SYNCOPE Duka Glava Department of Cardiology University Hospital

 • Affected 3")

 b) c) There are three basic disorders: syncope nonsyncopal")
 Syncopa • Syncope develope because of abrupt lowering of cardiac output, with cerebral")
 Nonsyncopal loss of consciousness • Cause is not general cerebral hypoperfusion • There")
 Disorders that imitate loss of consciousness • Basically it is not loss of")






-a synus node dysfunction, • Causing alternating")

 • Between attacks,")
: sick sinus syndrome, AV block II/III degree, VT, PSVT,")
: sick sinus syndrome, AV block II/III degree, VT, PSVT,")











-portable ECG detect heart rhythms, arrhytmiae •")
 syncope • for returning blood to the brain-positioning the person")


- Slides: 36
SYNCOPE Duška Glavaš Department of Cardiology University Hospital Split
SYNCOPE • syncope (gr. sinkoptein-fall unconscious, fainting, passing out, . ) • Affected 3 -6/1000 people every year • 1 -3% of visitis to emergency unit • 1/3 medical students • More common in older and females
SYNCOPE-Differential diagnosis • Central nervous system ischaemia-inadequate supply of oxygenated blood in the brain, verebro-basilar insuff. • Vasovagal-response to “triggers” • Blood pressure-Orthostatic hypotension (movement from lying to standing position) • Cardiac • Other reasons
Disorders of consciousness: • a) b) c) There are three basic disorders: syncope nonsyncopal disorders of consciousness disorders that imitate disorders of consciousness
a) Syncopa • Syncope develope because of abrupt lowering of cardiac output, with cerebral ishaemia • Appearance is abrupt, duration short (~20 s), with complete recovery. Syncope is followed with hypotensia • Prodromal signs: dizziness, weakness, difficulties with vision, nausea, sweating, . • After syncope possibly is amnesia, cramps, incontinence • PRESINKOPA: existing of prodromal signs, without loss of consciousness
b) Nonsyncopal loss of consciousness • Cause is not general cerebral hypoperfusion • There are other mechanisms: epilepsy, hypoglicaemia, hypoxia, intoxication, .
c) Disorders that imitate loss of consciousness • Basically it is not loss of consciousness • Cardiovascular collapse: abrupt loss of circulation bacause of heart or peripheral vascular reasons; spondaneus recovery • Psychiatric disorders: hyperventilation syndrome, hysteria, catalepsy, drop attacks, .
Reflex syncope • VASOVAGAL: trigger is orthostatic reason • Ofen when somebody longer stay (in warm enviroment, . ) • Because of gravitation and filtration of fluid, 15 -20% volume is moved below diaphragm, results in ↓ vein inflow and stroke volume, with activation of reflex
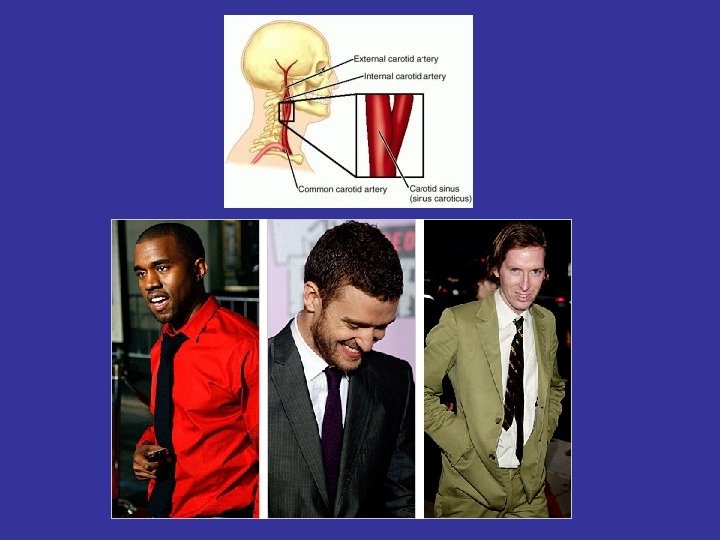
Reflex syncope - SITUATIONAL: afferent arm of reflex is located in different organs (bladder, bowels, bronchi, central nerve system, during deglutition); painfull unpleasant stimulus - baroreceptor of sinus caroticus (carotid sinus syncope) - “triggers” shaving, moving of head, .
Carotid synus syncope • In healthy persons, pressure of sinus caroticus leads to ↓ heart rate and blood pressure • In older, sinus could be hypersensitive and develop bradicardia and hypotension • Term “Carotis synus syncope” we used for patients with abnormal replay to massage, and when patients have often symptoms (syncope, dizziness) provoked with “triggers” (tight collar)
Ortostatic syncope • Consequence of primary or secundary dysfunction of autonomic nerve system • Primary dysfunction-conseguence of degenerative neurologic disorders (Shy-Dragerov sy, Bradbury. Eglestonov sy), synkope without compensation mechanisms (as ↑puls), often progressive course, of disease, , . • Secundary-consequence of diabetic, alc, and other neuropathy, multiple sclerosis, drugs, .
Ortostatic hypotension • Hypovolemia have different reasons: • Ortostatic hypotension could be consequence of bleeding, diarrhae, vomitting, diuretics, sweating, . • Often after longer standing, after weight loss, in older and weaker persons, after sympatectomia, . • “Triggered” with endocrine disorders: hypoglicaemia, feocromocytoma, .
