zainab K. mete’eb
Normal anatomy • The skeletal support for the thigh is the femur. The femur is the largest tubular bone in the body.
• A. The shaft of femur is bowed forward. • B. Has an oblique course from the neck of the femur to the distal end. As a consequence of this oblique orientation, the knee is close to the midline under the body's center of gravity. The medial cortex is under compression, whereas the lateral cortex is under tension. • C. The middle part of the shaft of femur is triangular in cross-section and has smooth medial (posteromedial), lateral (posterolateral), and anterior surfaces and medial, lateral, and posterior borders. The medial and lateral borders are rounded whereas the posterior border forms a broad roughened crest-the linea aspera. At the distal end of the femur, this posterior surface forms the floor of the popliteal fossa and its margins, which are continuous with the linea aspera above, form medial and lateral supracondylar lines. The medial supracondylar lines terminate at a prominent tubercle (the adductor tubercle) on the superior aspect of the medial condyle of the distal end. The distal end of femur is characterized by two large condyles, which articulate with the proximal head of the tibia. • The condyles are separated posteriorly by an intercondylar fossa and are joined anteriorly where they articulate with the patella.
The thigh musculature • It is divided into three distinct fascial compartments. From: Grant's Atlas of Anatomy (13 th Ed)
From: Grant's Atlas of Anatomy (13 th Ed)
• The anterior compartment of thigh contains the sartorius and the four large quadriceps femoris muscles (rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius). All are innervated by the femoral nerve. In addition, the terminal ends of the psoas major and iliacus muscles pass into the upper part of the anterior compartment from sites of origin on the posterior abdominal wall. These muscles are innervated by branches directly from the anterior rami of L 1 to L 3 (psoas major) or from the femoral nerve (iliacus) as it passes down the abdominal wall. • The medial compartment of thigh contains six muscles (gracilis, pectineus, adductor longus, adductor brevis, adductor magnus, and obturator externus). All except pectineus, which is innervated by the femoral nerve, and part of the adductor magnus, which is innervated by the sciatic nerve, are innervated by the obturator nerve. • Posterior compartment: This includes the biceps femoris, semitendinosus, and semimembranosus, termed the 'hamstrings'. All are innervated by the sciatic nerve.
The clinical lesson 1 The bone is surrounded by the largest mass of muscle. This provides advantages and disadvantages: 1. The femur is relatively protected from injuries, 2. Healing potential is improved by having this well- vascularized sleeve containing a source of mesenchymal stem cells, 3. And open fractures often need no more than split thickness skin grafts to obtain satisfactory cover. 4. Reduction can be difficult as muscle contraction displaces the fracture
The clinical lesson 2 The femoral shaft is subjected to major muscular deforming forces A. B. C. D. E. Abductors (gluteus medius and minimus): They insert on the greater trochanter and abduct the proximal femur following subtrochanteric and proximal shaft fractures. Iliopsoas: It flexes and externally rotates the proximal fragment by its attachment to the lesser trochanter. Adductors: They span most shaft fractures and exert a strong axial and varus load to the bone by traction on the distal fragment. Gastrocnemius: It acts on distal shaft fractures and supracondylar fractures by flexing the distal fragment. Fascia lata: It acts as a tension band by resisting the medial angulating forces of the adductors.
The vascular supply to the femoral shaft • It is derived mainly from the profunda femoral artery. The one to two nutrient vessels usually enter the bone proximally and posteriorly along the linea aspera. This artery then arborizes proximally and distally to provide the endosteal circulation to the shaft. The endosteal vessels supply the inner two-thirds of the cortex. The periosteal vessels also enter the bone along the linea aspera and supply blood to the outer one-third of the cortex.
Deep artery of thigh. A. Anterior view. B. Posterior view.
The clinical lesson 3 • Potential sites of vascular injury after fracture at the adductor hiatus and the perforating vessels of the profunda femoris. • Femoral shaft fractures heal readily if the blood supply is not excessively compromised. Therefore, it is important to avoid excessive periosteal stripping, especially posteriorly, where the arteries enter the bone at the linea aspera. • Reaming may further obliterate the endosteal circulation, but it returns fairly rapidly, in 3 to 4 weeks.
