Liver Disease in Thalassaemia Dr Md Habibur Rahman

Liver Disease in Thalassaemia Dr Md Habibur Rahman Professor & Head Department of Gastroenterology SSMC & MH

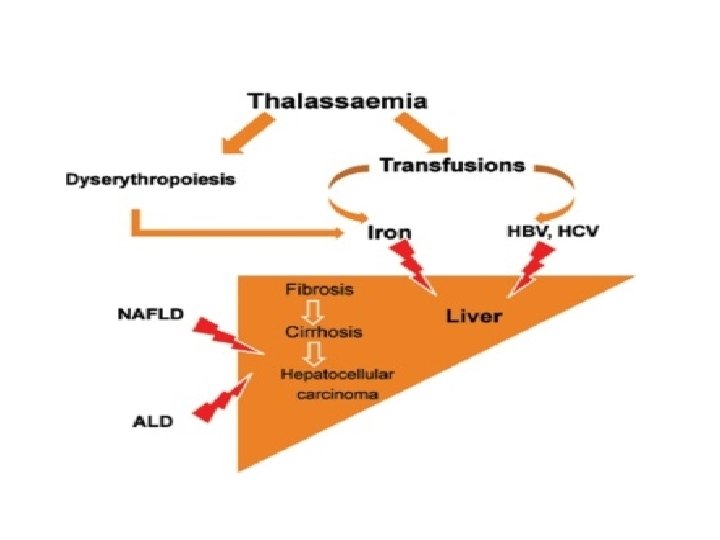
Introduction • Liver is the main iron storage organ. • Liver disease is the second cause of mortality in thalassaemia. • Transfusion related iron overload and hepatitis ( HCV and HBV ) are the main causes of liver damage. • Other factors are non alcoholic fatty liver disease, drugs & alcohol.

Hepatic Iron Overload in Thalassaemia • Total body Fe is 4 gm & daily Fe loss is 1 -2 mg. • One unit blood represents 200 -250 mg iron. • Repeated transfusion leads to rapid development of iron(Fe) overload. • Dyserythropoesis is another important mechanism of iron overload.

How iron overload damage liver ? • Red blood cells are degraded in reticuloendothelial system of spleen and liver ( Kupffer cells ) • Excessive intra-macrophagic iron released into blood stream which bound with transferrin.
 become saturated rapidly. • After saturation")
• Transferrin ( Iron bound protein ) become saturated rapidly. • After saturation of IBP, excess iron ( NTBI ) taken up by the hepatocytes, heart and pancreas. • Non transferrin bound iron ( NTBI ) is highly damaging for liver parenchyma.

How parenchymal cell damage NTBI produce reactive oxygen species Damage of the hepatocyte cell membranes, intracellular organelles including cell nuclei Necrosis finally Fibrosis (ultimate stage of which is cirrhosis and HCC)

Diagnosis of hepatic iron overload • Clinical features –Skin pigmentation Hepatomegaly • Lab investigation– Serum ferritin Plasma trasferrin saturation MRI Liver biopsy (gold standard)
 HIC : normal ( <40 µmol/gm liver wt. ) Type HIC")
Hepatic Iron Concentration(HIC) HIC : normal ( <40 µmol/gm liver wt. ) Type HIC (µmol/gm) Mild 40 - 120 Moderate 120 - 240 Severe > 240

Diagnosis of hepatic disease in general • Clinical features. Jaundice, Oedema Hepatomegaly, other stigmata of CLD Sign of portal hypertension.

Diagnosis of hepatic disease in general • Lab investigation. SGPT, prothrombin time, S. total protein and albumin, Alpha fetoprotein, USG of HBS, Fibroscan Endoscopy of upper GIT, Liver biopsy

Treatment of hepatic iron overload • When treatment should be initiated, remain unclear. • Classically, serum Ferritin 1000 mg/ml used as indication of treatment. • However, Hepatic Iron Concentration (HIC) is the most reliable parameter. ( HIC > 40 µmol/gm dry wt )

Chelating agents : usually start between 2 -4 yrs after 20 -25 transfusion. 1. Desferrioxamine : 30 -40 mg/kg subcutaneously 5 days/week 2. Deferiprone : 75 -100 mg/kg orally 3 times/day with desferrioxamine/ monotherapy 3. Deferasirox : 5 -20 mg/kg/day
 is a major cause of")
Hepatitis C in Thalassaemia • Hepatitis C virus (HCV) is a major cause of CLD worldwide. • About 71 million peoples are chronically infected in the world. • Natural history is variable. • Most of the patients (about 85%) become chronically infected. • Most of the cases remain asymptomatic before development of features of CLD.

