Drugs for Coagulation Disorders Andrew N Schmelz Pharm


 n Categorize coagulation-modifying drugs based on their classification and mechanism of action")


 (Factor Xa) Extrinsic Pathway (Blood enters tissue spaces)")

 disorders (MI and – Stationary clot (thrombus) grows")
 n Thrombocytopenia – Low number of platelets, cannot properly form")

")
 n MOA: Enhances inhibitory effect of antithrombin III (inhibits")
")
 n MOA: Enhances inhibitory effect of antithrombin III (inhibits")
 n MOA: Enhances inhibitory effect of antithrombin III")
 n MOA: Inhibits enzymes responsible")
 Bivalirudin (Angiomax®) n MOA: Directly inhibit thrombin")
 Argatroban Bivalirudin")
 Bivalirudin (Angiomax®) n MOA: Directly inhibit thrombin")


")
 n MOA: Inhibit GP IIb/IIIa, enzyme")
 n MOA: Inhibit GP IIb/IIIa, enzyme")
 n Example: Aspirin (Ecotrin®) n MOA: Irreversibly binds to COX, inhibiting formation")
 n Example: Aspirin (Ecotrin®) n MOA: Irreversibly binds to COX, inhibiting formation")
 n MOA: ADP-receptor blockers")
 n MOA: ADP-receptor blockers n Route: IV")
 n MOA: PDE-3 inhibitor n Route:")
 n Combination")

 n MOA: Fibrin-enhanced conversion of plasminogen to plasmin")
 n MOA: Fibrin-enhanced conversion of plasminogen to plasmin")


 n MOA: Inhibits fibrinolysis (affects multiple mediators)")
 n MOA: Inhibits fibrinolysis (affects multiple mediators) n Route:")