Femoral Shaft fracture in adults • A femoral shaft fracture is a fracture of the femoral diaphysis occurring between 5 cm distal to the lesser trochanter and 5 cm proximal to the adductor tubercle.
Epidemiology • Femoral shaft fractures occur most frequently in young men after high-energy trauma and elderly women after a low-energy fall.
Mechanism of injury • In adults they are almost always the result of high-energy trauma. These fractures result from motor vehicle accident, gunshot injury, or fall from a height. • Pathologic fractures, especially in the elderly, commonly occur at the relatively weak metaphyseal-diaphyseal junction. Any fracture that is inconsistent with the degree of trauma should arouse suspicion for pathologic fracture. • Stress fractures occur mainly in military recruits or runners. Most patients report a recent increase in training intensity just before the onset of thigh pain.
Fracture patterns are clues to the type of force that produced the break. • A spiral fracture is usually caused by a fall in which the foot is anchored while a twisting force is transmitted to the femur. Transverse and oblique fractures are more often due to angulation or direct violence and are therefore particularly common in road accidents. With severe violence (often a combination of direct and indirect forces) the fracture may be comminuted, or the bone may be broken in more than one place (a segmental fracture).
Pathological anatomy 1. Fracture displacement often follows a predictable pattern dictated by the pull of muscles attached to each fragment. 2. The soft tissues are always injured and bleeding from the perforators of the profunda femoris may be severe.
3. Femoral shaft fractures are classified into three types. • 1. Comminuted femoral shaft fractures • 2. Spiral, transverse, or oblique shaft fractures • 3. Open femoral shaft fractures • Most fractures of the femoral shaft have some degree of comminution, although it is not always apparent on x-ray. Comminuted fractures are further classified by Winquist based on the size of the fracture fragment and the degree of comminution.
Winquist’s (Winquist, Hansen et al. 1984) classification reflects the observation that the degrees of soft-tissue damage and fracture instability increase with increasing grades of comminution. In Type 1 there is only a tiny cortical fragment. In Type 2 the ‘butterfly fragment’ is larger but there is still at least 50 per cent cortical contact between the main fragments. In Type 3 the butterfly fragment involves more than 50 per cent of the bone width. Type 4 is essentially a segmental fracture.
Clinical features • The effects of blood loss and other injuries, some of which can be life-threatening, may dominate the clinical picture. • The patient will present with severe pain in the involved extremity. • They usually have visible deformities. • The thigh will be swollen and tense secondary to hemorrhage and formation of a hematoma. • The extremity may be shortened. • There may be crepitation with movement.
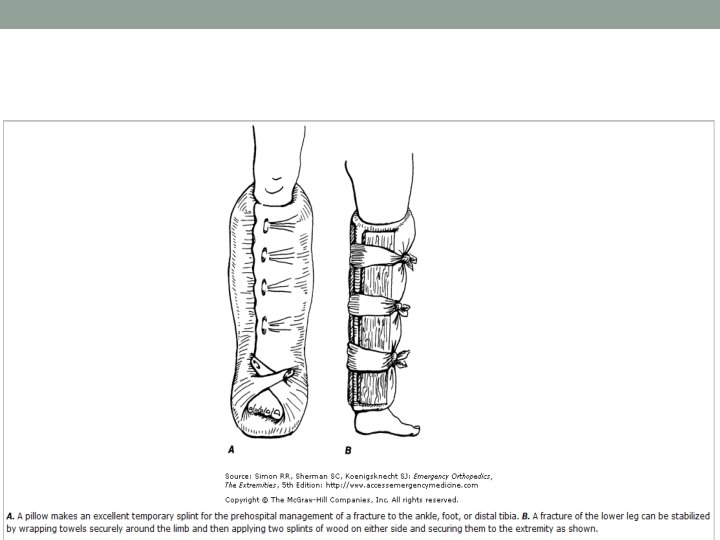
From: Emergency Orthopedics
• Neurologic examination should be performed to assess the function of the sciatic nerve. Arterial injuries are rare, but they must be excluded on the initial examination. Arterial injuries associated with a femoral shaft fracture should be suspected in the presence of: • Expanding hematoma • Absent or diminishing pulses • Paraesthesia or pallor in the leg and foot. • Careful clinical scrutiny is necessary to exclude other lower limb or pelvic fractures. • An ipsilateral femoral neck fracture occurs in about 10 per cent of cases and, if present, there is a one in three chance of a significant knee injury as well. • The combination of femoral shaft and tibial shaft fractures on the same side, producing a ‘floating knee’, signals a high risk of multi-system injury in the patient.
