End of life Care in Chronic Kidney Disease


 – Slow onset of kidney disease which is")
 Ø CKD")

")




 12 (Home) Ø CAPD - 42 Ø")





















 Conservative Kidney Management Guideline. (B) Non- Dialysis Management Guideline.")





 HD 84")



")





- Slides: 53
End of life Care in Chronic Kidney Disease Margie Kennedy Renal Nurse Counsellor September 2011
This presentation Ø Introducing some background information – What is involved for a person living with Chronic Kidney Disease? Ø What are the guidelines ? Ø What are the challenges faced so far since implementing these guidelines in January 2011? Ø Can these guidelines be modified to be of use in other areas of Chronic illness? Ø
DEFINITIONS Ø Chronic Kidney Disease (CRD) – Slow onset of kidney disease which is irreversible. Ø End Stage Kidney Disease (ESKD) – Advanced kidney disease. Ø Dialysis (HD) – An artificial process which removes chemical substances and water from the blood by passing it through an artificial kidney.
Progression of Chronic Kidney Disease Glomerular Filtration Rate (GFR normal 120 mls/min) Ø CKD – Chronic Kidney Disease Ø CKD 1 – GFR – Greater than 90 mls / min Ø CKD 2 – GFR – 60 – 89 mls / min Ø CKD 3 – GFR – 30 – 59 mls / min Ø CKD 4 – GFR – 25 – 29 mls / min Ø CKD 5 – GFR less than 15 mls / min Ø
Advanced kidney disease is not asymptomatic. Ø Potential complications of dialysis is longer than those of chronic kidney disease alone. Ø Clinicians often assume a more favourable prognosis than is justified. Ø For many patients dialysis is not the bridge to renal transplantation. Ø Dialysis doesn’t transform lives – it is often palliative treatment. (Brown et al 2007) Ø
End Stage Renal Disease Ø Options – 1. Dialysis - Haemodialysis CAPD (Peritoneal Dialysis) APD 2. Transplantation –Cadaveric Living Donor / Related , Non - Related 3. Death
Ø Haemodialysis – 4 hrs X 3 times week in Hospital or at Home. Ø APD – 8 -10 hours nightly – Home Ø Diet restriction Ø Fluid restriction Ø Medications Ø Loss of independence
Ø Transplantation Work up – approx 3 -4 month Wait – average 2 -3 yrs Average Function – 15 -16 yrs Success Rate – 95% - 1 year
Chronic Kidney Disease is for Life Ø Post Transplant – Immunosuppression Risk of Rejection Risk of Infection Risk of Diabetes Risk of Skin Cancer Others Ø Clinic Visits – for life – every 3 months
Dialysis / Transplantation affects a Person Socially Physical Psychologically Spiritually
Beaumont Hospital Ø Haemodialysis - 191 (Hospital) 12 (Home) Ø CAPD - 42 Ø Cadaveric Transplant - 138 - 2011 Ø Living Related Transplant - 16 – 2011
Disease Trajectory
Female Renal Patient Age 37 Timeline Ø 1984 – 1985 Ø 1985 – 1987 Ø 1987 – 1991 Ø 1992 - 2005 Ø 2005 – 2011 Ø Haemodialysis Transplant CAPD / HD Transplant Haemodialysis Patient on Dialysis– 16 yrs