- Slides: 45
Drugs for Coagulation Disorders Andrew N. Schmelz, Pharm. D Post-Doctoral Teaching Fellow Purdue University October 8, 2008 anschmel@purdue. edu
Objectives n List important steps of hemostasis and fibrinolysis n Describe thromboembolic disorders that are indications for coagulation modifiers n Identify the primary mechanism for each coagulation modifying-drug discussed n Match specific coagulation-modifying drugs to lab tests with which they are appropriately monitored
Objectives (cont) n Categorize coagulation-modifying drugs based on their classification and mechanism of action n List important adverse effects for each coagulation-modifying drug discussed
Process of Hemostasis n Hemostasis: Protects the body from both external and internal injury n Injury to blood vessels causes: – Vessel spasms (causing constriction) – Platelet adherence to injury site – Platelets aggregate and form plug – Insoluble fibrin strands form and coagulate
Process of Hemostasis
Intrinsic Pathway (In response to injury) (Factor Xa) Extrinsic Pathway (Blood enters tissue spaces)
Removal of Blood Clots n Fibrinolysis: Removal of clot so that tissue can resume its normal activity
Diseases of Hemostasis n Thromboembolic CVA) disorders (MI and – Stationary clot (thrombus) grows and deprives specific areas of oxygen n Deep Vein Thrombosis (DVT) – Formation of clots in large veins (usually legs) n Embolus – Thrombus may break off and be carried by bloodstream to affect other areas
Diseases of Hemostasis (cont) n Thrombocytopenia – Low number of platelets, cannot properly form clots n Hemophilias – Genetic deficiencies of clotting factors
Mechanisms of Action n Anticoagulants – Inhibition of clotting factors n Antiplatelets – Inhibition of platelet function n Thrombolytics – Lyse thrombi n Hemostatics – Inhibition of fibrinolysis
Inhibition of Clotting Factors (Anticoagulants)
Heparin n Example: Heparin (Heplock®) n MOA: Enhances inhibitory effect of antithrombin III (inhibits factor Xa)
Heparin Enoxaparin (Factor Xa)
Heparin n Example: Heparin (Heplock®) n MOA: Enhances inhibitory effect of antithrombin III (inhibits factor Xa) n Route: IV (continuous infusion), SC n Monitoring: a. PTT (25 -40 s), platelets, s/sxs of hemorrhage n Adverse Effects: – Hemorrhage – Anaphylaxis – Thrombocytopenia (HIT)