Imaging 1. Routine anteroposterior (AP) and lateral views are usually adequate in demonstrating the fracture. • Stress fractures of the femoral shaft may not be visualized on these routine views. • The fracture pattern should be noted; it will form a guide to treatment.
2. never forget to xray the hip and knee as well.
3. A baseline chest x-ray is useful as there is a risk of adult respiratory distress syndrome (ARDS) in those with multiple injuries.
Emergency treatment • Shock should be treated; blood volume is restored and maintained. • Traction with a splint is first aid for a patient with a femoral shaft fracture. If a sciatic nerve injury is associated, a plaster splint should be substituted for the traction splint to avoid further injury to the nerve. This temporary stabilization helps to control pain, reduces bleeding and makes transfer easier. • Pain medications should be provided early. • Admission for a definitive plan of action instituted as soon as the patient’s condition has been fully assessed.
Definitive treatment- principles • Operative stabilization is the standard of care for most femoral shaft fractures. • Surgical stabilization should occur within 24 hours, if possible. • Early stabilization of long bone injuries appears to be particularly important in the multiply injured patient. • The definitive treatment for femoral shaft fractures is closed intramedullary nailing.
The patient with multiple injuries • The association of femoral shaft fractures with other injuries, including head, chest, abdominal and pelvic trauma, increases the potential for developing fat embolism, ARDS and multi-organ failure. The risk of systemic complications can be significantly reduced by early stabilization of the fracture. • [Opinion 1] by a locked intramedullary nail. • [opinion 2 from Apley] prompt stabilization with an external fixator may be wise; the fixator can be exchanged for an intramedullary nail when the patient’s condition stabilizes.
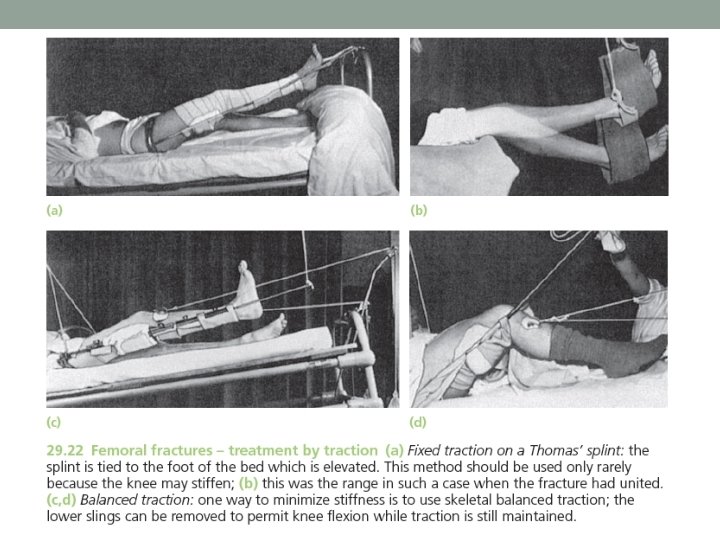
The isolated femoral shaft fracture Traction, bracing and spica casts • Traction can reduce and hold most fractures in reasonable alignment, except those in the upper third of the femur. Joint mobility can be ensured by active exercises. The chief drawback is the length of time spent in bed (10– 14 weeks for adults) with the attendant problems of keeping the femur aligned until sufficient callus has formed plus reducing patient morbidity and frustration. I.
