Child Maltreatment Outcomes Integrate the evaluation of child













 �RED flag Physical Examination �Torn frenulum (object forced into mouth)")
 �RED Flags radiologic findings �Metaphyseal fractures (corner fractures) �Rib fractures")







 �Signs and symptoms �Vomiting �Irritability �Decreased oral intake �Respiratory distress")







 are")

- Slides: 39
Child Maltreatment
Outcomes �Integrate the evaluation of child maltreatment into daily nursing practice �Identify risk factors, key indicators, common physical injuries, and long term consequences of child maltreatment �Recognize that screening, evaluation, and appropriate nursing interventions are extremely important for victims of child treatment �Appreciate the value of documentation, evidence collection, and the importance of reporting suspected child maltreatment to appropriate local authorities
Introduction �Physical abuse an important cause for pediatric morbidity and mortality �Associated with major physical and mental health problems that extends into adulthood �Child Abuse Prevention and Treatment Act �“any recent act or failure to act on the part of a parent or caregiver, which results in death, serious physical or emotional harm, sexual abuse or exploitation…or an act or failure to act which prevents an imminent risk of serious harm. ”
Epidemiology �Vast majority of children under-identified with 71% of fatalities from maltreatment are < 3 yrs �Acting alone or with another parent were responsible for 77. 7% of child maltreatment or neglect fatalities �Children who endure repeated abuse and neglect may experience attachment disorder, cognitive challenges, social difficulties, and compromised mental health �Prone to both substance abuse, police and judicial interactions �Stress, immune, neuroendocrine problems throughout life. �High incidence of repeating behavior with one own’s children
Long Term Consequences �Those who endure repeated abuse and neglect �attachment disorder �Cognitive challenges �Social difficulties �Compromised mental health �More prone to substance abuse �Increased negative contact with law enforcement and the judicial system �Emerging recognition that adverse childhood experiences including physical abuse, influence biological adaptations associated with how the brain, neuroendocrine stress response, and immune system function
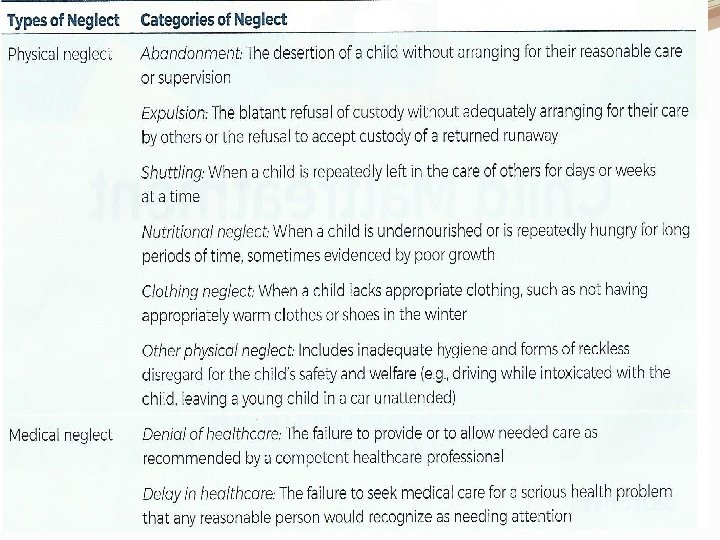
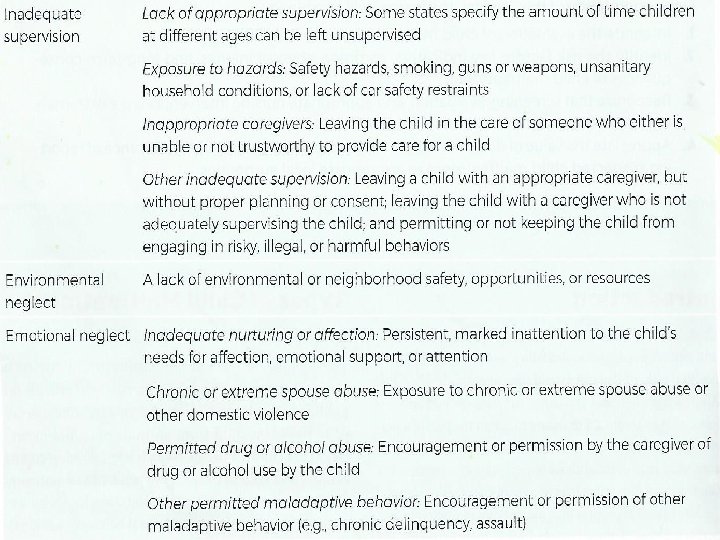
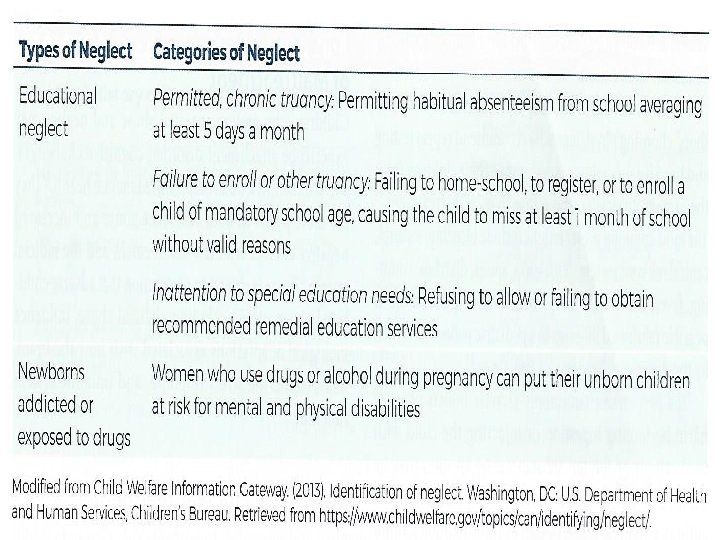
Neglect �Most common �Failure to provide for child’s basic physical, emotional, or educational needs or to protect a child from harm or potential harm �Neglected children do not learn how to develop coping abilities and tend to be overly dependent and unhappy �Tend to develop criminal behavior, personality disorders, substance abuse, and stressful life events