Low-Molecular-Weight Heparins n Example: Enoxaparin (Lovenox®) n MOA: Enhances inhibitory effect of antithrombin III (inhibits factor Xa) n Route: SC n Monitoring: Anti-factor Xa, SCr, platelets n Adverse Effects: – Hemorrhage – Thrombocytopenia – Hypersensitivity (anaphylaxis)
Vitamin K-Dependant Clotting Factor Inhibitors n Example: Warfarin (Coumadin®) n MOA: Inhibits enzymes responsible for cyclic conversion of Vitamin K n Route: PO n Monitoring: PT/INR (12 -15 / 2 -3. 5), s/sxs of hemorrhage n Adverse Effects: – Hemorrhage – Anemia – Bruising
Direct Thrombin Inhibitors n Examples: Argatroban (Novastan®) Bivalirudin (Angiomax®) n MOA: Directly inhibit thrombin (preventing formation of fibrin clots)
(Factor Xa) Argatroban Bivalirudin
Direct Thrombin Inhibitors n Examples: Argatroban (Novastan®) Bivalirudin (Angiomax®) n MOA: Directly inhibit thrombin (preventing formation of fibrin clots) n Route: IV n Monitoring: a. PTT (25 -40 s) n Adverse Effects: – Serious internal hemorrhage – Back pain (bivalirudin)
Nursing Considerations n Medication Safety n Assess patients for signs of bleeding – Bruising – Obvious signs of bleeding (nosebleeds, bleeding from rectum, blood in emesis) – “Coffee Ground” or black, tarry stools / emesis n Patient education n Toxicity: warfarin – vit K administration heparin – protamine sulfate
Patient Case n JR is 55 YOWM recently diagnosed with a DVT and is currently receiving enoxaparin (Lovenox). n Before he can be d/c’ed from the hospital, his MD wants to starts him on chronic anticoagulation to prevent future DVTs
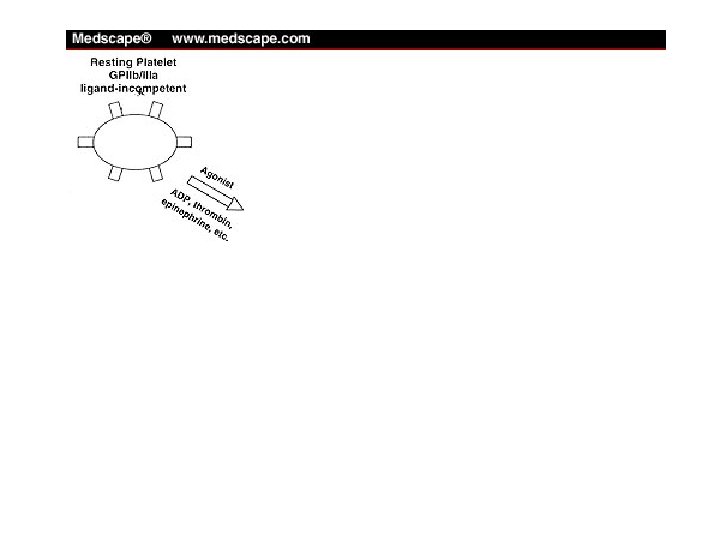
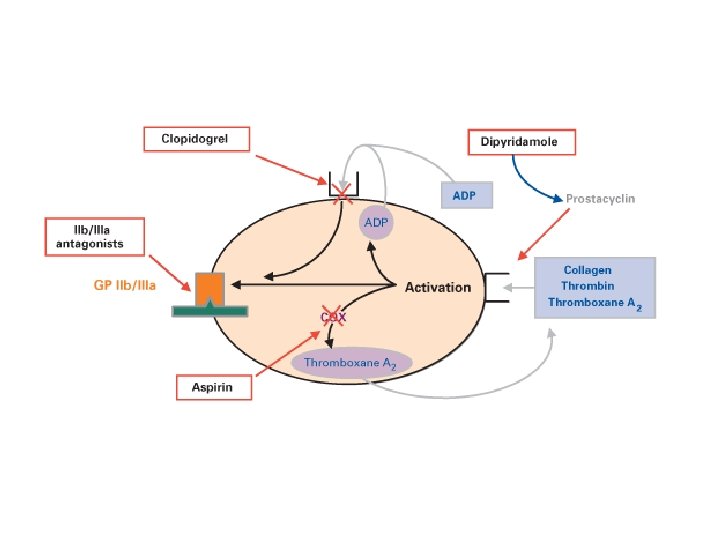
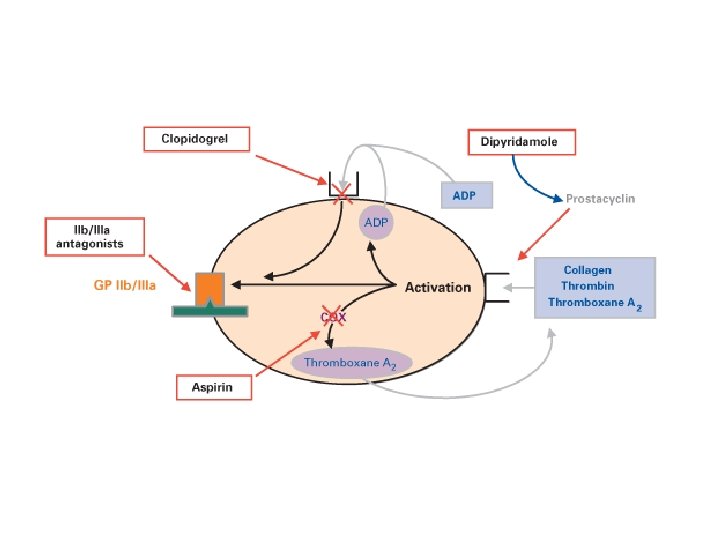
Inhibition of Platelet Function (Antiplatelets)
GP IIb/IIIa Antagonists n Example: Abciximab (Reo. Pro®) n MOA: Inhibit GP IIb/IIIa, enzyme necessary for platelet aggregation
GP IIb/IIIa Antagonists n Example: Abciximab (Reo. Pro®) n MOA: Inhibit GP IIb/IIIa, enzyme necessary for platelet aggregation n Route: IV n Monitoring: Platelets n Adverse Effects: – Hemorrhage – Thrombocytopenia
Aspirin (Ecotrin®) n Example: Aspirin (Ecotrin®) n MOA: Irreversibly binds to COX, inhibiting formation of thromboxane A 2
Aspirin (Ecotrin®) n Example: Aspirin (Ecotrin®) n MOA: Irreversibly binds to COX, inhibiting formation of thromboxane A 2 n Route: PO n Monitoring: S/sxs hemorrhage n Adverse Effects: – Increased clotting times – GI bleeding – Anaphylaxis