The main indications for traction (1) fractures in children; (2) contraindications to anaesthesia; and (3) lack of suitable skill or facilities for internal fixation. • It is a poor choice for elderly patients, for pathological fractures and for those with multiple injuries.
The various methods of traction in adults • Adults (and older adolescents) require skeletal traction through a pin or a tightly strung Kirschner wire behind the tibial tubercle. Traction (8– 10 kg for an adult) is applied over pulleys at the foot of the bed. • The limb is usually supported on a Thomas’ splint and a flexion piece allows movement at the knee. However, a splint is not essential; indeed, skeletal traction without a splint (Perkins’ traction) has the advantages of producing less distortion of the fracture and allowing freer movement in bed. Exercises are begun as soon as possible.
Perkins’ traction
• Once the fracture is sticky (at about 8 weeks in adults) traction can be discontinued and the patient allowed up and partial weight-bearing in a cast or brace. For fractures in the upper half of the femur, a plaster spica is the safest but it will almost certainly prolong the period of knee stiffness. For fractures in the lower half of the femur, castbracing is suitable. This type of protection is needed until the fracture has consolidated (16– 24 weeks).
II. Plate and screw fixation • Plating is a comparatively easy way of obtaining accurate reduction and firm fixation. The method was popular at one time but went out of favour because of a high complication rate. This occurred when plates were applied through a wide open exposure of the fracture site and perfect anatomical reduction of all bone pieces. Such extensive surgery damaged the healing potential and led to tardy union and implant failure.
minimally invasive plate osteosynthesis • However, plates have encountered resurgence: today, they are inserted through short incisions and placed in a submuscular plane, rather than deep to periosteum; an indirect (closed) reduction of the fracture is done; fewer screws are used, and usually placed at the ends of the plate, leading to a less rigid hold on the fracture. This technique of minimally invasive plate osteosynthesis (MIPO) has led to better union rates. However, postoperative weightbearing will need to be modified as the implant is not as strong as an intramedullary nail.
• The main indications for plates are (1) fractures at either end of the femoral shaft, especially those with extensions into the supracondylar or pretrochanteric areas, (2) a shaft fracture in a growing child, and (3) a fracture with a vascular injury which requires repair. • Others: Handbook Of Fractures Koval 3 rd Ed • Extremely narrow medullary canal where IM nailing is impossible or difficult. • Obliteration of the medullary canal due to infection or previous closed management. • Fractures that occur adjacent to or through a previous malunion.
• Advantages to plating include: • Ability to obtain an anatomic reduction in appropriate fracture patterns. • Lack of additional trauma to remote locations such as the femoral neck, the acetabulum, and the distal femur.
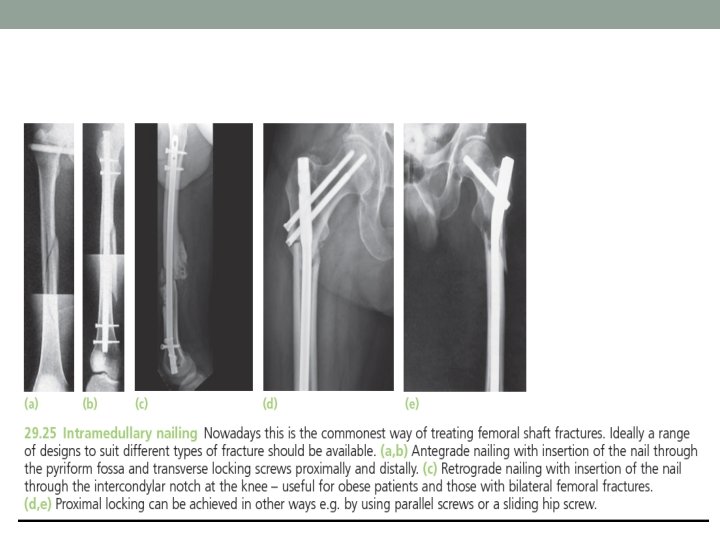
III. Intramedullary nailing • Intramedullary nailing, if appropriate facilities and expertise are available, is the method of choice for most femoral shaft fractures. • The basic implant system consists of an intramedullary nail (in a range of sizes) which is perforated near each end so that locking screws can be inserted transversely at the proximal and distal ends; this controls rotation and length, and ensures stability even for subtrochanteric and distal third fractures. • Often there is enough shared stability between the nail and fracture ends to allow some weight-bearing early on.
