TENTSTP TrainTheTrainer TTT Workshop Senior Trainer Date TENTSTP
 Workshop Senior Trainer: Date:")






















")





, Ozer et al (2003)")

 – 7461 respondents –")

 • 21, 425 adults")






 Trauma (UCS)/ Reminders (CS) XS initial (UCR) or later")












 –")



")
















 Effect Size SMD & 95% CIs")
 Effect Size SMD & 95% CIs")

")
")



























- Slides: 107
TENTS-TP Train-The-Trainer (TTT) Workshop Senior Trainer: Date:
TENTS-TP TTT Workshop • Aim of the TTT workshop • Why TTT? • Why are you here? • What are your learning objectives?
Introductions • Split into pairs and ask your partner: - What is your job title? - What is your interest in this topic? - Why do you want to train as a trainer? • Then convey this information back to the whole group
Timetable Day I Workshop opening and introduction Pre-workshop questionnaire Warm-ups and icebreakers Learning expectations and ground rules Background on TENTS and TENTS-TP Brief overview of the Curriculum Break Detailed overview of the Curriculum (incorporating methods for training trainers (e. g. use of role play, public speaking etc) Lunch Detailed overview of the Curriculum continued Break Detailed overview of the Curriculum continued Questions and answers session Wrap –up
Timetable Day 2 Feedback on Day 1 Detailed overview of the Curriculum Break Detailed overview of the Curriculum Exploring own attitudes and values Introduction to TENTS-TP website and resources Lunch Introduction to methods for training trainers/health and social care professionals Planning future workshops Monitoring, evaluation and supervision Break Questions and answers session Post-workshop questionnaire Wrap-up, closing and distribution of certificates
Introduction to the TENTS-TP Adopted Guidance • Describe the core principles of the guidance • Describe the core principles of governance and strategic policy • Describe the stepped model of care
The TENTS Project • The European Network for Traumatic Stress • EU funded May 2007 - May 2009 • Developed the TENTS post-disaster psychosocial care guidelines • Established a growing network • www. tentsproject. eu
The TENTS – TP Project • The European Network for Traumatic Stress - Training & Practice aims to: – expand develop the TENTS network – connect to other important European initiatives – implement evidence-based interventions in the field of trauma and recovery
NATO Guidance • Governance and strategic policy: • NEEDS BRIEF SUMMARY OF NATO GUIDANCE AND HOW IT CAME ABOUT
NATO-TENTS Guidance • Combining the NATO and TENTS principles • Guidance based on pieces of work conducted for the North Atlantic Treaty Organisation (NATO) and the European Union (EU) – the TENTS programme • Brought together common principles and recommendations to provide a consensus of opinion. http: //www. healthplanning. co. uk/principles/
TENTS- TP Core Curriculum • 13 modules with learning outcomes • Based on the current evidence base • Curriculum is available on the TENTS-TP website: http: //www. tentsproject. eu/index. jsp? USMI D=120 • Additional resources at www. estss. org
Psychosocial Resilience • Define resilience in the context of trauma. • Describe interventions/approaches that foster resilience • Describe post traumatic growth
Two paradigm shifts of the last 30 years • Shift in: – Focus on individual persons to – Focus on persons within families, communities, workplaces, schools and groups of strangers • Shift from: – Viewing people’s responses to trauma as a secondary disaster in which people are hapless victims, unpredictable, and/or driven by competition and panic to – Viewing people as innovative problem-solvers
Resilience to trauma • Interacting capacities and capabilities that drive resilience to trauma: – Social relationships and capital – Economic – Institutional – Infrastructure – Community – Psychosocial
Trajectories of response Trajectory Nature of trajectory Resistance A stable or maintained pattern of no or mild experiences of stress Resilience Initially, moderate to severe experiences of stress (distress) followed by steep decrease Recovery Initially, moderate to severe experiences of stress (distress) followed by gradual decrease Relapsing +/or remitting problems Initially, moderate to severe experiences of stress (distress) followed by patterns that are not stable over time Delayed dysfunction No, mild or moderate experiences of stress that are not accompanied by dysfunction initially, but dysfunction follows later Chronic dysfunction Medium and long-term experiences of moderate to severe stress that is accompanied by dysfunction or occurrence of disorder(s) that are stable over time
Resilience, resistance and recovery