Female Renal Patient Age 43 Timeline Ø 1984 – 1990 Haemodialysis Ø 1990 – 2006 Transplant Ø 2006 – 2011 Haemodialysis Patient on HD – 11 years
Female renal patient aged 53 Timeline Ø 1983 - 1986 Ø 1986 – 1988 Ø 1989 – 1998 Ø 1998 – 2004 Transplant Ø 2004 – 2011 Haemodialysis Patient on HD 20 Years Haemodialysis Transplant Haemodialysis
Patient needled 312 per year. 163 Blood tests per year.
Exacerbations and patterns of decline ↑ intensity of psychological, social or spiritual symptoms as well as the more obvious deterioration. (Palliative care for all 2009 )
Veteran Dialysis Patient Ø Ø Ø Years of suffering Cumulative stress/ anxiety Innumeralable needling/procedures/ investigations Challenge of coping/ enduring/ hoping Failed transplant Resilience / Endurance “The illness is an ambiguous loss; a constant grieving process which is mood related and never ending. You are always well enough but never quite right. Rarely sick but always ill” (Liam Mc. Carthy Nov 2007) “He who has a why to live can bear with almost any how” “Nietzsche” (Frankl 1959)
In Relation to the “Veteran” dialysis patient, the biggest challenge of all is how to introduce the subject of End of Life Care Ø How do you broach the subject ? Ø Should you broach the subject? Ø When should you broach the subject? Ø How do you balance the intent to provide good end of life care with the possibility of taking away the person’s hope?
Ø Death is often seen as simply a physiological event, and some even view it as a failure, and even in some instances, a kind of moral failure …. . the ultimate defeat. But the truth is, death is a developmental phase in our life cycle. (Joan Halifax Roshi)
Ø The experience of dying is more than a set of medical problems to be confronted. In fact the fundamental nature of dying is not medical at all. It is personal and experiential. Dying is a personal experience. (Dr. Ira Byock)
2010 “Renal” Deaths Ø Total = 115 Ø Haemodialysis : 54. 8% - Acute HD 19. 1% Chronic HD 35. 7% Ø CKD Stage 2 -5 : 33. 0% (Pre-dialysis) Ø Transplant Ø Peritoneal/CCPD 3. 5% 8. 7%
Ø Average Age of Death – 52 years Ø 59% > 70 years
ØPLACE OF DEATH Ø HOSPITAL = 89. 5% Ø HOME = 8. 7% Ø HOSPICE = 1. 8%
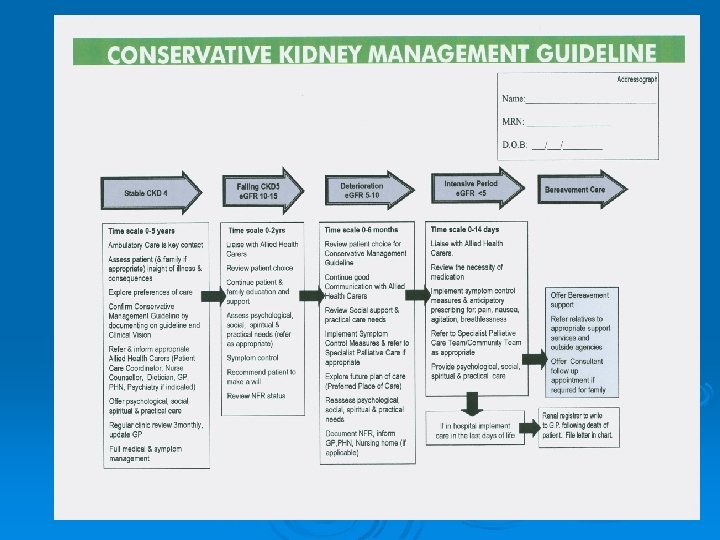
Ø It is important to recognise when End of Life may be approaching, signalling the need to re-focus the emphasis of care to relief of symptoms – maintenance of comfort and attention to psychological, social and spiritual concerns.
A Healthy Death Ø Medical – Physical = Pain Free Ø Social – Emotional = Supportive Ø Pastoral – Spiritual = Peaceful (Sacred Art of Living Center, 2004)