• HCV infection is a major concern in thalassaemia. • Overall prevalence in general population is < 1%. • About 4 -85% of thalassaemic pt are positive for HCV antibodies ( Di Macro- 2010). • In Bangladesh the prevlence is about 26% (Thalassaemia foundation. ) • Two factors are important— a) Hepatic iron overload b) Limitation of use of antiviral treatment

• In some developing countries, HCV screening of blood donors has not been established, at least not all blood banks have conformed to the requirement, and so the risk for patients is still high. • In conjunction with iron overload, chronic hepatitis C is an important contributor to liver disease, making the availability of effective treatment essential.

Diagnosis of HCV infection When Suspected ? 1. If transfusions were started before 1991 and 2. Raised S. transaminases persist > 6 months. Anti-HCV Antibodies False Negative – Early acute infection Immunosuppresed patient HCV RNA detection & Genotyping.

Evaluation for liver disease Clinical Investigation Asymptomatic Hepatomegaly Ascitis Stigmata of chronic liver disease Complete blood count ALT AST/Platelet ratio Prothrombin time S. Total protein & albumin USG of HBS Fibroscan Endoscopy to see portal HTN Liver biopsy

Treatment • The treatment choices cannot be made by the thalassaemia unit alone and should be made by respective specialist (Gastroenterologist/Hepatologist). • The indications for HCV therapy are the same in patients with and without haemoglobinopathies.

• The IFN-free, ribavirin-free anti-HCV regimens that can be used in patients with haemoglobinopathies are the same as in patients without haemoglobinopathies. • Available drugs are--– Pegylated Interferon – Ribavirin – Sofosbuvir – Velpatasvir – Daclatasvir – Ledipasvir

Challenges However the availability of drugs, their use in children is difficult because--1. Interferon : not given < 7 yrs 2. Ribavirin : causes autoimmune hemolytic anaemia 3. Sofosfovir, Velpatasvir, Daclatasvir and Ledipasvir – Not indicated < 12 years. 4. Re infection 5. Vaccination still not available.

Hepatitis B in Thalassaemia • Global public health problem. • About 240 million people are chronically infected. • Prevalence is decreasing due toa) b) c) d) Socio-economic status improvement Universal vaccination program Effective antiviral therapy Screening of blood donors.

• In thalassaemia, HBV infection affect 0. 3 – 5. 7% of patients. In Bangladesh – about 1% (TF). • Vaccinations, effective treatment and blood donors screening have considerably reduced the incidence of HBV infectoins.

• HBV infection : 4 phases— I. III. IV. HBe. Ag positive chronic infection HBe. Ag positive chronic hepatitis HBe. Ag negative chronic infection HBe. Ag negative chronic hepatitis

Assessment of patient HBV markers Extent of liver disease HBs. Ag HBe. Ag Anti HBc Ig. M & Total Anti Hbe HBV DNA S. Bilirubin ALT Prothrombin time S. Total protein & Albumin USG of HBS Fibroscan Liver biopsy

To Whom Treatment Given 1. HBe. Ag +/- chronic hepatitis B, HBV DNA > 2000 IU/ml, ALT > ULN, and/or liver necroinflammation or fibrosis. 2. Compensated or decompensated cirrhosis with any detectable HBV DNA level.

3. HBV DNA > 20, 000 IU/ml and ALT > 2 X ULN 4. HBe. Ag + chronic HBV infection, persistantly normal ALT and high HBV DNA 5. HBe. Ag +/- chronic HBV infection with family H/O of HCC or cirrhosis

Available Drugs – Pegylated Interferon – Lamivudine – Adefovir – Entecavir First line drugs – Tenofovir – Telbivudine

Duration of Treatment Condition Pegylated Interferon NA analogues Non Cirrhosis 48 wks Undetectable DNA for two conscecutive years Cirrhotic Compensated 48 wks Indefinity Contradicted Indefinity Decompensated

Summary • Prevalence of HCV infection is very high in thalassaemic patient due to ineffective screening. • Screening of donor should be meticulous. • Vaccination of HBV must be ensured. • Reversal of hepatic iron excess is a key objective to protect the liver. • Diagnosis and treatment of HCV and/or HBV chronic hepatitis remain important.

- Slides: 31