Psychosocial Resilience • Distress or Disorder? Discuss in groups how you think you would differentiate between these two.
Distress or disorder? • Distress – Implies an external and usually temporary cause of great physical – or mental strain and stress Emotional responses that: • are referable to the advent of a stressor • are proportionate to the impact of the stressor • tend to improve or resolve withdrawal of the stressor • Disorder – Feelings and dysfunction that: • are disproportionate to the anticipated impact of the stressor • persistent after removal of the stressor • taken to indicate an anatomical, physiological or psychological abnormality of a particular person
• Personal and collective psychosocial resilience – “a person’s capacity for adapting psychologically, emotionally and physically reasonably well and without lasting detriment to self, relationships or personal development in the face of adversity, threat or challenge” Williams, 2007 • Collective – “Collective resilience refers to the way crowds of people express and expect solidarity and cohesion, and thereby coordinate and draw upon collective sources of support and other practical resources adaptively to deal with adversity” Drury, 2009
Psychosocial resilience • Important criterion for evaluating community or societal resilience • Distress is a highly sensitive indicator of environmental stress - trauma and adversities • Within limits, distress is to be anticipated and is normal • When distress is highly prevalent, severe, or persistent, it points to problems, dysfunction
Posttraumatic growth • • • Trauma does not just tear down Crisis common source of positive change Identity, philosophy, and goals Relationship and social network Empathy Vulnerability and receptiveness of help
Introduction to Traumatic Stress Reactions and Disorders • Describe the range of normal reactions following traumatic events and their natural course. • Describe problematic reactions following traumatic events including PTSD and other common disorders according to the DSMIV and ICD-10. • Describe the basic epidemiology of traumatic stress disorders
Traumatic stress reactions and disorders • What is the normal psychological response to a traumatic event? • What is post traumatic stress disorder? • Do any other psychiatric disorders occur following traumatic events?
Natural Course of Traumatic Stress Foa & Rothbaum (1990)
Distress Natural Course of Traumatic Stress Time Creamer et al, 2007
Post Traumatic Stress Disorder • • Exposure to traumatic event Re-experiencing Avoidance and numbing Increased arousal Clinically significant distress or impairment Acute 1 -3 months Chronic > 3 months
Other Possible Presentations • • • Normal reaction Acute stress disorder Pre-existing difficulties Anxiety Depression Adjustment disorders Substance misuse Psychosis Somatoform disorders Malingering
Co-morbidity • Present in > 50% cases • Commonest co-diagnoses – Major depressive disorder – Panic disorder – Other anxiety disorder – Substance abuse/dependence • NVVRS (Kulka et al, 1990) = 99% lifetime
Peritraumatic dissociation a state of limited or distorted awareness during and immediately after trauma.
Associated Factors Brewin et al (2000), Ozer et al (2003)
Trauma & PTSD prevalence Traumatic event: 50 -80% PTSD 7 -8%: women 10 -12 %, men 4 -6 % (Netherlands and US) (Kessler et al 1995, De Vries & Olff, JTS, 2009)
U. K. Prevalence • England Adult Psychiatric Morbidity Survey (2009) – 7461 respondents – 33. 3% traumatic event since 16 – 3% Trauma Screening Questionnaire +ve • NI Trauma, Health and Conflict Study (2008) – 1095 respondents – 66. 3% traumatic event in life, 50% conflict related – 4. 7% 12 month CIDI PTSD, 8. 5% lifetime
U. S. Prevalence • US National Co-morbidity Survey • > 5, 500 15 to 54 year olds • Trauma Exposure – 60. 7% M, 51. 25% F • Lifetime Prevalence – 10. 4% F, 5. 0% M, 6. 8% • 12 Month Prevalence – 3. 5% Kessler et al (1995 & 2005)
European Study of the Epidemiology of Mental Disorders (ESEMe. D) • 21, 425 adults nationally representative of six European countries (Belgium, France, Germany, Italy, the Netherlands and Spain) • PTSD life-time prevalence = 1. 9% (M=0. 9%; F= 2. 9%) • 12 month prevalence = 1. 1% (M=0. 5%; F=1. 7%)
Introduction to Traumatic Stress Reactions and Disorders • Explain the principles of theoretical basis of PTSD from neurobiological, psychological and social standpoints.
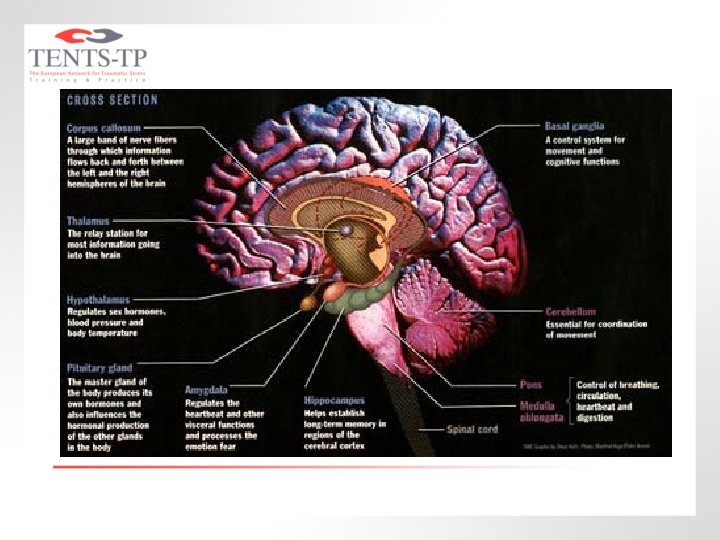
Questions • What areas of the brain are implicated in PTSD? • What neurophysiological changes occur in PTSD? – What are the key hormones/neurotransmitters?
The Amygdala in PTSD • Receives information about external stimuli • Determines significance of external stimuli • Significance triggers emotional responses including “fight, flight or freezing”