Physical Abuse �Physical abuse make direction much more objective than other forms of abuse �Unintentional and intentional injuries �Past medical history / “story” VERY important to build evidence �Monitor for signs of discrepancies
Psychological Abuse �Intentional behavior on the part of the caregiver that conveys to a child that they are worthless, flawed, unloved, unwanted, endangered, or valued only in meeting another’s needs �Emotionally abused children do not learn how to regulate and control emotional expression, nor do they learn to manage the subtleties of emotional life. �Difficult for nurse to pinpoint with limited exposure (like ED). Might take several exposures.
Sexual Abuse �Any completed or attempted sexual act, sexual contact with, or exploitation of a child by a caregiver �Those who have experienced sexual abuse require consistent, objective, and immediate medical care, with forensic evidence collected by ED (SANE) nurses and medical providers trained in jurisdictional guidelines and protocols �Goes unreported into adulthood �Many children fearful of “breaking the rules” �Does not want to upset or disappoint alleged abuser �Manipulate and silence children creating opportunity for offenders �Child’s dependence on caregivers �Child’s developmental age �Cognitive ability
Medical Child Maltreatment �AKA Munchhausen Syndrome by Proxy AKA Pediatric Condition Falsification AKA Factitious Disorder by Proxy AKA Factitious Disorder AKA Medicinal Abuse �A child receives unnecessary and harmful or potentially harmful medical care at the instigation of a caretaker �Factitious disorder; factitious disorder by proxy, medicinal abuse, and pediatric condition falsification �Perpetrators tend to “doctor shop” choosing physicians who recommend repeat testing and invasive procedures, and remove their children from the care of physicians who refuse to escalate treatment �Motivation usually need for attention or to covertly manipulate or deceive authority figures �Often leads to disability or death
Risk Factors for Maltreatment CHILD �Emotional/ behavioral difficulties �Chronic illness �Physical disabilities �Developmental disabilities �Preterm birth �Unwanted child �Unplanned pregnancy PARENT �Low self-esteem �Poor impulse control �Substance/alcohol abuse �Parent was abused as a child �Depression or other mental illness �Poor knowledge of child development or unrealistic expectations for child �Negative perception of normal child behavior
Risk Factors for Maltreatment �Environment �Social isolation �Poverty �Unemployment �Low educational achievement �Single parent �Non-biologically related male living in household �Family or intimate partner violence �Immigrant families
Intentional Trauma Screening �RED Flag history of present illness �No history or inconsistent history �Changing history �Unwitnessed injury �Delay in seeking care �Prior ED visit �Domestic violence in home �Premature infant (<37 weeks) �LBW �Chronic medical conditions