Intramedullary nail insertion methods • Antegrade insertion (through either the piriformis fossa or the tip of the greater trochanter, depending on the design of nail) or retrograde insertion (through the intercondylar notch distally) are equally suitable techniques to use; there is a small incidence of hip and thigh pain with antegrade nails, whereas there is a small problem with knee pain with retrograde nails. • Open medullary nailing is a feasible alternative where facilities for closed nailing are lacking. A limited lateral exposure of the femur is made; the fracture is reduced and a guidewire is passed between the main proximal and distal fragments.
• Retrograde insertion of intramedullary nails is particularly useful for: 1. obese patients; 2. when there are bilateral femoral shaft fractures (as the procedure can be performed without the need for a fracture table and the added time for setting up for each side); 3. when there is a tibial shaft fracture on the same side; 4. and if there is a femoral neck fracture more proximally, as screws can be inserted to hold this fracture without being impeded by the nail.
Outcome of Intramedullary nail • The fracture usually heals within 20 weeks and the complication rate is low; sometimes malunion (more likely malrotation) or delayed union (from leaving the fracture site over-distracted) occurs.
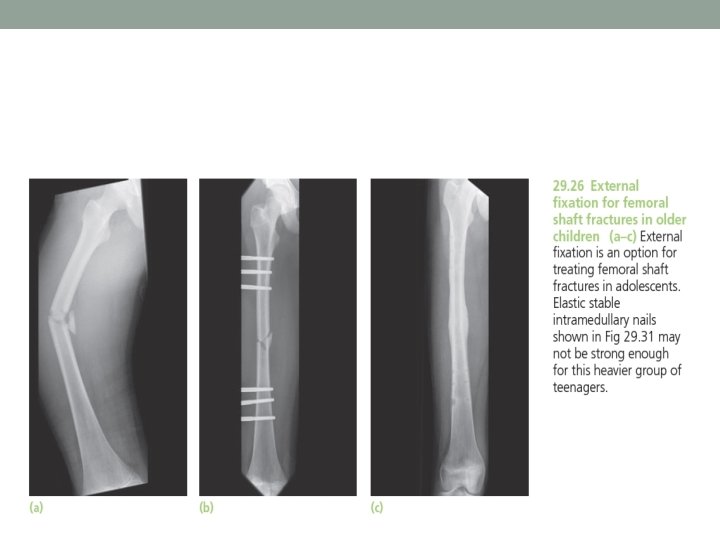
IV. External fixation • The main indications for external fixation are (1) treatment of severe open injuries; (2) management of patients with multiple injuries where there is a need to reduce operating time and prevent the ‘second hit’; and (3) the need to deal with severe bone loss by the technique of bone transport. External fixation is also useful for (4) treating femoral fractures in adolescents
Outcome of External fixation • Like closed intramedullary nailing, it has the advantage of not exposing the fracture site and small amounts of axial movement can be applied to the bone by allowing a telescoping action in the fixator body (with some designs of external fixator). • Partial weight-bearing is usually possible immediately but this will depend on the x-ray appearance of callus – this may take some time (more than 6 weeks) if the fixator is a rigid device. Most femoral shaft fractures will unite in under 5 months but some take longer if the fracture is badly comminuted or contact between fracture ends is poor. • However, there are still problems with pin-site infection, pin loosening and (if the half-pins are applied close to joints) limitation of movement due to interference with sliding structures.