Cardiac syncope • Morgagni-Adams-Stokes syndrome: abrupt loss of consciousness because of interruption of circulation in the brain; block, seizures, distrubance of pulse and reapiration • asystolia of 10 s-unconsciousness; • 10 -40 s-cramps with apnea and cyanosis; • >5 min could be fattaly outcome
Cardiac syncope • Sick sinus syndrome (sy tachycardiabradicardia)-a synus node dysfunction, • Causing alternating tachycardia-bradycardia • Often there is a long pause asystole between heart beat
Cardiac syncope • Subclavian steal syndrome, arises from retrograde flow of blood in the vertebral artery or the internal thoracic artery, due to a proximal stenosis of subclavian artery • Various medications, such as beta-blockers may couse bradicardia and syncope
Cardiac syncope • Cardiac syncope are usually sudden (without prodromal sign) • Between attacks, patients usually fiiling good • the mean reasons of cardial syncopa are: arrhythmias and conduction disturbances (ventricular asystolia, AV block, VT, . )
Cardiac syncope • ARRHYTHMIAE (brady/tahy): sick sinus syndrome, AV block II/III degree, VT, PSVT, Sy WPW, longer/ shorter QT, Sy Brugade, drugs • HR<30/min, compansation is not enough for cerebral perfusion • HR>180/min diastole is to short for filling of ventricul • Other “triggers”: anaemia, ishaemua, valve disorders, CV insufficiency
Cardiac syncope • ARRHYTHMIAE (brady/tahy): sick sinus syndrome, AV block II/III degree, VT, PSVT, longer/ shorter QT, Sy Brugade, drugs • HR<30/min, compansation is not enough for cerebral perfusion • HR>180/min diastole is to short for filling of ventricul • Other “triggers”: anaemia, ishaemua, valve disorders, CV insufficiency
Cardiac syncope: PSVT
Cardiac syncope: VT
Cardiac syncope: VT and VF
Cardiac syncope • Structural heart disease: -stenotic valve disorders -opstructive cardiomyopathy, -acute coronary syndrome, -aortic dissection, pulmonary embolism, myxoma, tamponade, heart failure, .
Syncope-heart failure
Syncope-Aortic dissection
Cardiac syncope • Aortic stenosis is related with strain • Reasons: lower vascular resistance and lower stroke and minute volumen • Transient tachyarrhytmiae are often reasons for syncope in aortic stenosis • Ventricular asystolia is consequence of hypersensitive baroreceptors (aorta, LV)
Cardiac syncope • Aortic stenosis is related with strain • Reasons: lower vascular resistance and lower stroke and minute volumen • Transient tachyarrhytmiae are often reasons for syncope in aortic stenosis • Ventricular asystolia is consequence of hypersensitive baroreceptors (aorta, LV)
Cardiac syncope • intracardial formation could, dependent of moving of the body, stimulate syncope (myxoma) • syncope in mitral stenosis-related to embolism and tachyarrhythmiae • In primary pulmonary hypertension, mechanism is the same as in aortic stenosis • Syncope in Falloth tetralogy is related to strain (↑ R-L shant and artery hypoxia, with ↓ vascular resistance)
Diagnostic approach • Lab. tests: Hemoglobin count may indicate anemia; potassium, troponin, . • ECG: a. fibrillation, blocks, infraction, VT, . • For people with uncomplicated syncope with normal neurological exam, CT or MRI in not indicated • Carotid artery problems are unlikely to cause syncopa (ev. carotid ultrasound)
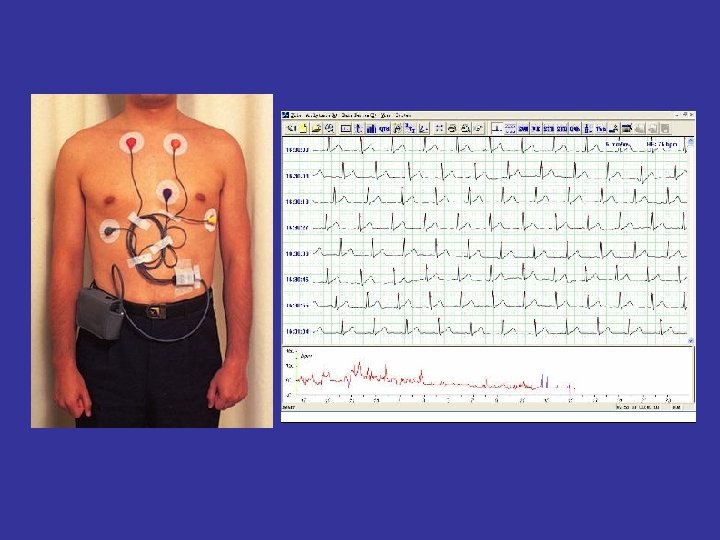
Diagnostic approach • Holter (24 h ECG monitoring)-portable ECG detect heart rhythms, arrhytmiae • Tilt table test: performed to elict orthostatic syncope secondary to auton. Dysfunction • Insertable cardiac monitor (loope recorder), to 28 -36 months, device continously monitors the rate and rhythm • San Francisco syncope rule-people with higher risk of serious reason(dilatative HF, .
Tretament: Vasovagal, orthostatic (hypotension) syncope • for returning blood to the brain-positioning the person on the ground, with legs elevated • or leaning forward and the head between the knees for at least 10 -15 min • cool and quiet place
Tretament: Cardiac syncope • • depends of reasons tachyarrhytmiae-PSVT/a. fibrill=β-blockers, bradyarrtyhmiae-a. fibrill, blocks=pacemaker VT/VF=amiodarone, implantable cardioverter-defibrillators (ICD)
Thank you!