Neurobiology of PTSD • ? PTSD represents a failure of medial prefrontal/anterior cingulate networks to regulate amygdala activity resulting in hyperreactivity to threat
Hypothalamic- Pituitary. Adrenal Axis • Enhanced negative feedback • Low cortisol levels • Disinhibition of traumatic memory retrieval • Failure to contain sympathetic response
Question • What are the psychological and social theories of PTSD?
Positive Feedback Cycle (Pitman, 1989) Trauma (UCS)/ Reminders (CS) XS initial (UCR) or later (CR) stress hormone release Overconsolidation of memories Too much significance leads to too much remembrance
Dual Representation Model • Verbally accessible memories – easily verbally recalled and give rise to emotions related to the trauma • Situationally accessible memories – cannot be deliberately accessed and give rise to symptoms such as dreams and flashbacks Brewin et al, 1996
Cognitive Model • Traumatic memory induces a sense of current threat • Promoted by excessively negative appraisals of what happened Ehlers & Clarke, 2000
Social Factors • The existence of PTSD continues to attract some debate – ? culturally determined, understandable emotions to traumatic events are being pathologised • Social factors moderate response – Family, material loss, financial inc litigation, loss of role
QUIZ 1 1 2 3
QUIZ 2 1 1 2
QUIZ 3 • Where is cortisol produced? • What type of surge is there after a traumatic event? • What areas of the brain are thought to inhibit the amygdala? • What is the unconditioned stimulus in PTSD?
Early Intervention following Traumatic Events • Describe the commonly used approaches to acute and early intervention following traumatic events and the rationale behind them including interventions for everyone, targeted interventions and the timing of them. • Describe specific interventions including critical incident stress debriefing, psychological first aid, critical incident stress management, trauma risk management, supportive counselling and trauma focused cognitive behavioural therapy. • Discuss the current evidence base for the effectiveness of early interventions following traumatic events.
What is early intervention? • General concept for psychosocial and mental health responses to mass trauma • Broad multiagency responses • Specific/formalised interventions: – – – Psychological first aid (PFA) Supportive counselling (SC) Trauma risk management (TRi. M) Critical incident stress debriefing (CISD) Trauma-focused Cogn. Behav. Therapy (TB-CBT)
Sing. Ie Session Early Intervention • No certain clinical effects for any intervention tested in 12 RCTs • Single session debriefing may cause harm to some individually debriefed individuals • No convincing evidence emerging for group debriefing
CBT V waitlist acute distress from 2 weeks • Clinician administered SMD = -0. 61 [-1. 10, -. 13] • Self report SMD = -0. 84 [-1. 72, 0. 04] Roberts et al, 2009
CBT v waitlist Acute PTSD • Clinician administered SMD = -1. 22 [-1. 65, -0. 78] • Self report SMD = -1. 68 [-2. 34, -1. 01] Roberts et al, 2009
Wait and Target - CAPS Ehlers et al, 2003
Early Pharmacological Interventions • No convincing evidence – Propranolol versus placebo (two studies) – Gabapentin versus placebo (one study) – Temazepam versus placebo (one study) – Escitalopram versus placebo (one study) • Limited evidence of benefit – Hydrocortisone versus placebo (one study)
NICE Guidelines for Early Intervention • Offer immediate practical, social and emotional support • Don’t debrief individuals • Consider symptomatic pharmacotherapy • Watchful waiting • Trauma focused CBT for acute PTSD
Screening and Information • Describe the evidence base for screening for post traumatic disorders. • Describe the evidence base for providing information and psychoeducation following traumatic events.
Screening • Overall mean diagnostic efficiency of 86. 5% but false positives a problem if prevalence low • Ideal instrument has fewer items and simple to administer and score • Trauma Screening Questionnaire (TSQ) and SPAN fared as well as any • TSQ ten yes/no questions • SPAN four questions but more complex (Brewin, 2005)
TSQ (Brewin et al, 2002)
Information • There is a very, limited evidence base for providing information and/or psychoeducation following traumatic events. • Ehlers et al (2003) and Turpin et al (2005) found no effect • No definite evidence of harm • Further work needed but most agree should be available
Assessment, Formulation and Treatment Planning • Describe the essential components of a full assessment of a psychologically traumatised individual. • Describe the principles of formulation and treatment planning. • Discuss the importance of understanding an individual’s presentation before commencing treatment.
