Tibial shaft fractures AO Trauma Advanced Principles Course

Tibial shaft fractures AO Trauma Advanced Principles Course

Learning objectives • List indications for plating and nailing of tibial shaft fractures • Review specific considerations regarding soft tissues of the lower extremity and discuss indications for an external fixator • Define reduction options in relation to location and type of fracture • Explain the anatomical basis and technique for the use of blocking and ASLS screws in IM nailing • List key outcome publications

External fixation has specific applications for diaphyseal fractures of the tibia

Temporary fixation—indications • Contaminated open fractures • Hemodynamically unstable patient • Periarticular fractures • Complex injury • Multiple bone injuries

Temporary fixation—open fractures • Highly contaminated fracture wounds • Severe soft-tissue damage, especially crush injuries • Stabilization outside zone of injury • Vascular injuries • Unstable hemodynamically • Head injury • “Less experienced” staff

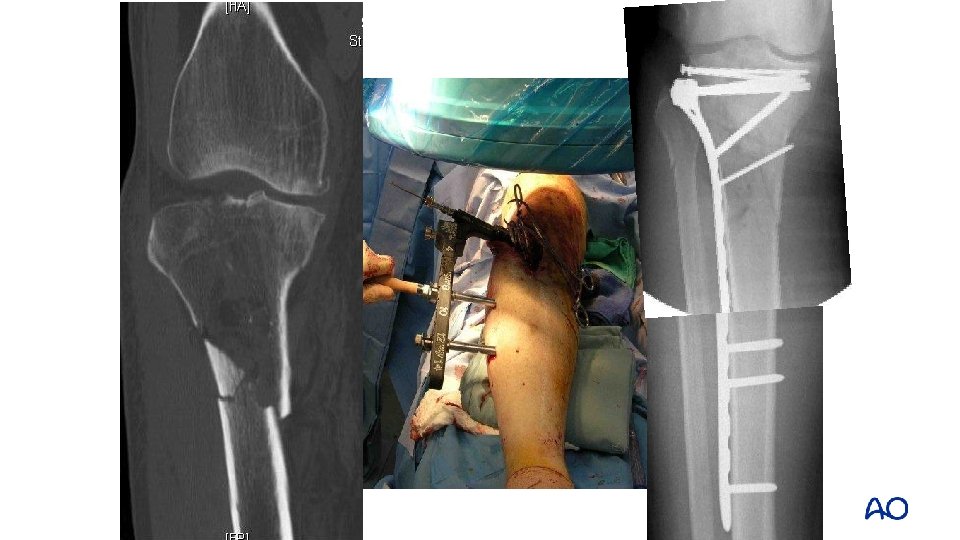
Severe multifragmentary grade IIIB injury

Temporary treatment with external fixator

Temporary fixation—vascular injury • Rapid stabilization around vessel injury • Possible to establish pre-injury length • Stabilizes leg during repair • Knee dislocations

Vascular injury

Fracture stabilized with external fixator

Indications for definitive external fixation • Complex periarticular injuries • Especially when articular injury is simple • Soft tissues not permissive of usual open surgical approach • Major bone loss • Soft tissue injuries precluding incisions • Pediatric patients

Intramedullary nailing is an effective treatment
: Review of")
Nailing outcomes Coles and Gross (Can J Surg. 2000; 43: 256– 262): Review of the Prospective Literature

Functional data • 99 patients • Outcomes analysis of matched pairs • 47 closed IM nail • 52 cast Displaced Isolated Fractures of the Tibial Shaft Treated with Either a Cast or Intramedullary Nailing—Bone et al (J Bone Joint Surg Am. 1997; 79: 1336– 1341)

Better results in nailing group • • Union rate Time to union Infection Return to work 25 patients in each group, assessed at 4. 4 years Better SF-36, p < 0. 05 Better Iowa knee and ankle evaluation, p < 0. 05 Bone et al JBJS 1997

Proximal and distal fractures at risk for malalignment

Deformity with proximal fractures • High rates of malalignment • Lang: 58% • Freedman: 84% • Valgus • Procurvatum (apex anterior)

Valgus Medial entry portal can worsen the valgus

Procurvatum • Patella blocks entry • Posteriorly directed nail insertion • Knee flexion

Techniques to avoid malreduction • Correct starting point • Central and proximal • Nail in extension • Blocking screws • Unicortical plating

Starting point • Start high • Medial side of lateral tibial spine Lateral Medial

Extension nailing Semiextended position 15– 200 flexion Medial parapatellar arthrotomy Tornetta et al (Clin Orthop Relat Res. 1996; 328: 185– 189)

Poller screws • Block passage of nail from unwanted direction • Screws placed on concave side of deformity • Functionally narrows IM canal • Increase strength and rigidity of fixation

Blocking screws

Unicortical plate

Deformity with distal fractures • Malalignment is common with distal fractures • Vallier: 23% (>40) • Freedman: 8%
 clamps • External fixation • Steinman")
Reduction aids for distal fractures • Pointed (percutaneous) clamps • External fixation • Steinman pin • Fibular fixation • Blocking screws

Percutaneous clamps

Clamp + Schanz pin Clam + Ex. Fix

Steinman pin

Fibular fixation • Nork et al (J Bone Joint Surg Am. 2005; 87: 1213– 1221. ) • Egol et al (J Orthop Trauma. 2006; 20: 94– 103. ) Photo from MTOS: Fracture, author: Horowitz

Blocking screw

Plates are effective for proximal and distal fractures

Better alignment in proximal fractures Lower rate of malreduction with plates Lindvall E, et al (J Orthop Trauma. 2009; 23: 485– 492) Bhandari M, et al (J Orthop Trauma. 2003; 17: 591– 595)


Benefits of plates for distal fractures • Less malalignment • High union rate Vallier et al (J Orthop Trauma. 2011; 25: 736– 741) Vallier et al, (J Orthop Trauma. 2012; 26: 327– 332)

Absolute stability technique • Simple fracture • Good soft tissues • Anatomical reduction • Compression • Neutralization

Relative stability technique • Comminuted fracture • Indirect reduction • Bridge plate • Minimally invasive plate osteosynthesis

Soft-tissue status guides treatment decisions

Treatment guided by soft tissues • Damaged soft-tissue envelope favors indirect reduction techniques for acute treatment • Open reduction technique requires an optimal soft-tissue envelope and may require a delayed approach

Take-home messages • External fixation has important temporary and definitive applications • Intramedullary nailing is a highly effective treatment • Malalignment of proximal and distal tibial fractures is common • Plating strategies are effective for proximal and distal fractures • Soft-tissue status dictates surgical approach
- Slides: 42