Treatment of open fractures • Open femoral fractures should be carefully assessed for (1) skin loss; (2) wound contamination; (3) muscle ischaemia; and (4) injury to vessels and nerves. • The immediate treatment is similar to that of closed fractures; in addition, the patient is started on intravenous antibiotics. The wound will need cleansing: it should be extended to give unhindered access, contaminated areas and dead tissue must be excised and the entire area should be washed thoroughly. • Stabilization of open femoral shaft fractures is best achieved with locked intramedullary nails unless there is heavy contamination or bone loss – in which case external fixation (if necessary with the capacity to deal with bone loss through distraction osteogenesis) is preferable.
Complex injuries • FRACTURES ASSOCIATED WITH VASCULAR INJURY • Warning signs of an associated vascular injury are…. • Most femoral fractures with vascular injuries will have had warm ischaemia times greater than 2– 3 hours by the time the patient arrives in the operating theatre; when this exceeds 4– 6 hours, salvage may not be possible and the risk of amputation rises. This means that diagnosis must be prompt and re-establishing perfusion a priority; fracture stabilization is secondary.
Management of vascular injury • Do not accept ‘arterial spasm’ as a cause of absent pulses; the fracture level on x-ray will indicate the region of arterial damage and arteriography may only delay surgery to reestablish perfusion. • A recommended sequence for treatment is (a) to create a shunt from the femoral vessels in the groin to beyond the point of injury using plastic catheters; (b) to stabilize the fracture (usually by plating or external fixation) and then (c) to carry out definitive vascular repair.
FRACTURE ASSOCIATED WITH KNEE INJURY • Femoral fractures are frequently accompanied by injury to the ligaments of the knee. Direct blows to the knee from the dashboard of a car in an accident will damage knee ligaments as well as break the femoral shaft and femoral neck – this triad of problems should be recognized. As soon as the fracture has been stabilized, the knee should be carefully examined any associated abnormality treated.
‘FLOATING KNEE’ • Ipsilateral fractures of the femur and tibia may leave the knee joint ‘floating’. This is a very serious situation, and other injuries are often present. Both fractures will need immediate stabilization – an anterior approach to the knee joint will allow both fractures to be stabilized by intramedullary nails – retrograde for the femur and antegrade for the tibia. It is usual to fix the femur first.
COMBINED NECK AND SHAFT FRACTURES • The most important thing is diagnosis: always examine the hip and obtain an x-ray of the pelvis. • Both sites must be stabilized, first the femoral neck and then the femur. Parallel screw fixation of the femoral neck followed by retrograde femoral nailing is a useful way to treat this problem.
PATHOLOGICAL FRACTURES • Fractures through metastatic lesions should be fixed by intramedullary nailing. Provided the patient is fit enough to tolerate the operation, a short life expectancy is not a contraindication. • ‘Prophylactic fixation’ is also indicated if a lytic lesion is (a) greater than half the diameter of the bone; (b) longer than 3 cm on any view, or (c) painful, irrespective of its size. • Paget’s disease, fibrous dysplasia or rickets may present a problem. The femur is likely to be bowed and, in the case of Paget’s disease, abnormally hard. An osteotomy to straighten the femur may be necessary to allow a nail to be inserted fully
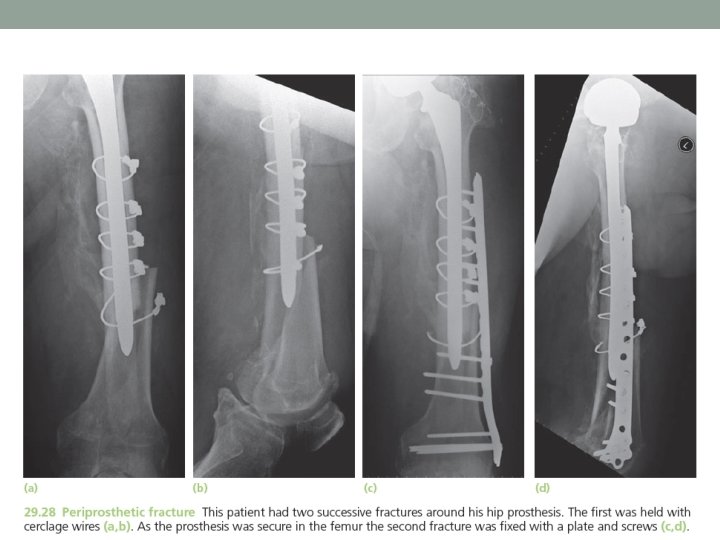
PERIPROSTHETIC FRACTURES • Femoral shaft fractures around a hip implant are uncommon; they may happen during primary hip surgery when reaming or preparing the medullary canal, or when forcing in an over-sized uncemented prosthesis, or during revision surgery while extracting cement or attempting to dislocate the hip if the soft tissue release has been insufficient. Sometimes the fracture occurs much later, and there are usually x-ray signs of osteolysis or implant loosening suggesting a reason for bone weakness.