Question • How do you assess someone who has been psychologically traumatised?
Assessment • Full history, examination, other information – Biological, psychological, social, risk • Standardised measures – CAPS, IES-R, PSS-SR • • No assumptions NB range of presentations Explore history of trauma with examples Re-experiencing and hyperarousal screen – Trauma Screening Questionnaire
Formulation • • Brief description of issues Differential diagnosis Predisposing factors Precipitating factors Maintaining factors Further information required Management Plan
Management Planning • Consider evidence base • Involve individual – NB choice • Ensure address all factors elicited – Biological – Psychological – Social – Risk
Psychological Treatment of PTSD • Describe theoretical basis underlying the commonly used trauma focused psychological treatments including exposure therapy, cognitive behavioural therapy, eye movement desensitisation and reprocessing and brief eclectic psychotherapy. • Describe non trauma focused approaches including stress inoculation training, anxiety management, psychodynamic therapy and hypnotherapy. • Discuss the current evidence base for the effectiveness of psychological treatment approaches for PTSD.
Questions • What approaches are used to treat chronic PTSD? • Are any treatment approaches effective?
TFCBT Approaches • Exposure – The therapist helps the PTSD sufferer to confront their traumatic memories (written or verbal narrative, detailed recounting of the traumatic experience, repetition). – In vivo repeated exposure to avoided and fear -evoking situations that are now safe but which are associated with the trauma.
Script Preparation
TFCBT Approaches • Cognitive Therapy – Focus on the identification and modification of misinterpretations that lead the PTSD sufferer to overestimate current threat (fear). – Also focus on modification of beliefs related to other aspects of the experience and how the individual interprets their behaviour during the trauma (eg issues concerning guilt and shame).
Cognitive Restructuring • Video Clip
Non-TF CBT Approaches • Stress Management – Relaxation training. – Breathing retraining. – Positive thinking and self-talk. – Assertiveness training. – Thought stopping. – Stress inoculation training.
Breathing Retraining • Video Clip
EMDR • Standardised, trauma-focused, procedure with several elements, always involving the use of bilateral physical stimulation (eye movements, taps or tones), hypothesised to stimulate the individual’s own information processing in order to help integrate the targeted event as an adaptive contextualised memory.
EMDR
Psycho. Rx Clinician Ratings (v wait list) Effect Size SMD & 95% CIs
Psycho. Rx Clinician Ratings (v wait list) Effect Size SMD & 95% CIs
Pharmacological Treatment • Describe theoretical basis underlying the commonly used pharmacological treatments • Discuss the current evidence base for the effectiveness of pharmacological treatments for PTSD
Clinician Ratings (v placebo)
Clinician Ratings (v placebo)
CAPS–SX Reductions in Means Davidson et al, 2006 x 2
NICE Recommendations • First line – Individual TFCBT or EMDR – Usually 8 -12 sessions, some 90 minutes • Second line – Alternative trauma-focused treatment – Drug augmentation • Other indications for drugs – Patient choice – Serious ongoing threat
Community Interventions • Describe the impact of traumatic events on communities. • Describe specific approaches to effective interventions for communities.
What are community-based interventions? • Activities that facilitate normalization of social, family and individual psychosocial functioning in a community affected by a disaster – Promote a sense of safety, self and community efficacy/empowerment, connectedness among community members, and increase hope in recovery of individuals and the community – Provide support and treatment to people with difficulties in family, work or social functioning
Circles of Vulnerability
Specific approaches to community interventions: • • Practical help given in an empathic manner Emotional support and initial reassurance Providing information Material assistance • • Employment Facilitating mutual support Psychosocial care interventions Memorial events and building monuments
* Psychiatric medication * Treatment of dysfunctional traumatized clients Level of * Individual, family, group counseling service * Loss, grief and worry work expertise * Psychological evaluation and referral * Social and life skills building groups * Self help and mutual support groups * Emotional support provisions by trained para-professionals * Guidance in structuring free time * Networking (e. g. youth, elderly, special needs groups) * Family reunification * Training of care-providers and dissemination of skills and knowledge * Public awareness of “normal psychological reactions to abnormal situations” * Information on accessing other services, about legal status, missing ones * Facilitating basic social structures, institutions, roles and responsibilities Number of clients served / allocation of resources Pyramid of community psychosocial intervention (Ajduković, 1997; Ajduković & Ajduković, 2003)