Intentional Trauma Screening (continued) �RED flag Physical Examination �Torn frenulum (object forced into mouth) �Failure to thrive �Large heads in infants (need to measure circumference on all kids <12 months) �Any bruise on a non-ambulating child �Any bruise in a non-exploratory location (torso, ears, neck) in kids , 4 years �Bruises, marks, or scars in patterns that suggest hitting with an object
Intentional Trauma Screening (continued) �RED Flags radiologic findings �Metaphyseal fractures (corner fractures) �Rib fractures (especially posterior) in infants �Any fracture in a non-ambulating infant �Undiagnosed healing fracture �Subdural hematoma and/or subarachnoid hemorrhage or neuroimaging in young children, particularly in the absence of skull fracture (children younger than 1 year)
“What happened here” �Asking the verbal child – looking for body language and facial expressions along with speech pattern �Children more apt to describe story behind injury when it is not a result of abuse �Compare explanations with pattern of injury, and caregiver
Bruises �Most common �Raise level of suspicion if not in areas as a result of exploring �Mnemonics TEN-4 -FACES for suspicious bruising �Torso �Ear �Neck �Frenulum �Auricular of the ear �Cheek �Eyelid �Sclera �YOUNGER THAN 4 years
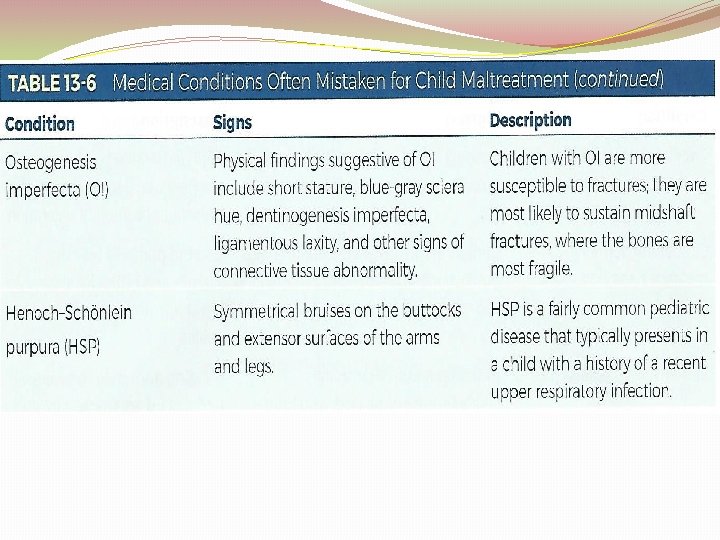
Fractures �Very common in ambulating children �Second most common presentation in maltreatment �Raise concern of physical abuse in non-ambulatory children with fractures and no clear history of how the injury occurred �Certain particular skeletal injuries might raise concern especially for <2 years
Skeletal Injury in Intentional Trauma �Long bones �Classic fracture “Corner” or “Bucket Handle” epiphyseal/metaphyseal seen as a “bucket handle” or “corner” fracture at end of long bones �Secondary to jerking or shaking child’s limb �Spiral fractures may be suspicious of abuse but can be seen with rotational forces (e. g. , “toddler’s fracture” of the tibia
Skeletal Injury in Intentional Trauma �Ribs �Posterior displaced rib fractures are usually due to severe squeezing of the rib cage. �May not be visible on plain film until callus formation occurs
Skeletal Injury in Intentional Trauma �Skull �Fractures more than 3 mm wide, complex fractures, bilateral fractures, and nonparietal fractures suggest forces greater than those sustained from minor household trauma
Abusive Head Trauma �AKA shaken baby Syndrome �Leading cause of intentional death �Absence of history of injury �Subdural, retinal hemorrhage �Fractures of ribs and long bones �Initial presentation may mimic other neurologic or medical problems
Abusive Head Trauma (continued) �Signs and symptoms �Vomiting �Irritability �Decreased oral intake �Respiratory distress without respiratory illness �Seizures �Behavioral changes �Delayed development �Urgent neurologic and ophthalmology diagnostics and assessment
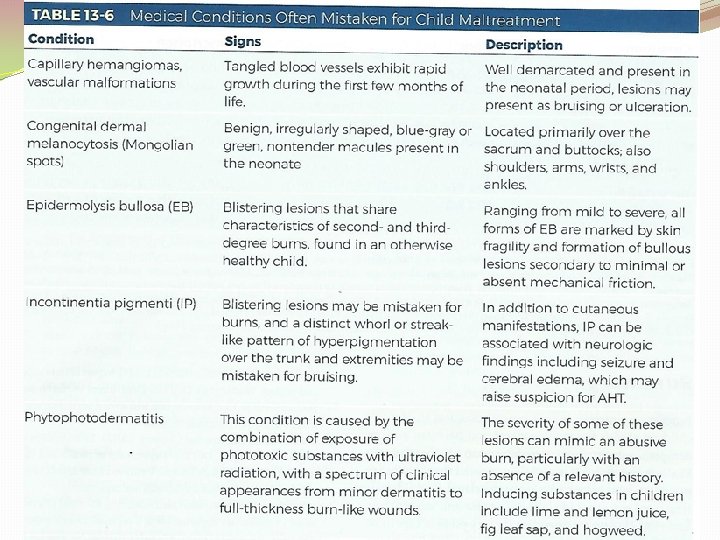