• If the prosthesis is worn or loose, it should be removed and replaced by one with a long stem, thereby treating both problems. If the primary implant is neither loose nor worn it can be left in place and the fracture treated by plate fixation with structural allografts bridging the fracture
EARLY Complications of femoral shaft fractures • Shock One or two litres of blood can be lost even with a closed fracture, and if the injury is bilateral shock may be severe. Prevention is better than cure; most patients will require a transfusion.
• Fat embolism and ARDS Fracture through a large marrow- filled cavity almost inevitably results in small showers of fat emboli being swept to the lungs. This can usually be accommodated without serious consequences, but in some cases (and especially in those with multiple injuries and severe shock, or in patients with associated chest injuries) it results in progressive respiratory distress and multi-organ failure (adult respiratory distress syndrome). • Blood gases should be measured if this is suspected and signs such as shortness of breath, restlessness or a rise in temperature or pulse rate should prompt a search for petechial haemorrhages over the upper body, axillae and conjunctivae. Treatment is supportive, with the emphasis on preventing hypoxia and maintaining blood volume.
• Thromboembolism Prolonged traction in bed predisposes to thrombosis. Movement and exercise are important in preventing this, but high-risk patients should be given prophylactic anticoagulants as well. • Vigilance is needed and full anticoagulant treatment is started immediately if thigh or pelvic vein thrombosis is diagnosed.
• Infection In open injuries, and following internal fixation, there is always a risk of infection. Prophylactic antibiotics and careful attention to the principles of fracture surgery should keep the incidence below 2 percent.
• If the bone does become infected, the patient should be treated as for an acute osteomyelitis. Antibiotic treatment may suppress the infection until the fracture unites, at which time the femoral nail can be removed and the canal reamed and washed out. However, if there is pus or a sequestrum, a more radical approach is called for: the wound is explored, all dead and infected tissue is removed and the nail as well; the canal is reamed and washed out and the fracture is then stabilized by an external fixator.
• Sciatic nerve injury • Traction by splint or compression are more common than local trauma. May be due to iatrogenic injury. • In a complete lesion the hamstrings and all muscles below the knee are paralysed; the ankle jerk is absent. Sensation is lost below the knee, except on the medial side of the leg. The patient walks with a drop foot and a high-stepping gait to avoid dragging the insensitive foot on the ground. • Sometimes only the deep part of the nerve is affected, producing what is essentially a common peroneal (lateral popliteal) nerve lesion leads to foot drop and sensory lose in the first web on the dorsum of the foot.
LATE Complications of femoral shaft fractures • Delayed union and non-union • If there is failure to progress by 6 months, as judged by serial x-rays, then intervention may be needed.
• A common practice is to remove locking screws from the intramedullary nail to enable the fracture to ‘collapse’ (‘dynamise’ in modern orthopaedic parlance). This can be successful in a small proportion of cases; more often it fails and results in pain as rotational control of the fracture is lost (the femur is often subject to torsional forces in walking). • A better course is to remove the nail, ream the medullary canal and introduce a larger diameter nail – exchange nailing. Bone grafts should be added to the fracture site if there are gaps not closed at the revision procedure.