Dying Person’s Bill of Rights Non Abandonment Ø Alleviation of Suffering Ø Respect for total Personhood Ø Choice based on truth telling Ø (Sacred Art of Living Center, 2004)
Guideline Ø A statement of principles giving guidance but allowing for professional initiative. Ø The Guideline provides a template of care to all staff in End of Life care of patients within the TUN Directorate.
Principle It is our responsibility to support people with advanced kidney disease to live life as fully as possible and enable them to die with dignity in a setting of their own choice. In addition, family members are supported throughout the illness of their relative, and are treated with compassion and in a caring manner following the death of their relative.
Ø Not all deaths can be anticipated or planned for. Ø Sudden unexpected deaths – traumatic for family, staff, other patients closely associated through friendship/ shared experiences/ proximity of treatment. Ø Local practice
Timeline to development of this Guideline Ø Invitation by letter to nursing / medical staff in the unit to join an ad hoc committee to work on drawing up a policy on End of Life Care.
Steering Committee Ø 1 Nephrologist Ø 1 Consultant Palliative Medicine/ Specialist Palliative Care Nurse Ø 1 Renal Registrar Ø 2 Patient Care Co-ordinators Ø 3 Ambulatory Care CNS Ø Staff Nurses Ø Renal Counsellors Ø Ø 10 meetings between April 2010 – Feb 2011 Signed off at Nephrology Guideline Committee Meeting 11 th March 2011
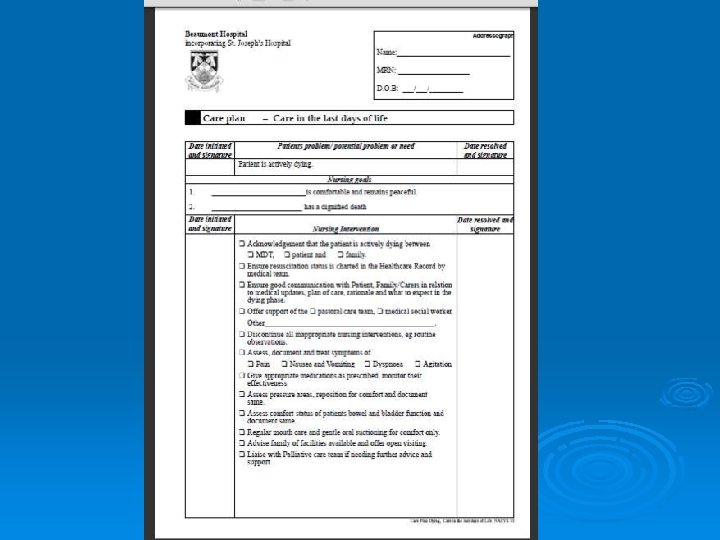
3 parts to Guideline (A) Conservative Kidney Management Guideline. (B) Non- Dialysis Management Guideline. (C) Care in the last days of life Guideline. (Beaumont Hospital)
Conservative Kidney Management Guideline Ø Applies at point on the disease trajectory where the patient has made a decision not to opt for dialysis , Likely at CKD stage 3 -4
CONSERVATIVE MANAGEMENT Ø January 2011 – August 2011Ø Currently - Ø R. I. P. - 7 Patients 3 Patients 76 years 81 years 85 years 2 Patients 87 years 3/12 70 years 2/52
Change of Mind – 2 patients Ø 1 ST Patient Female – 80 years Feb 2011 – CKD Ø April 2011 – Conservative Management Ø May 2011 – Counsellor appointment Ø August 2011 – Change of Mind (Amb. C. /Consultant) Ø
Ø 2 nd Patient Male – 78 years Ø April 2009 – ARF Ø May 2009 – Recovered function Ø Nov 2010 – CKD Ø March 2011 – Conservative management Ø June 2011 – Change of mind (GP/Consultant)
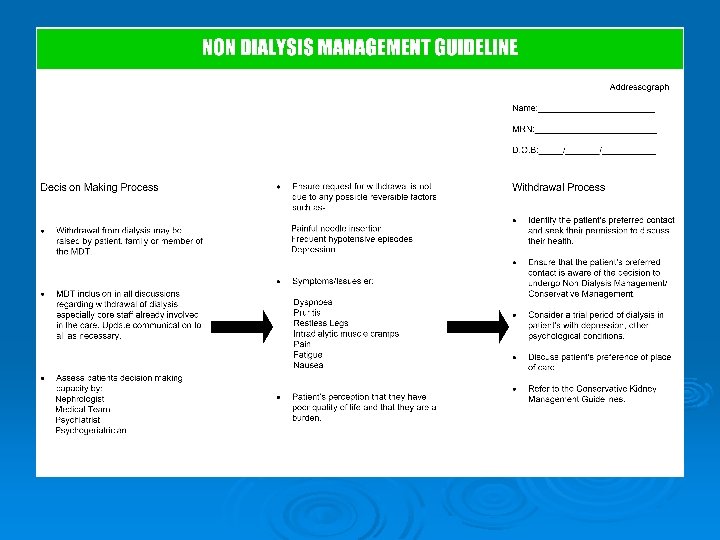
Non-dialysis Management Guideline. Ø Patients who have made a decision to withdraw from dialysis, and for whom dialysis is no longer a suitable treatment for clinical reasons. Ø NB – The patient continues to be actively cared for in all but the provision of dialysis. - proceed to Guideline for Conservative Management of Care in the last days of life.