ADP Receptor Blockers n Example: Clopidogrel (Plavix®) n MOA: ADP-receptor blockers
ADP Receptor Blockers n Example: Clopidogrel (Plavix®) n MOA: ADP-receptor blockers n Route: IV (loading dose), PO n Monitoring: S/sxs hemorrhage n Adverse Effects: – Increased clotting time – GI bleeding – Blood dyscrasias (TTP)
Agents for Intermittent Claudication n Example: Cilostazole (Pletal®) n MOA: PDE-3 inhibitor n Route: PO n Monitoring: S/sxs hemorrhage, heart n Adverse Effects: – Palpitation, tachycardia, – Nausea, vomitting
Nursing Considerations n Careful monitoring of patient condition (increased risk of bleeding) n Combination with anticoagulants – increased risk of bleeding n Injection / venipuncture sites will require prolonged pressure to control bleeding n Patient education
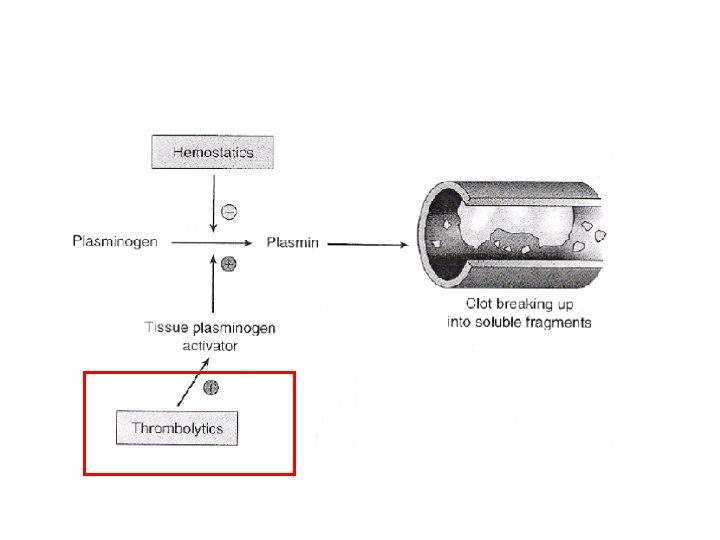
Pharmacotherapy with Thrombolytics
Thrombolytics n Example: Alteplase (Activase®, TPA) n MOA: Fibrin-enhanced conversion of plasminogen to plasmin
Thrombolytics n Example: Alteplase (Activase®, TPA) n MOA: Fibrin-enhanced conversion of plasminogen to plasmin n Route: IV n Monitoring: S/sxs hemorrhage, coagulation tests, H/H, platelets, mental status, dysrhythmias (MI) n Adverse Effects: – Serious internal bleeding – Intracranial hemorrhage
Nursing Considerations n Identify underlying conditions that exclude patient from receiving thrombolytics – Recent trauma, surgery, or biopsy – Arterial emboli – Recent cerebral embolism – Hemorrhage – Thrombocytopenia – Childbirth (within 10 days)
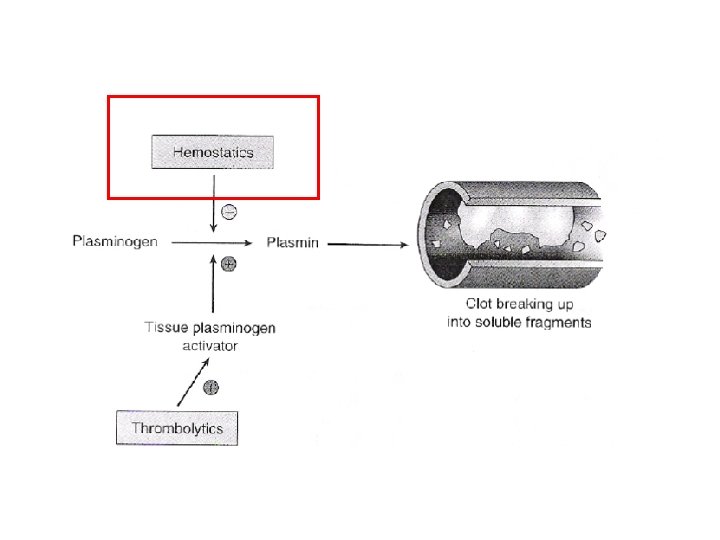
Pharmacotherapy with Hemostatics
Hemostatics n Example: Aprotinin (Trasylol®) n MOA: Inhibits fibrinolysis (affects multiple mediators)
Hemostatics n Example: Aprotinin (Trasylol®) n MOA: Inhibits fibrinolysis (affects multiple mediators) n Route: IV n Monitoring: Clotting, peripheral pulses, paresthesias, (+) Homans’ sign n Adverse Effects: – Clotting – Extravasation
Questions
Summary n Hemostasis protects the body from injury n Several pathologies may affect hemostasis n Four main drug categories are used to treat coagulation disorders n Nurses play an important role – Monitoring drug efficacy – Monitoring patient for adverse effects
Drugs for Coagulation Disorders Andrew N. Schmelz, Pharm. D Post-Doctoral Teaching Fellow Purdue University October 8, 2008 anschmel@purdue. edu