Burns �Absent or inadequate explanation �Hot water as agent �Immersion scald �Bilateral/symmetric burn pattern �Clear margins � 10% or more of TBS affected �Full-thickness �Coexistent injuries
Inflicted Burns �Generally �Deeper than unintentional �More severe because of delay of care �No evidence of, “pull over” spill, tend to have a typical and predictable burn pattern �Unintentional have irregular margins, and non-uniform depth, downward flow pattern �Inflicted immersion characteristically sharp lines of demarcation �Often involve genitals and lower extremities in symmetric distribution – “sock” or “glove” pattern �History, number of burns, continuity may warrant further investigation � 33% of children with burns have positive skeletal surveys
Unintentional vs Intentional Pull over spill Burn Stocking / Glove Burn
Bite Marks �May be round, or oval �With bruising �Wounds of various shapes surrounding bruise �Clearly defined teeth impressions �Important evidence if recent and obviously not cleaned or older and infected �Local law enforcement or forensic nurse experts should be ideally involved �Photographic and DNA evidence
Evaluation of Child Maltreatment �Screening is systematic process �AAP – The evaluation of Suspected Child Physical Abuse helps guide a facility in developing such a protocol �Provide relaxed environment to obtain history from children and caregivers – open ended questions �Comprehensive and accurate documentation- using exact quotes - photographs
Nursing Interventions �Document for Court �provide the facts- avoid personal opinions �Descriptive documentation gives reader most accurate picture of what is observed �Exact words of patient and caregivers in quotes, even in slang, violent terms, or vulgar terms �Evidence �Defined as data presented to a court or jury to prove or disapprove a claim (physical, words spoken, observations) �Safeguard evidentiary materials �Avoid cutting through blood, stains, splatter, or holes made by projectiles; cut along seams �Know jurisdictional laws regarding evidence collection and chain of custody �REMEMBER: The well-being of a patient takes precedence over forensic evidence collection
Mandated Reporting �All involved in child care (physicians, nurses, teachers, daycare workers, police) are mandated reporters required by law in all states – report suspected abuse or neglect �Fear of over-reporting in an already overburdened system may be a deterrent �Confidence and self-efficacy in ability to recognize child maltreatment may assist healthcare providers to take appropriate action and report suspicions
Summary �Nurses crucial position to identify children at risk for maltreatment �Performing a more comprehensive evaluation to determine whether they are in a safe situation �Those educated related to this issue more likely to recognize & report their findings �Healthcare providers at every point of care must effectively identify and intervene on behalf of children who deserve a life free from abuse