Complex PTSD • Describe the common presentations of complex PTSD sufferers. • Discuss theoretical basis as to why alternative management approaches may be beneficial for complex PTSD compared to simple PTSD. • Describe the current evidence base for the effectiveness of treatments for complex PTSD.
Question • What is complex PTSD? • What are the key symptoms and difficulties? • Which individuals are most vulnerable to developing complex PTSD?
Multiply Traumatised • Population versus diagnosis – E. g. adult survivors of CSA and other abuse, asylum seekers, refugees, IDPs, military veterans, domestic violence • Many presentations – Often complex, interpersonal relationship and affect regulation difficulties characteristic • Physical, mental health and social issues
Complex PTSD • • No such diagnosis PTSD plus X Multiple Traumatised under age of 26 Developmental impact Attachments impact Affect Regulation
Management • • Full biopsychosocial assessment Multiagency, multidisciplinary Agreed management plan Phased approach – Usually social, psychological and pharmacological elements
STAIR-MPE • A Phase-Based Treatment for the Multiply Traumatized • Phase I: Skills Training in Affective and Interpersonal Regulation (STAIR) • Phase II: Modified Prolonged Exposure (MPE) • 8 x one hour of each • Designed for women with PTSD related to childhood sexual abuse Cloitre et al, 2002
Grief • Describe normal grief reactions. • Describe pathological/traumatic grief reactions. • Describe the current evidence base for facilitating the grieving process.
Children and Families • Describe the normal and pathological reactions that children may experience following traumatic events and their age and developmental specific mechanisms. • Describe the basic epidemiology of traumatic stress disorders in children and adolescents • Discuss the current evidence base for the prevention and treatment of PTSD in children.
PTSD among children and adolescents • Studies among children who experienced specific traumas indicate that children may have higher prevalence rates of PTSD then adults in the general population • US National Survey of Adolescents: sixmonths prevalence: 3. 7% for boys and 6. 3% for girls (Killpatrick et al. , 2003)
Trauma and Danish adolescents • Danish national representative sample of 390 eight-grade students aged 13 to 15 • 87% of females and 78% of males were exposed to at least one event • Lifetime prevalence of PTSD (according to DSM-III-R) was 9% (5. 6% males and 12. 3% females) Elklit (2002)
Children treatment recommendations • TF-CBT adapted for age, circumstances, and level of development • Family involvement where appropriate • No good evidence for the efficacy of treatments such as drugs, play therapy, art therapy or formal family therapy
Emergency Responders • Describe the principles of appropriately supporting emergency responders • Describe the current evidence base for the effectiveness of interventions for emergency responders
Attitudes and Values • Split into groups of 3 or 4. • As a group, discuss your views on providing psychological versus pharmacological treatments for PTSD.
Exercise • In pairs, devise a 2 minute presentation summarising one of the modules from the curriculum and present to the group.
Teaching Techniques • Public speaking: - Use of interaction techniques with the audience - Movement in and around the audience - Appropriate duration of eye contact - Use of gestures - Use of humour - Speech intonation
Planning future workshops Write an action plan using the example checklists: • Two months or more before the workshop • Two weeks before the workshop • One week before the workshop • One day before (or the morning of the training)
Monitoring, evaluation and refresher courses • Folder of activities Feedback reports Course evaluations Participant numbers • • • Assessment at the end of the training. Feedback from and assessment of new trainees Refresher course within two years of training
Supervision • Named Supervisor • Supervision sessions • Further support can be accessed via the TENTS-TP website: http: //www. tentsproject. eu/ • Update emails
Question session • How do you feel about the training? • Is there anything that you feel wasn’t covered in enough detail? • Do you feel ready to organise your own workshops?
Thank you for attending the TENTS -TP TTT Workshop