NICE Chronic Kidney Disease CKD Guidance 2014 Chronic
 Guidance 2014 Chronic kidney disease in adults: assessment and")



 Terms G 1 >90 Normal or high")








")










- Slides: 27
NICE Chronic Kidney Disease (CKD) Guidance 2014 Chronic kidney disease in adults: assessment and management (CG 182)
NICE CKD Guidance 2014 • Changes to e. GFR calculation and reporting • Updated classification of CKD • New areas of controversy • Serious flaws in the guidance, but how to manage these? • But first… what is a normal e. GFR?
Acceptable GFR by donor age prior to donation www. bts. org
e. GFR • Most centres were using the MDRD equation • The NICE guidelines recommended that laboratories start using the CKD-EPI equation • e. GFR should be reported up to 90 ml/min
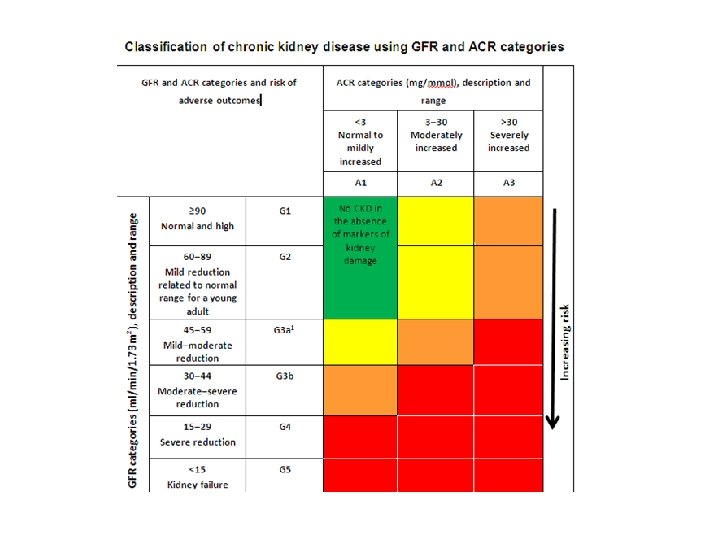
Classification of CKD GFR category GFR (ml/min) Terms G 1 >90 Normal or high G 2 60 -89 Mildly decreased* G 3 a 45 -59 Mildly to moderately decreased G 3 b 30 -44 Moderately to severely decreased G 4 15 -29 Severely decreased G 5 <15 Severely decreased ACR category ACR (mg/mmol) Terms A 1 <3 Normal to mildly increased A 2 3 -30 Moderately increased A 3 >30 Severely increased
Offer testing for CKD to people with… • Diabetes • Hypertension • History of acute kidney injury • Cardiovascular disease • Structural renal tract disease, recurrent renal calculi or prostatic hypertrophy • Multisystem diseases with potential kidney involvement – for example, systemic lupus erythematosus • Family history of end-stage kidney disease or hereditary kidney disease • Opportunistic detection of haematuria
Who should have a renal ultrasound… Offer a renal ultrasound scan to all people with CKD who • have accelerated progression of CKD • have visible or persistent invisible haematuria • have symptoms of urinary tract obstruction • have a family history of polycystic kidney disease and are aged over 20 years • have a GFR of less than 30 ml/min
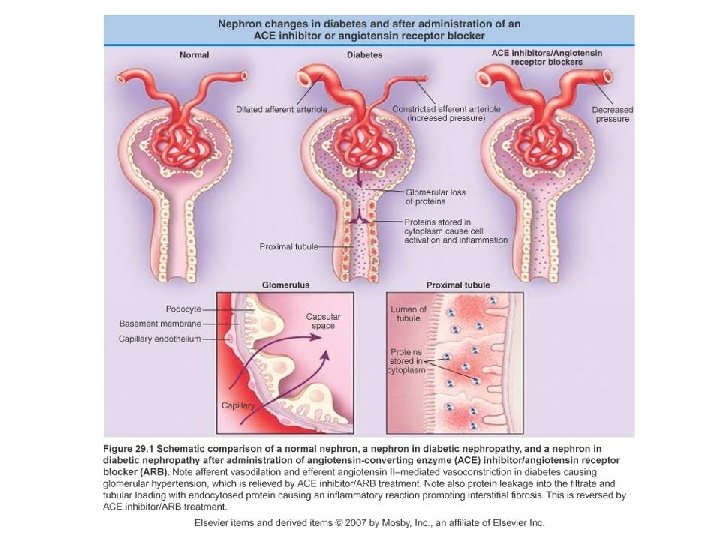
Preventing progression of CKD • Control BP < 130/80 • Reduce proteinuria with ACEi or ARBs • Excellent glycaemic control can prevent the onset of microalbuminuria
Patients with e. GFR between 45 -59
e. GFRcystatin. C Do not diagnose CKD in people with • an e. GFRcreatinine of 45– 59 ml/min, and • an e. GFRcystatin. C of more than 60 ml/min, and • no other marker of kidney disease
Patients with e. GFR 60 - 90
Patients with e. GFR 60 - 90 If e. GFR 60 -90 (and it is not deteriorating over time- several checks needed over at least 3 months to establish this) And, if: Completely normal BP off antihypertensives Completely normal urine dipstick No albuminuria on ACR No family history of renal disease No personal history of kidney disease No past medical history (including no diabetes, no renal stone disease, no cardiovascular disease, no multi-system disease etc) …then the person doesn’t have CKD as defined in the NICE CKD guidelines…
Patients with e. GFR 60 - 90 However, we do feel uncomfortable not monitoring these patients in any way, especially if they are younger adults. The renal consultants at Truro recommend that people have an annual check of U&E, BP, and urine ACR until age ~60 -70 to monitor for the development of CKD.
CKD Primary Care resources • Kernow Clinical Commissioning Group Referral Management System (KCCG RMS) website • rch-tr. Renal@nhs. net
Feedback on the email service • The number of emails to the service has doubled since 2011, with 168 new email queries in 6 months in 2015. • Users of the service reported very high satisfaction with the timing of advice, as well as the quality of the advice • There continues to strong interest and appreciation of this service
CKD: In Summary • Natural decline in e. GFR with age • e. GFR can now be reliably reported up to 90 ml/min • If e. GFR 60 -90 and no other markers of kidney damage then this is reassuring, but recommend annual monitoring
Questions/ Comments
Questions from the sticky notes…
Closing remarks Thank you to the invited speakers – Dr Fergus Caskey, Medical Director UK Renal Registry, Renal Consultant at North Bristol NHS Trust. – Dr Kathryn Griffith, RCGP Clinical Champion for Kidney Care, Cardiovascular Lead for Vo. YCCG, GP – Dr Anna Barton, Principal Biochemist, Royal Cornwall Hospitals Trust
Closing remarks Acute Kidney Injury • Primary Care has a crucial role in prevention, detection and management of AKI • AKI often means SICK ADULT
Objectives- AKI • To be aware of the impact of AKI on patient safety • To be aware of the 3 stages of AKI • To be aware of the planned ‘switch on’ of AKI alerts to primary care • To increase confidence of how to respond to an AKI alert
Closing remarks Chronic Kidney Disease • Tools are available to assist Primary Care to detect deteriorating CKD • To be aware of the implications of the NICE CKD guidelines from 2014 • To improve awareness of which patients can be managed in Primary Care
Thank You!