Withdrawal from Dialysis Ø Total – 6 Ø 2 – Regular (Chronic) HD 84 yrs old -4 yrs HD 82 yrs old -8 yrs HD Ø 4 – Acute (Trial) HD 79 yrs old - 13 days HD 87 yrs old – 15 days HD 94 yrs old – 21 days HD 78 yrs old - 1 month HD
Case Study of Withdrawal of Haemodialysis 82 yrs old Female Ø 10 yrs on HD Ø Decided herself to withdraw from dialysis. Reasons – Ø Ø Ø Ø “Tired of dialysis, ” “No quality of life, ” Recent surgery which greatly impeded her mobility. Little prospect of improvement to mobility. Depression. Psychiatric review. Patient declined anti-depressant. Competency to make decision supported by Consultant Nephrologist, who knew patient X 10 yrs. Patient’s daughter very upset but supportive of patient’s decision.
Ø Patient experienced a crisis of faith, Ø Spiritual pain. Ø Chaplaincy input/ regular support. Ø Specialist Palliative care supervision/support re medications to maintain comfort. Ø Slipped into peaceful coma, Ø RIP – 13 days later.
Ø“The single biggest problem with communication is the illusion that it has taken place. ” (G. B. Shaw)
Challenges so Far Ø Ø Communication. Conservative Management – Decision on ward – (In-pt) - refer to Patient Care Co ordinator. Decision in OPD - refer to Ambulatory Care. Ø Document form and fill out fully. Ø Arrange follow-up OPD appointment. Ø Refer patient to other Health Professionals as required.
Ø Discontinue all non-essential medications before patient leaves the hospital for discharge. Ø Letter to be sent to the GP. Template letter currently in 3 rd draft. Ø Dr. to speak to GP also – ensure you have the correct GP , address, etc. Ø Ensure main carer knows who to contact for support/advice before they leave the hospital. Ø DNA. – follow up call from Ambulatory Care. Ø Notification of Death.
Colleagues Ø Communication Ø Commitment Ø Compassion Ø Caring Ø Common Sense Ø < Carers Charting – Communicate changes – In Chart To GP Ø Checking – Update information / review patients needs Ø Changing – Has the patient’s condition changed ? Are any alterations needed to their care?
Application of these Guidelines to other areas of Chronic illness Ø Multidisciplinary input. Ø Outline significant areas of change on the disease trajectory. Ø Decide on appropriate response to these changes. Ø Document and implement. Ø Review.
For a Nurse May you never doubt the gifts you bring; Rather, learn from these frontiers Wisdom for your own heart. May you come to inherit The blessings of your kindness And never be without care and love When winter enters your own life. (O’Donohue 2007)
Thank you To the Palliative Care Team for Collaboration with us on these Guidelines.