• Malunion • Fractures treated by traction and bracing often develop some deformity. • Until the x-ray shows solid union the fracture is too insecure to permit weight-bearing; the bone will bend and what previously seemed a satisfactory reduction may end up with lateral or anterior bowing. • No more than 15 degrees of angulation should be accepted
• Malunion is much less likely in those treated with static interlocked nails; yet it does still occur – especially malrotation – and this can be prevented only by meticulous intra-operative and post-operative assessment followed, where necessary, by immediate correction.
• Shortening is seldom a major problem unless there was bone loss; if it does occur, treatment will depend on the amount and its clinical impact – sometimes all that is needed is a built-up shoe.
• Joint stiffness • The knee is often affected after a femoral shaft fracture. The joint may be injured at the same time, or it stiffens due to soft-tissue adhesions during treatment; hence the importance of repeated evaluation and early physiotherapy.
• Refracture and implant failure • Fractures which heal with abundant callus are unlikely to recur. By contrast, in those treated by internal fixation, callus formation is often slow and meagre. With delayed union or non-union, the integrity of the femur may be almost wholly dependent on the implant and sooner or later it will fail.
• If a comminuted fracture is plated, bone grafts should be added and weight-bearing delayed so as to protect the plate from reaching its fatigue limit too soon. • Intramedullary nails are less prone to break. However, sometimes they do, especially with a slow healing fracture of the lower third and a static locked nail; the break usually occurs through the screw-hole closest to the fracture.
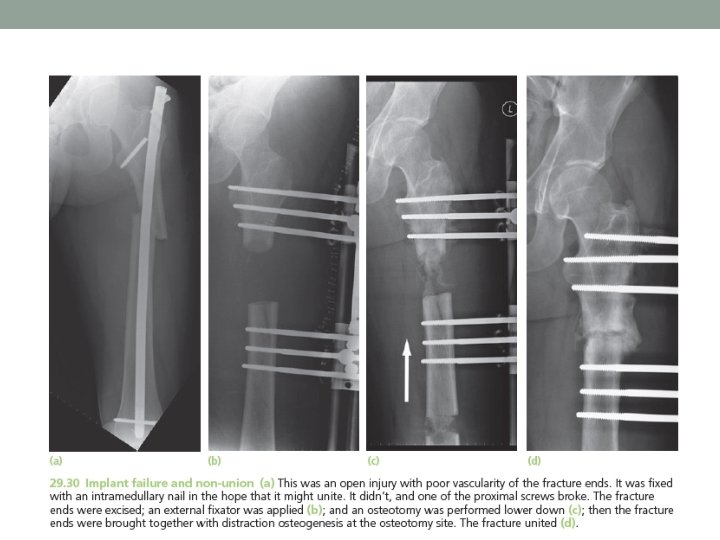
• Treatment consists of replacing the nail and adding bone grafts. In resistant cases, the fracture site may need excising (as viability of the bone ends is poor) followed by distraction osteogenesis which simultaneously stabilizes the limb and deals with the length discrepancy.
lower extremity traction splint for a femur fracture • After a femur fracture, the overriding bone results in loss of soft-tissue tension in the thigh and an increased potential space for hemorrhage. Up to 1 liter of blood can distend the soft tissues of the thigh. A lower extremity traction splint maintains tension on the soft tissues, decreases the amount of hemorrhage, and subsequently improves outcome.
• Perhaps the oldest known lower extremity traction splint is the Thomas splint This splint has been used since the late 1800 s and became famous during World War I when mortality was reduced by 50% after its introduction into battle.
• A modification of this splint is the Hare traction splint, in which a half-ring makes up the most proximal portion
• The Sager splint has a single shaft that is placed on the inner aspect of the leg, but can be applied to the outer side of the leg if a pelvic fracture is present. The splint does not have a half-ring posteriorly, which has two important advantages: (1) relieves any pressure on the sciatic nerve and, (2) reduces hip flexion (which occurs up to 30° in the Hare splint), thereby eliminating angulation of the fracture site.
References • Apley’s System of Orthopaedics and Fractures Ninth Edition • Emergency Orthopedics robert R. simon 5 th edition. • Handbook Of Fractures Koval 3 rd Ed